
Abstract
Regional cerebral blood flow (CBF) was studied with O15-water positron emission tomography and anatomic region-of-interest analysis on coregistered magnetic resonance in patients with idiopathic (n = 12) and secondary (n = 5) normal pressure hydrocephalus (NPH). Mean CBF was compared with values obtained from healthy volunteers (n = 12) and with clinical parameters. Mean CBF was significantly decreased in the cerebrum and cerebellum of patients with NPH. The regional analysis demonstrated that CBF was reduced in the basal ganglia and the thalamus but not in white matter regions. The results suggest that the role of the basal ganglia and thalamus in NPH may be more prominent than currently appreciated. The implications for theories regarding the pathogenesis of NPH are discussed.
Normal pressure hydrocephalus (NPH) is in part a disorder of the cerebrospinal fluid (CSF) circulation that is characterized clinically by gait, cognitive, and urinary disturbances. The pathophysiology of NPH and the criteria for CSF shunting remain controversial. By analogy with experimental hydrocephalus, it has been proposed that cerebral blood flow (CBF) in general and periventricular white matter CBF in particular may be reduced in NPH, changes which are reversed in patients who respond to shunting. We have recently reviewed these studies, which include some 631 cases (Owler and Pickard, 2001). Although a variety of techniques have been utilized, including 133Xenon clearance, stable xenon computed tomography (CT), single photon emission computed tomography (SPECT), and positron emission tomography (PET), very little consensus exists, possibly because the technology had insufficient resolution, and the patients were poorly characterized clinically. We have studied global and regional CBF in NPH patients using 15O-labeled water PET combined with accurate magnetic resonance (MR) coregistration.
METHODS
Patients
We report 17 patients (age 69.6 ± 9.8 years; 8 men and 9 women) with NPH who were referred to the CSF Clinic at Addenbrooke's Hospital. Twelve patients presented with idiopathic NPH and five with NPH secondary to meningitis after a head injury, intracerebral hemorrhage, meningitis, surgery for removal of meningioma, and basilar artery ectasia. In addition, one of the idiopathic NPH patients also had Steel-Richardson syndrome.
The criteria for inclusion were gait disturbance, with or without cognitive changes or urinary incontinence, dilated ventricles on CT, and normal CSF pressure measured via an Ommaya reservoir. All patients were assessed clinically using an NPH scale modified from Larsson et al. (1991), which assessed gait (0, normal; 1, insecure; 2, insecure [cane]; 3, bimanual support; 4, aided; 5, wheelchair), living condition (0, independent; 1, at home with assistance; 2, retirement home; 3, nursing home; 4, hospital), and urinary symptoms (0, nil; 1, present). This resulted in a score of up to 10 points as well as a gait score. In addition, as a measure of overall function, we recorded a modified Stein-Langfitt score (0, no neurologic deficit and able to work; 1, minimal deficit and able to function independently at home; 2, some supervision required at home; 3, custodial care required despite considerable independent function; 4, no capacity for independent function). The degree of periventricular white matter hyperintensities were determined from T2-weighted MR images, and a score from 0 to 4 points was assigned to each patient (0, no white matter hyperintensities; 1, minimal white matter intensities; 2, capping of frontal and/or occipital horns of the lateral ventricles; 3, almost continuous white matter hyperintensities from frontal to occipital horns; 4, continuous white matter hyperintensities from frontal to occipital horns).
Patients with a provisional diagnosis of NPH who were suitable for further treatment underwent insertion of a frontal Ommaya reservoir. After a postoperative period of at least 2 days, a computerized CSF infusion study (Czosnyka et al., 1996) was performed to characterize the CSF dynamics including the resistance to CSF absorption (Rcsf). Patients with an increased Rcsf who were medically suitable underwent CSF ventriculoperitoneal shunting.
Control group
The control group consisted of 12 volunteers (mean age: 42.8 ± 9.8 years) who underwent both magnetic resonance imaging (MRI) and PET scanning in the same manner as the patient group. All volunteers were healthy with no history of either cardiovascular or neurologic abnormalities or disease.
PET and MRI scanning
PET scanning was performed on a GE Advance scanner at the Wolfson Brain Imaging Center. A radial arterial line and peripheral venous line were inserted. The patient's Ommaya reservoir was accessed to monitor CSF pressure throughout the procedure. The patient was positioned supine on the scanner table and encouraged to lie quietly in a darkened room. A 10-minute transmission scan was performed using two rotating 68Ge/68Ga rod sources (approximately 600MBq total) to correct for photon attenuation. An intravenous infusion of 800 MBq of O15-labeled water was then delivered to the patient over 20 minutes; after a 10-minute build-up period to achieve tracer steady state, PET data was acquired in 3D mode in two contiguous 5-minute frames. Arterial blood samples were taken at 10, 15, and 20 minutes into the infusion to monitor blood gases (including Pa
In addition, a volumetric 3 Tesla SPGR MRI scan (voxel size: 1 × 1 × 1 mm) of the brain was obtained on the same day as the PET scan in all of the control subjects and 14 of the 17 patients; three patients were unable to tolerate the MR scanner because of claustrophobia. The PET and MR images were coregistered using SPM-99 and CBF maps (voxel size 2.34 × 2.34 × 4.25 mm) were calculated using standard kinetic models (Frackowiak et al., 1981) (PETAN2001, Dr. Piotr Smielewski, Cambridge). The spatial resolution of the CBF maps is approximately 6 mm.
Analysis
For those subjects who had undertaken an MR scan, global CBF was assessed by drawing regions-of-interest (ROIs) on the coregistered MR images. For the cerebrum and the cerebellum, these regions were outlined with AnalyzeAVW using a combination of computer threshold drawing and manual correction. CSF spaces and large vessels were excluded from the ROIs. The process was repeated for each slice. For each ROI, a mean CBF was calculated based upon the entire ROI volume. In this way, a true mean CBF for the ROI was obtained, and the overall mean was not artificially affected by the size of the ROI. For the three patients without an MR scan, global ROIs for the cerebrum and cerebellum were drawn using AnalyzeAVW directly on the CBF maps (Fig. 1).
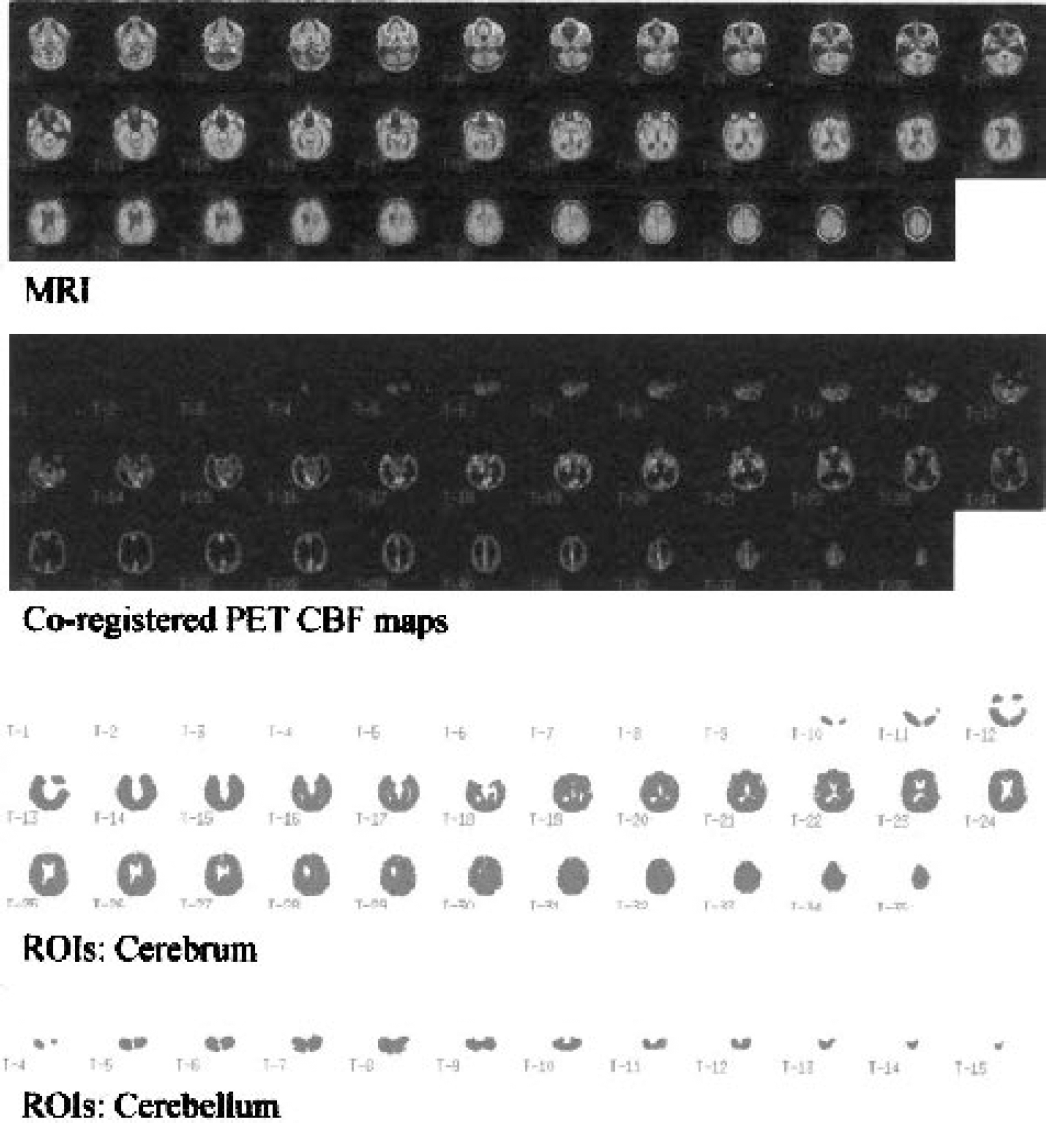
Coregistered MR images, PET CBF maps, and global ROIs for the cerebrum and cerebellum of a patient with NPH. MR, magnetic resonance; PET, positron emission tomography; CBF, cerebral blood flow; ROIs, regions of interest; NPH, normal pressure hydrocephalus.
The regional CBF results were obtained by manually placing small circular ROIs (each 15 voxels in size) bilaterally within anatomic regions on the slices of the MR scan where that structure was visible. This was performed for the frontal, occipital, temporal, and parietal white matter regions, as well as the thalamus, head of caudate, and the putamen (Fig. 2). Care was taken to place ROIs away from anatomic boundaries so as to minimize partial volume contamination of the ROI by other structures with different CBF. A regional CBF analysis could not be accurately performed in the three patients for whom there were no coregistered MR images. Therefore, results for the regional CBF analysis are based upon 11 patients with idiopathic NPH and 3 patients with secondary NPH.
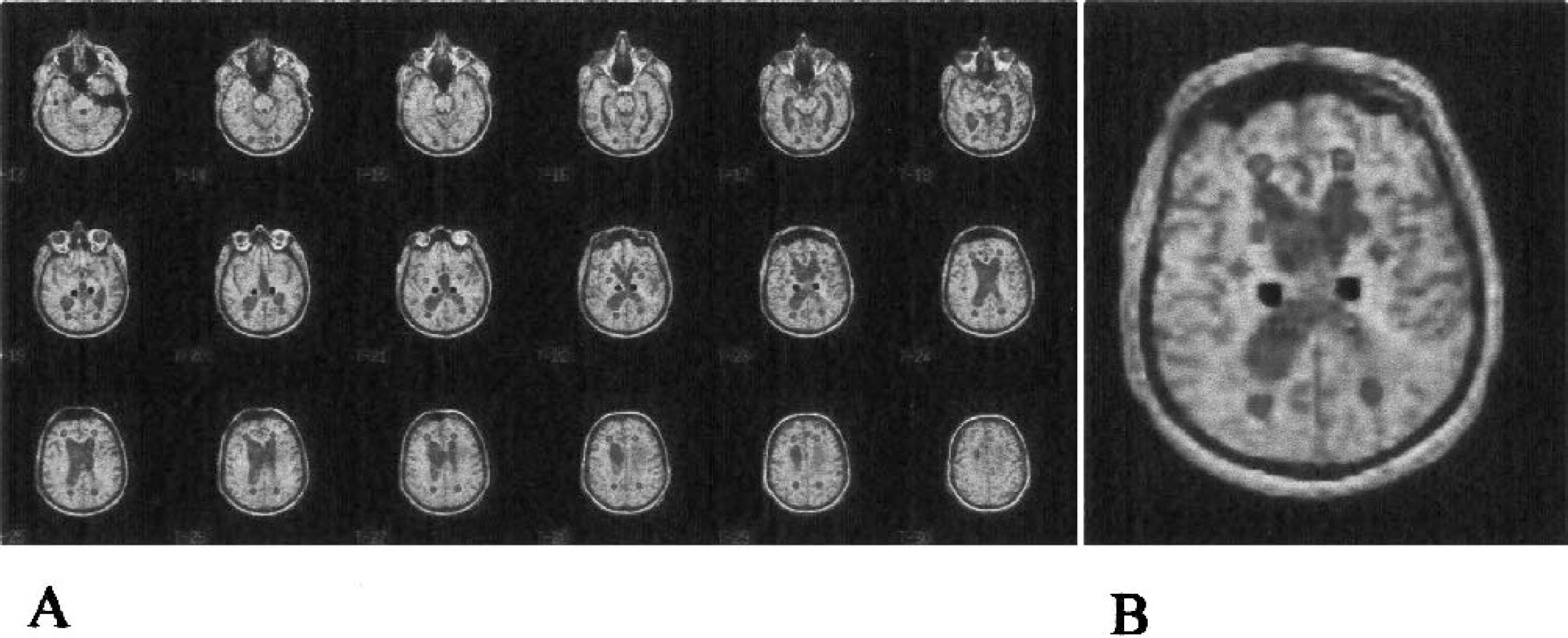
(A) Anatomic ROIs for the white matter and deep gray matter regions drawn directly onto coregistered MR images of a patient with NPH. (B) Illustrative MR image with multiple regional ROIs. ROIs, regions of interest; MR, magnetic resonance; NPH, normal pressure hydrocephalus.
The mean CBF values for global and anatomic regions were compared between patient groups and the control group using the Mann-Whitney U test. The preoperative NPH, gait, and modified Stein-Langfitt scores were compared with the mean for each region using Spearman rank order correlation.
All patients, relatives, and control subjects involved in the study gave informed consent. The study was performed with the approval of the Cambridge Local Region Ethics Committee (96/172, 96/209) and the UK Administration of Radioactive Substances Advisory Committee (083-2050(14649), 083-2050(10170)).
RESULTS
CSF infusion study results
For the patients with idiopathic NPH the mean Rcsf was 21.1 ± 7.0 mmHg/mL/min (mean ± SD) and baseline intracranial pressure (ICP) was 10.6 ± 3.7 mmHg. The mean Rcsf in patients with secondary NPH was 16.5 ± 6.1 mmHg/mL/min, and the baseline ICP was 12.6 ± 2.3 mmHg.
Global CBF values
There was a significant (P < 0.0005) difference between the mean CBF for the cerebrum of the NPH group (24.8 ± 4.3 mL/100g/min) and that of controls (30.5 ± 5.2 mL/100g/min) (Table 1). When the idiopathic NPH was analyzed separately to the secondary NPH group, the difference remained with the mean CBF being significantly lower (P < 0.0001) in the idiopathic NPH group (24.0 ± 2.9 mL/100g/min) compared with the controls. The mean CBF for the cerebrum of the secondary NPH group (26.7 ± 6.7 mL/100g/min) was also lower than controls, but the difference was not statistically significant.
Analysis of mean CBF in global regions of interest
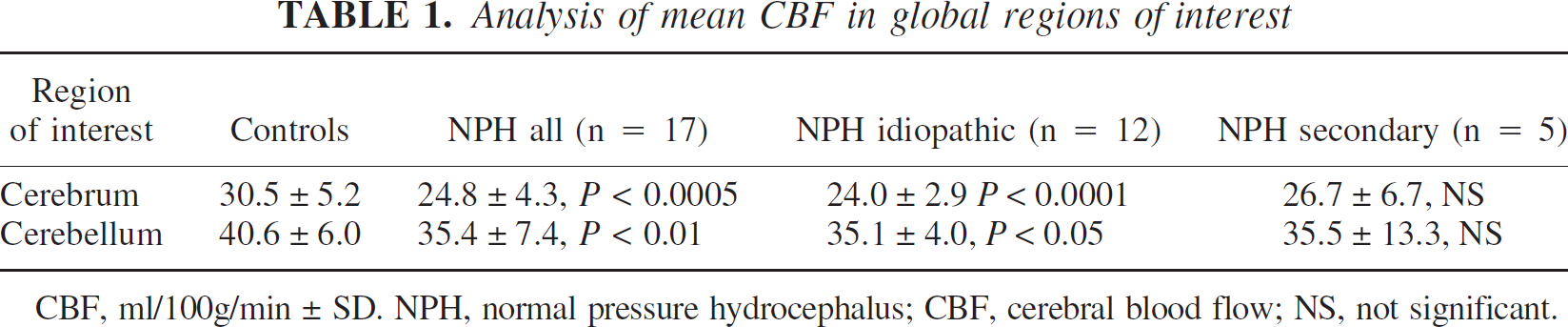
CBF, ml/100g/min ± SD. NPH, normal pressure hydrocephalus; CBF, cerebral blood flow; NS, not significant.
The mean CBF for the cerebellum was 35.4 ± 7.4 mL/100g/min for the NPH group compared with 40.6 ± 6.0 mL/100g/min in the control group. This difference was significant and remained so when the idiopathic group (35.1 ± 4.0 mL/100g/min; P < 0.05) was analyzed separately.
The mean arterial Pa
Regional CBF values
In the white matter regions, that is, frontal, temporal, parietal, and occipital regions, there was no difference between the whole patient group and controls. Furthermore, no significant difference became apparent when the idiopathic and secondary NPH groups were analyzed separately (Table 2)
Analysis of mean CBF in white matter anatomical regions
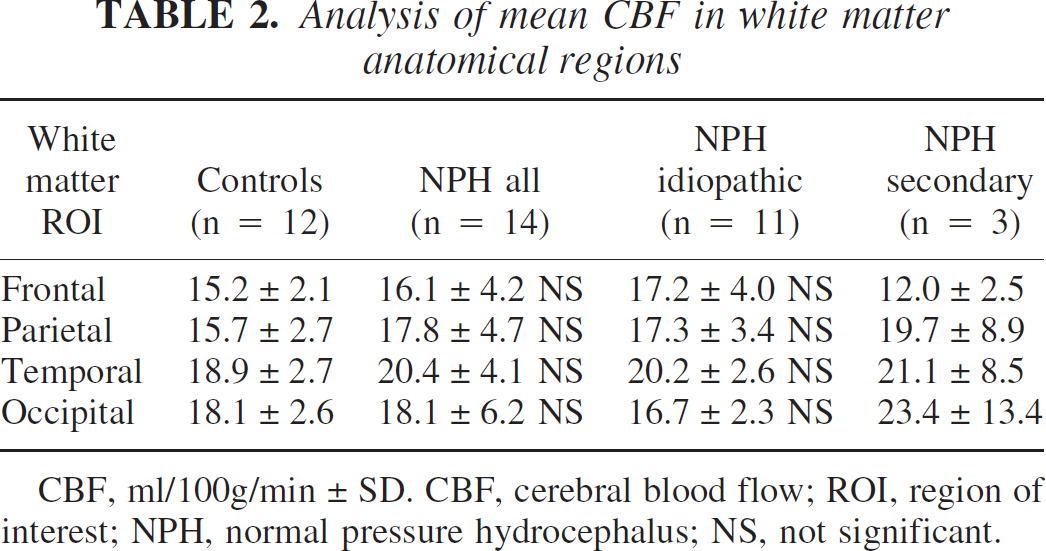
CBF, ml/100g/min ± SD. CBF, cerebral blood flow; ROI, region of interest; NPH, normal pressure hydrocephalus; NS, not significant.
Unlike the regional analysis of CBF in the white matter, marked differences in mean CBF between controls and NPH patients were demonstrated in the deep gray matter (Table 3). In the thalamus, the mean CBF of controls was 44.7 ± 5.7 mL/100g/min compared with 36.0 ± 7.5 mL/100g/min in the NPH patients (P < 0.005). The difference remained significant (P < 0.005) when the idiopathic NPH patients (35.6 ± 6.5 mL/100g/min) were analyzed separately. In the head of the caudate nucleus, the mean control CBF was 38.5 ± 7.0 mL/100g/min, which was significantly different to the NPH group as a whole (24.8 ± 6.5 mL/100g/min; P < 0.00005) and the idiopathic NPH group (23.6 ± 5.6 mL/100g/min; P < 0.00005). Mean CBF in the putamen of NPH patients (35.6 ± 8.3 mL/100g/min) was significantly (P < 0.05) lower than for controls (42.6 ± 7.1 mL/100g/min). Again, when the idiopathic NPH group (34.9 ± 8.3 mL/100g/min) was analyzed separately, the difference remained significant (P < 0.05)
Analysis of mean CBF in deep gray matter anatomical regions

CBF, ml/100g/min ± SD. CBF, cerebral blood flow; NPH, normal pressure hydrocephalus.
Relationship between clinical severity and CBF
Mean CBF values for the various regions were correlated (using correlation analysis) with clinical severity of NPH as assessed using the NPH, modified Stein-Langfitt, and gait scores. Because the clinical scoring of patients with secondary NPH reflected not only their NPH values but also their primary pathology and its consequences, patients with secondary NPH were excluded from the analysis. We could demonstrate no significant correlation between the CBF of individual patients and their NPH, gait, or modified Stein-Langfitt scores when all of the idiopathic NPH patients were analyzed. This was true of both the global and anatomic regions examined. However, the patient with coexisting Steel-Richardson syndrome had a relatively high mean CBF but clinically was in poor condition. When this patient was excluded from the analysis to obtain a group with purely idiopathic NPH, the following correlations became apparent. There was an inverse correlation between mean thalamic CBF and NPH score (R = −0.70; P < 0.05) (Fig. 3). In addition, the modified Stein-Langfitt score was inversely correlated with mean CBF in the putamen (R = −0.72; P < 0.05).
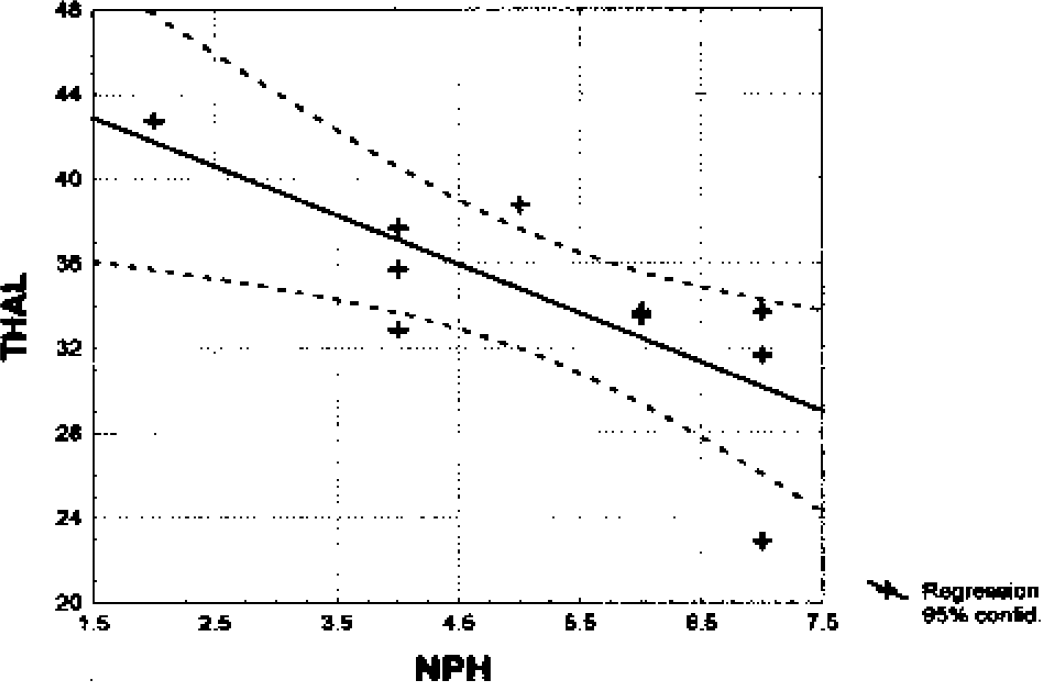
Correlation between NPH score and mean CBF in the thalamus of idiopathic NPH patients with MR coregistration, excluding the patient with Steel-Richardson syndrome (n = 10). This graph illustrates that for idiopathic NPH patients, those with lower mean CBF in the thalamus had higher, that is, poorer, levels of overall function using the NPH score. NPH, normal pressure hydrocephalus; CBF, cerebral blood flow; MR, magnetic resonance.
There were no significant correlations between the severity of periventricular white matter hyperintensities and CBF for any ROI, including white matter CBF.
DISCUSSION
The combination of PET scanning with anatomic ROI definition on coregistered MR for the study of CBF in patients with NPH has several advantages over other available technologies. The partition coefficient of 131Xenon may be affected by pathology, and study of its clearance is nontomographic and hence unable to study deep tissues accurately. Xenon CT is limited to measurement of CBF in only a few selected slices, and there are problems with quantification. SPECT CBF studies are limited by poor spatial resolution and difficulties in obtaining quantitative images. In addition, some SPECT tracers are metabolically active, and the results therefore reflect tissue metabolism as well as CBF. PET is a more accurate method of measuring CBF as the tracer (15O-water) is not metabolized, the spatial resolution is superior, and image quantification is more easily achieved. In addition, CBF can be measured for the whole brain, not just in a few slices. Finally, coregistration with MR images allows measurement of CBF in specific anatomic locations.
Despite the advantages of PET, significant methodological problems needed to be overcome in this study. One major methodological issue is the definition of the regions of interest. One option is to spatially normalize (warp) the PET images to a template defined in a standard space, such as Taliarach space, and calculate mean CBF values using standard ROIs. However, it is our experience that spatial normalization programs, such as the one embedded in SPM99, are unable to successfully warp hydrocephalic brains, where the ventricles are enlarged by definition and other distortions such as sulcal dilation may be present, to a “normal” template brain. In addition, an attempt at such a warping ignores the underlying pathologic morphology of the hydrocephalic brain itself. Hence, ROIs were defined on the MR image of each subject or directly on PET if MR was unavailable, using techniques aimed at making the ROIs as consistent as possible for all the subjects.
The methods of global and regional analysis used in this study are therefore aimed at overcoming these problems. For the global analysis, the combination of seeding and threshold drawing functions on a slice-by-slice basis allowed reproducible ROIs to be drawn. Accuracy was checked and necessary corrections of the ROIs were then made to the ROIs of each slice to ensure anatomic integrity. Partial volume contamination, particularly bordering the ventricle is a potential source of error. However, the effects of such partial volume contamination of the CBF values is probably minimal because of the methods used, the relatively high resolution of the PET images, and the number of voxels involved compared with the total number in each slice. The regional analysis is less prone to such partial-volume effects as the ROIs were placed away from the tissue boundaries. The major disadvantage of these methods is that they are time consuming and to some degree operator dependent.
Significant reductions in mean CBF of both whole cerebrum and the cerebellum were found for NPH patients compared with controls. Furthermore, regional analysis revealed that the deep gray matter regions of the thalamus, putamen, and head of caudate had significantly lower mean CBF compared with controls. There was no significant difference in mean CBF of white matter ROIs. When the secondary NPH group was excluded from the comparison with controls, the difference in mean CBF for the cerebrum, cerebellum, thalamus, putamen, and caudate nucleus remained significant, whereas the mean CBF for the white matter regions remained similar to the controls.
The age of the control group was significantly younger compared with the patient groups; specific controls were not recruited for this project because controls from the acute head injury program (Coles et al., 2002) were used to minimize radiation exposure. The relationship between age and CBF is controversial, although Meltzer et al. (2000) using PET with MR coregistration and partial volume correction found that there was no decrease in CBF with healthy aging. In addition, the regional nature of our findings suggests that age is not the major factor influencing these results. The mean Pa
In a previously published review of CBF studies in NPH patients, we found little consistency between investigators except that overall CBF was reduced (Owler and Pickard, 2001). Significant differences between NPH patients and controls were found in all but one study (Waldemar et al., 1993), although a reduction in cerebellar CBF was not reported in any study. In fact, some investigators using SPECT utilized the cerebellum as a reference region because it was not thought to be involved in NPH. Our findings suggest that such an assumption should not be made and that the process affecting the parenchyma of the cerebrum may also involve the cerebellum. With regards to regional analysis, there was no consensus on which regions of the brain were affected. Some authors suggested that the reduction in CBF may predominately involve the frontal region (Graff-Radford et al., 1989, 1987; Granado et al., 1991; Kristensen et al., 1996; Maeder and de Tribolet, 1995; Mathew et al., 1977; Meyer et al., 1985; Moretti et al., 1988; Nakano et al., 1996). There was only one study in which CBF in the thalamus was found to be reduced (Meyer et al., 1985). The basal ganglia have not previously been examined as distinct structures.
NPH is primarily a CSF circulation disorder with demonstrable abnormalities during CSF pressure monitoring such as increased frequency of B waves and a raised resistance to CSF absorption on CSF infusion studies (Boon et al., 2000, 1998; Czosnyka et al., 1996; Pickard et al., 1980). However, it is likely that a disorder of CSF circulation per se is probably not the only pathologic process; rather, some process affecting the viscoelastic properties of the brain parenchyma itself may play a role (Owler et al., 2001; Pang and Altschuler, 1994). Such a process may be related to the cerebral vasculature (Bradley et al., 1991). Several authors have described an association between hypertension and idiopathic NPH (Casmiro et al., 1989; Haidri and Modi, 1977; Koto et al., 1977; Krauss et al., 1996; Shukla et al., 1980). Postmortem studies of NPH patients have demonstrated intimal thickening and hyalinization of arterial walls in the white matter, basal ganglia, and thalamus (Akai et al., 1987). The vessels most at risk of such changes are the lenticulostriate vessels because these are end arteries with a prolonged course through the brain parenchyma. As the lenticulostriate vessels and similar vessels are the main arterial supply to the regions of the thalamus, caudate, and putamen, the reduction of CBF seen in patients with idiopathic NPH compared with controls supports the role for cerebrovascular disease in the pathophysiology of idiopathic NPH. Although white matter hyperintensities were common in our patients, there was no significant correlation between the degree of white matter hyperintensities and mean CBF for any ROI. Of course, this does not exclude the possibility that such white matter changes are small infarcts but simply shows that the CBF of the remaining white matter is not reduced.
The most important clinical feature of NPH is that of gait disturbance (Boon et al., 2000; Casmiro et al., 1989; Fisher, 1982; Greenberg et al., 1977; Shenkin et al., 1973), although its mechanism is not fully understood. The characteristics of the abnormal gait are poor balance, hypokinesia, and freezing, which are consistent with a frontal gait apraxia (Fisher, 1982). Stolze et al. (Stolze et al., 2001) noted the lack of balance regulation and motor programming in the gait of patients with NPH. They suggest that the lack of response to external cues in patients with NPH indicates that the role of the basal ganglia and supplementary motor cortex is limited. However, some of the features of the gait disorder may also be related to pathology within the basal ganglia. The findings of this study suggest that mean CBF in the white matter, including that of the frontal region, of patients with idiopathic NPH is no different to controls. However, the mean CBF values for the thalamus, putamen, and head of caudate were all significantly reduced. We were able to demonstrate that a lower CBF in the thalamus of patients with purely idiopathic NPH correlated with an increased NPH score. In addition, CBF in the putamen of these patients was correlated with a poorer level of functioning as assessed using the modified Stein-Langfitt score. Thus it appears likely that the role of the basal ganglia in the gait disorder of NPH may be underestimated at the present time.
Whether the reduction in CBF in the basal ganglia and thalamus is a primary phenomenon or whether it occurs secondary to deafferentation secondary to processes in other areas remains to be elucidated. In Huntington's disease, CBF in the caudate nucleus, an area of primary pathology, is reduced. The reduction in CBF in the caudate nucleus correlates with disease progression. (Deckel et al., 2000; Hasselbalch et al., 1992; Reynolds et al., 2002). In Parkinson's disease, CBF is decreased throughout the basal ganglia (Wolfson et al., 1985) and changes in CBF, presumably secondarily to the primary pathology, are seen in distant regions such as the supplementary motor cortex (Kikuchi et al., 2001).
Moreover, the reduction in CBF in the basal ganglia and thalamus may also contribute to the cognitive deficits of NPH. The striatum receives widespread cortical input and, via other basal ganglia and the thalamus, projects to frontal cortex. Interruption of frontostriatal pathways is a possible explanation for the cognitive deficits of Parkinson's disease (Owen et al., 1998) and may explain the frontal lobe cognitive deficits seen in NPH.
CONCLUSION
Our study has documented several new findings regarding the pathophysiology of NPH. Using 15O-water PET combined with anatomic ROI definition on coregistered MR, we were able to demonstrate that mean CBF was decreased in the cerebrum and cerebellum of patients with idiopathic NPH compared with normal healthy controls. It also showed that the regions most likely to be related to this decrease in CBF were the deep gray regions of the thalamus, putamen, and caudate nucleus. In contrast, white matter (including periventricular) mean CBF was not reduced in NPH compared with normal controls. This study therefore supports the thesis that in addition to being a disorder of CSF circulation, cerebrovascular factors are involved in the pathophysiology of NPH and that these factors may also be related to the gait disorder of NPH.