
Abstract
The aim of this prospective study was to investigate whether decreased cerebrovascular reactivity to acetazolamide, as determined by single-photon emission computed tomography (SPECT), is an independent predictor of the 5-year risk of subsequent stroke in patients with symptomatic major cerebral artery occlusion. Cerebrovascular reactivity to acetazolamide in the middle cerebral artery (MCA) territory ipsilateral to the occluded artery was determined on the basis of two different methodologies: cerebral blood flow (CBF) percent change obtained quantitatively from xenon-133 (133Xe) SPECT, and asymmetry index (AI) percent change obtained qualitatively from N-isopropyl-p-[123I]-iodoamphetamine (IMP) SPECT. Seventy patients with unilateral internal carotid artery or MCA occlusion were divided into two groups within each SPECT methodology (normal or decreased CBF percent change and AI percent change) and followed up for 5 years. Cumulative recurrence-free survival rates for patients with decreased CBF percent change were significantly lower than for those with normal CBF percent change (P = 0.0205). There was no significant difference in cumulative recurrence-free survival rates between patients with decreased AI percent change and those with normal AI percent change. Only decreased CBF percent change was a significant independent predictor of stroke recurrence (P = 0.0051). The present study demonstrated that decreased cerebrovascular reactivity to acetazolamide determined quantitatively by Xe SPECT is an independent predictor of the 5-year risk of subsequent stroke in patients with symptomatic major cerebral artery occlusion, and that the qualitative method using I-IMP SPECT is a poor predictor of the risk of subsequent stroke in this type of patient.
Major cerebral arterial occlusion or stenosis due to atherosclerotic disease may lead to reduced perfusion pressure in the distal cerebral circulation (Powers et al., 1987). Although the presence of reduced perfusion pressure has been suggested to represent a risk factor for ischemic stroke, the importance of hemodynamic factors for prognostic considerations in major cerebral arterial occlusive disease remains controversial (Barnett, 1997; Klijn et al., 1997). Recent prospective studies using positron emission tomography (PET) or transcranial Doppler ultrasonography have demonstrated that cerebral hemodynamic status can predict the outcome of major cerebral arterial occlusive disease (Grubb et al., 1998; Gur et al., 1996; Markus and Cullinane., 2001; Vernieri et al., 1999, 2001; Yamauchi et al., 1996).
Single-photon emission computed tomography (SPECT) can quantify the three-dimensional distribution of CBF and detect hemodynamic compromise in terms of reduced cerebrovascular reactivity to acetazolamide (Kuroda et al., 1993; Schmiedek et al., 1994; Vorstrup et al., 1986). We have previously demonstrated that hemodynamic compromise, determined by acetazolamide challenge and quantitative CBF measurement using xenon-133 (133Xe) inhalation and SPECT, is associated with a high 2-year recurrence of ischemic stroke in patients with symptomatic occlusion of the middle cerebral artery (MCA) or internal carotid artery (ICA) (Ogasawara et al., 2002). Using a similar method, (Kuroda et al. (2001) also demonstrated that decreased regional cerebrovascular reactivity to acetazolamide is associated with a higher risk of subsequent ischemic stroke. Conversely, studies by (Yokota et al. (1998) that defined hemodynamic compromise based on qualitative (relative) CBF measured using N-isopropyl-p-[123I]-iodoamphetamine (123I-IMP) failed to demonstrate an association between hemodynamic failure and stroke risk. It is possible that the two SPECT methodologies, cerebrovascular reactivities to acetazolamide measured quantitatively and qualitatively, do not identify the same patients as having hemodynamic compromise and a high risk of recurrent stroke.
The purpose of this prospective study was to investigate whether decreased cerebrovascular reactivity to acetazolamide, as determined by SPECT, is an independent predictor of the 5-year risk of subsequent stroke in patients with symptomatic ICA or MCA occlusion. Further, we compared the utility of quantitative versus qualitative measurements of cerebrovascular reactivity. The risk of stroke was compared to a decrease in cerebrovascular reactivity (measured quantitatively using 133Xe SPECT or qualitatively using 123I-IMP SPECT) in 70 patients followed up for 5 years.
MATERIALS AND METHODS
This study was reviewed and approved by the institutional ethics committee. Seventy consecutive patients (53 men, 17 women) meeting the inclusion criteria and who were admitted to Tohoku University School of Medicine from January 1993 to March 1996 participated in the study. The mean age was 57 years (range, 38–69 years), and the population characteristics were described previously (Ogasawara et al., 2002). Inclusion criteria for the present study were as follows: (1) age younger than 70 years, (2) unilateral complete occlusion of the ICA or the horizontal portion of the MCA confirmed by angiography with arterial catheterization, (3) evidence of ischemic cerebrovascular events in the arterial distribution distal to the lesion within 3 months prior to study entry, (4) useful residual function (modified Rankin disability scale 0, 1, or 2) (UK-TIA Study Group, 1988), (5) minimal infarct specified by computed tomography (CT) or magnetic resonance imaging (MRI), and (6) informed consent obtained from the patient or relatives. Patients were excluded from the study if they had (1) cardio-embolic infarction, based on the onset pattern, angiographic findings, and results of electrocardiography and echocardiography (Cerebral Embolism Task Force, 1986); (2) vascular lesions caused by other systemic diseases, such as aortitis syndrome, moyamoya disease, or fibromuscular dysplasia; (3) an occlusion, or moderate to severe stenosis (>50%) of major cerebral arteries in the contralateral carotid or vertebrobasilar system; or (4) systemic conditions such as cardiac failure, renal failure, hepatic failure, respiratory failure, severe diabetes mellitus (fasting blood sugar ⩾300 mg/dL), and severe hypertension (diastolic blood pressure ⩾110 mm Hg).
All patients were treated with antiplatelet therapy (81 mg/d aspirin or 200 mg/d ticlopidine HCl), and treatment of other risk factors and medical therapy were based on the individual clinical picture. Although the attending physicians were unaware of the findings of the SPECT studies, treatment did not differ among the patients. No patients underwent bypass surgery. Patients were examined at 1-month intervals and followed up for 60 months after study entry. An interim history was obtained, and a neurologic examination was performed at each visit.
The study terminated on March 31, 2001. The primary end points were stroke recurrence or death, and observation terminated if stroke recurred or death occurred. Magnetic resonance imaging or CT was obtained and compared with initial studies to confirm recurrent stroke. Stroke in the previously symptomatic arterial territory without evidence of primary intracranial hemorrhage was classified as an ipsilateral ischemic stroke.
Single-photon emission computed tomography images were obtained using a multidetector ring-type scanner, consisting of 64 NaI crystals in a 38-cm diameter circle. After tomographic reconstruction, the spatial resolution and slice thickness in the center of the plane were 9 and 16 mm full width at half-maximum (FWHM) for static imaging and 20 and 25 mm FWHM for dynamic imaging, respectively. The device can obtain three tomographic slices for dynamic imaging or six tomographic slices for static imaging in a single scanning process. The energy window in this study was 140 KeV (± 15%). Projection data for static and dynamic imaging were processed with Ramachandran's filtered backprojection after introduction of a Butterworth prefilter. A 64 × 64 (123I-IMP) or 32 × 32 (133Xe) image matrix was used.
Each subject underwent four SPECT studies. The first (133Xe SPECT at rest) and second (133Xe SPECT with acetazolamide challenge test) studies were performed consecutively on the same day, while the third (123I-IMP SPECT at rest) and fourth (123I-IMP SPECT with acetazolamide challenge test) studies were performed 2 and 7 days later, respectively. Thus, all SPECT studies were performed within 8 days.
The tracer was administered in a quiet, dimly lit room while the patient was resting with his or her eyes open. The patient's head was immobilized with a ready-made plastic headholder to align the external ear canals with the positioning crossed-light beam. Three markers were affixed on the head under the guidance of a light beam to reproduce the same head position during the four SPECT studies. Two markers were placed on the anterior edge of the external ear canals, and one was placed on the midline of the nose ridge. The three markers lay along a plane perpendicular to the axis of camera rotation.
Patients first inhaled 1.48 GBq 133Xe gas for 1 minute, and sequence SPECT imaging was performed every 1 minute for 10 minutes using a high-sensitivity collimator. Quantitative CBF mapping was reconstructed with the Kanno-Lassen method (Kanno and Lassen, 1979). Thirty minutes after the resting 133Xe SPECT measurement, the 133Xe SPECT study with acetazolamide challenge was performed by administering intravenous acetazolamide (1,000 mg) 10 minutes before 1.48 GBq 133Xe gas inhalation. Next, SPECT imaging with a high-resolution collimator was performed 15 minutes after intravenous injection of 111 MBq 123I-IMP, and tomographic data were continuously obtained over a 30-minute period. Finally, 1,000 mg acetazolamide was given intravenously, and the 123I-IMP SPECT study was repeated 10 minutes later. Dosimetry of 133Xe and 123I-IMP was estimated using guidelines from the Task Group of Committee 2 of the International Commission on Radiological Protection (1987). Effective dose of 123I-IMP was 3.55 mSv/111 MBq, and effective dose of 133Xe rebreathing (10 minutes) was 1.18 mSv/1.48 GBq. Total effective dose of the four SPECT studies was estimated as 9.4 mSv.
Single-photon emission computed tomography studies were performed in all patients at least 1 month after a last ischemic event and within 2 weeks before study entry. One tomographic plane, located 50 to 75 mm (133Xe SPECT images) and 50 to 66 mm (123I-IMP SPECT images) above and parallel to the orbitomeatal line, respectively, was analyzed for each patient, and the region of interest (ROI) was placed directly on each selected SPECT image. Computed tomography- or MRI-SPECT imaging coregistration was not used. Following the atlas developed by Kretschmann and Weinrich (1986), one investigator, who was masked to patient data, manually drew an irregular ROI of 16 cm2 or more in the cerebral cortex perfused by the ipsilateral MCA. This ROI was placed in the regions where infarction was not present on CT or MRI. On each SPECT image, a mirror-image ROI was also placed in the corresponding region on the contralateral side. Identical ROIs were analyzed in each subject for four SPECT studies.
Regional cerebrovascular reactivity to acetazolamide in the MCA territory ipsilateral to symptomatic occluded artery was determined on the basis of two different methodologies. On 133Xe SPECT images, the mean CBF was determined in each ROI. As quantitative assessment, CBF percent change was calculated as follows: CBF percent change = [(acetazolamide challenge CBF – CBF at rest) / CBF at rest] x 100. Conversely, on 123I-IMP SPECT images, the mean count was determined in each ROI. The degree of right-left hemispheric asymmetry in the MCA territory was calculated as the following asymmetry index (AI): AI = (Coccl - Ccon) / ([Coccl + Ccon] / 2) x 100, where Coccl is the mean count on the occluded side and Cnon is the mean count on the corresponding region on the contralateral side. The AIs were calculated at rest and with acetazolamide challenge. For qualitative assessment, the difference between the AI with acetazolamide challenge and the AI at rest was calculated and defined as AI percent change. The value is positive when regional cerebrovascular reactivity to acetazolamide in the occluded side is higher than that in the contralateral side, and negative when regional cerebrovascular reactivity to acetazolamide in the occluded side is lower than that in the contralateral side.
Using 133Xe and 123I-IMP SPECT, we studied 10 normal subjects (8 men and 2 women) aged 35 to 65 years (mean, 52.3 years) to obtain control values prior to evaluation of CBF data. Informed consent was obtained for these 10 normal subjects. The control values of CBF percent change obtained by 133Xe SPECT in 20 ROIs ranged from 22.5 to 34.0 (28.1% ± 4.41%, mean ± SD). The normal values of AI percent change obtained by 123I-IMP SPECT in 10 sets of ROIs ranged from −5.99 to 6.01 (0.01 ± 3.64) when the left and right side were defined as the occluded and contralateral side, respectively. CBF or AI percent change in the control subjects was not age dependent.
On the basis of SPECT data, 70 patients were divided by two different methodologies into two hemodynamic categories at study entry. The first group included patients with normal or decreased CBF percent change ipsilateral to the symptomatic occluded artery. We considered values lower than the 95% confidence limit of the control population (<18.9%) to be decreased. The second group included patients with normal or decreased AI percent change. The lower 95% confidence limit of AI percent change defined in the control population was −8.22. In the present study, however, AI percent change was considered decreased when the value was less than −10; this threshold is commonly used in qualitative analysis with SPECT (Hirano et al., 1994; Monsein et al., 1991). One investigator who was unaware of the clinical status of the patients performed patient categorization.
Values were expressed as the mean ± SD for statistical analysis. Clinical backgrounds between the two groups were compared using the Student's t test or the χ2 test, as appropriate. Cumulative recurrence-free survival rate or the incidence of ipsilateral recurrent stroke was also compared between the two groups using the Kaplan-Meier method and log-rank statistics. Multivariate analysis with the Cox proportional hazards model was used to determine the joint effect of multiple variables on stroke recurrence over time. The risk factors, site of vascular lesion, CBF percent change ipsilateral to the symptomatic occluded artery, and AI percent change were considered covariates. Statistical significance was set at the P < 0.05 level.
RESULTS
Based on the CBF percent change ipsilateral to the symptomatic occluded artery, 23 patients had decreased CBF percent change, and 47 had normal CBF percent change (Table 1). There was no significant difference in population characteristics between the two groups. The CBF percent change contralateral to the symptomatic occluded artery was normal in all 47 patients with normal ipsilateral CBF percent change, whereas it was normal in 16 and decreased in 7 of 23 patients with decreased ipsilateral CBF percent change.
Patient characteristics at entry into study
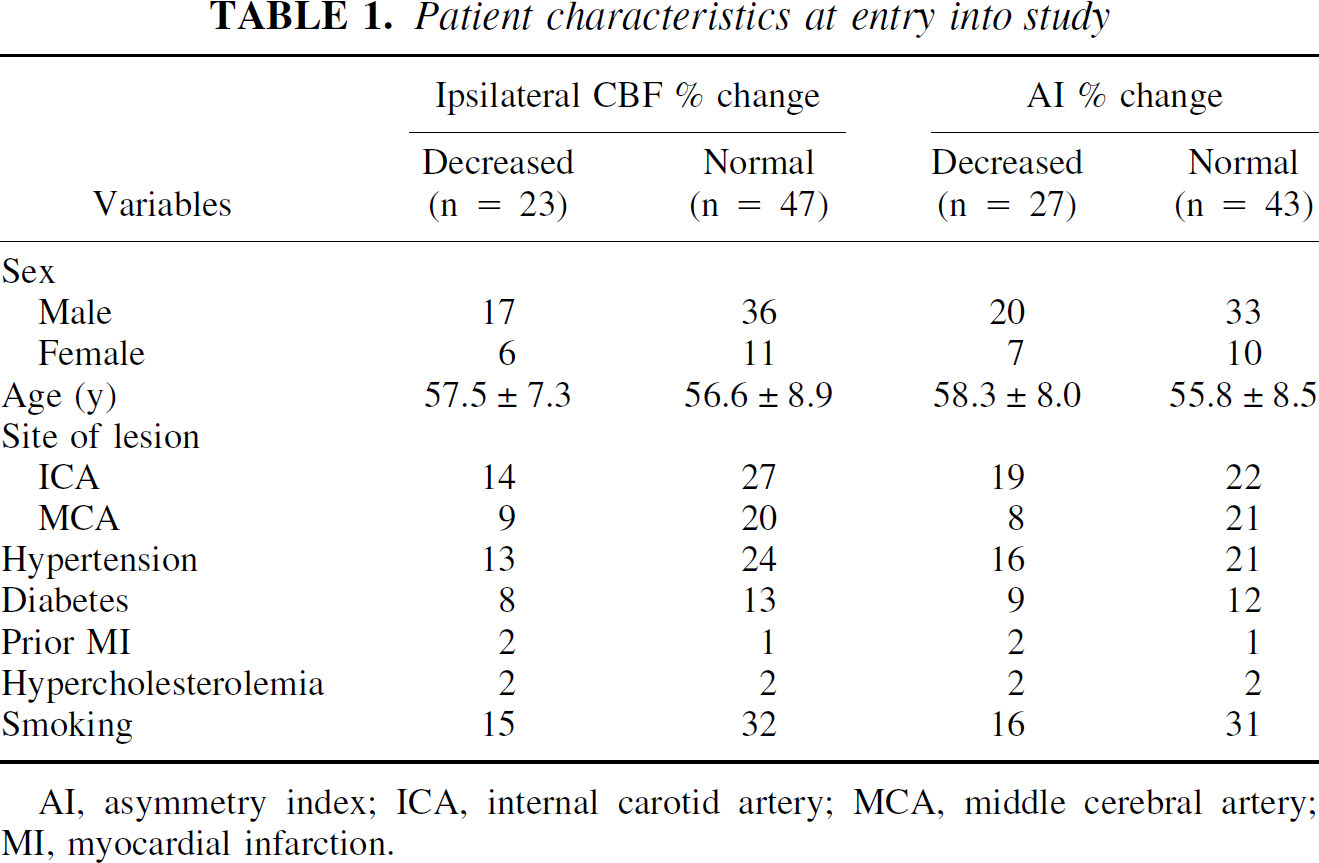
AI, asymmetry index; ICA, internal carotid artery; MCA, middle cerebral artery; MI, myocardial infarction.
Twenty-seven patients had decreased AI percent change, and 43 had normal AI percent change (Table 1). There was no significant difference in population characteristics between the two groups. In all 43 patients with normal AI percent change, the values were under the upper 95% confidence limit defined in the control population (<8.2).
Ipsilateral CBF percent change was significantly correlated with AI percent change in the 70 patients studied (r = 0.601, P < 0.0001). Of 27 patients with decreased AI percent change, 11 (41%) had normal ipsilateral CBF percent change. Seven of 43 (16%) patients with normal AI percent change had decreased ipsilateral CBF percent change with decreased contralateral CBF percent change. Five of these seven patients had ICA occlusion with collateral circulation through the anterior communicating artery. Decreased AI percent change was 70% sensitive and 77% specific for decreased ipsilateral CBF percent change (Table 2). Representative images in a patient with decreased AI percent change and normal ipsilateral CBF percent change are illustrated in Fig. 1.
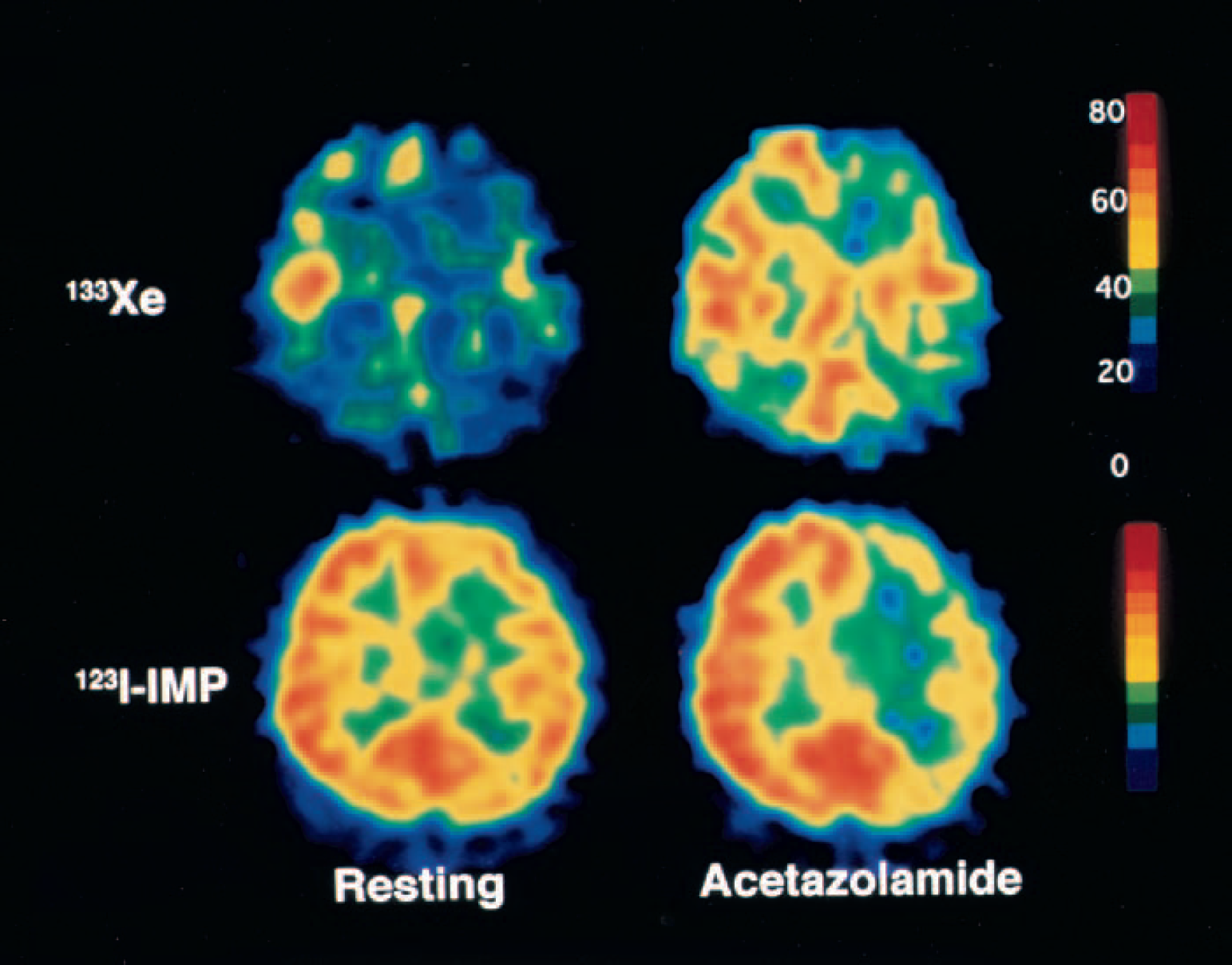
A 42-year-old woman with symptomatic left internal carotid artery occlusion exhibiting decreased asymmetry index (AI) percent change and normal ipsilateral cerebral blood flow (CBF) percent change. With acetazolamide challenge, CBF on 133Xe tomograms increased from 38 to 47 mL·100g−1·min−1 (CBF percent change = 24%) on the left side and from 45 to 61 mL·100g−1·min−1 (CBF percent change = 36%) contralaterally. This asymmetrical increasing rate of CBF was shown on 123I-IMP SPECT images as a decrease in AI percent change (−13.0), although ipsilateral CBF percent change determined on 133Xe tomograms was within normal limits (>18.9%). 133Xe, xenon-133; 123I-IMP, N-isopropyl-p-[123I]-iodoamphetamine.
Relation between ipsilateral cerebral blood flow % change and asymmetry index % change
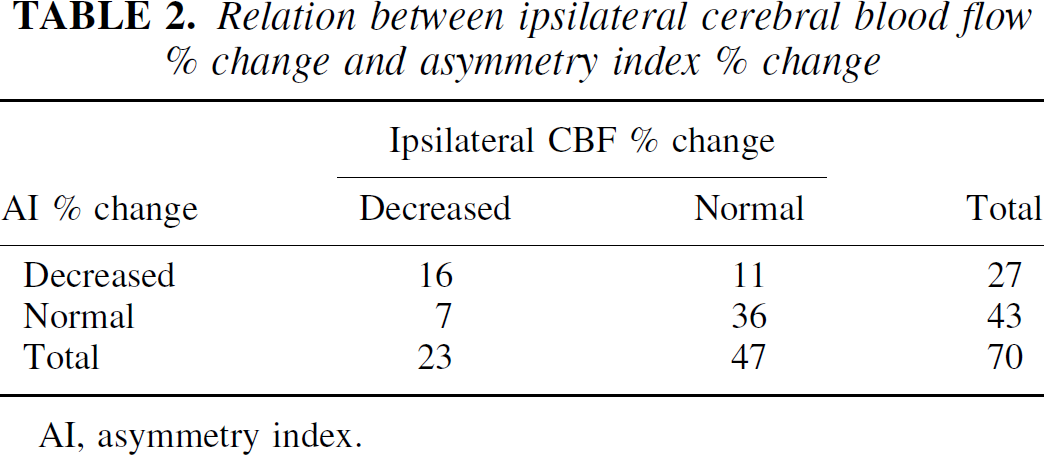
AI, asymmetry index; ICA, internal carotid artery; MCA, middle cerebral artery; MI, myocardial infarction.
All 70 patients were followed up for 5 years or until stroke recurrence or death. A total of 13 strokes were identified, 11 of which were ipsilateral to ICA or MCA occlusion. Four deaths were attributed to lung cancer, gastric cancer, myocardial infarction, and a motor vehicle accident.
Ischemic strokes occurred in 8 of 23 patients with decreased ipsilateral CBF percent change and 5 of 47 patients with normal ipsilateral CBF percent change. There were eight ipsilateral strokes in patients with decreased ipsilateral CBF percent change and three ipsilateral strokes in those with normal ipsilateral CBF percent change. Death occurred in one patient with decreased ipsilateral CBF percent change and in three patients with normal ipsilateral CBF percent change. The cumulative recurrence-free survival rate in patients with decreased ipsilateral CBF percent change was significantly lower than in those with normal ipsilateral CBF percent change (P = 0.0205, Fig. 2). The risk of ipsilateral stroke in patients with decreased ipsilateral CBF percent change was significantly higher than in those with normal ipsilateral CBF percent change (P = 0.0015, Fig. 3). All strokes in patients with decreased ipsilateral CBF percent change occurred within 8 months of the last ischemic event.
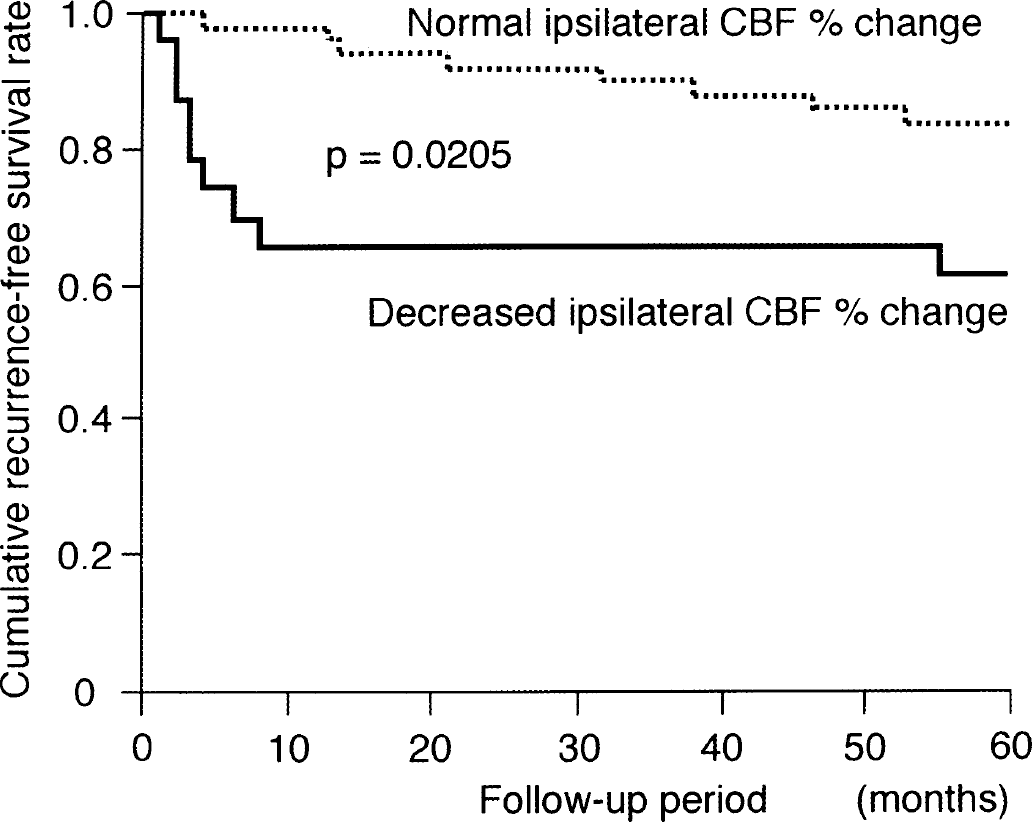
Kaplan-Meier cumulative recurrence-free survival curves in patients with normal and decreased ipsilateral cerebral blood flow (CBF) percent change.
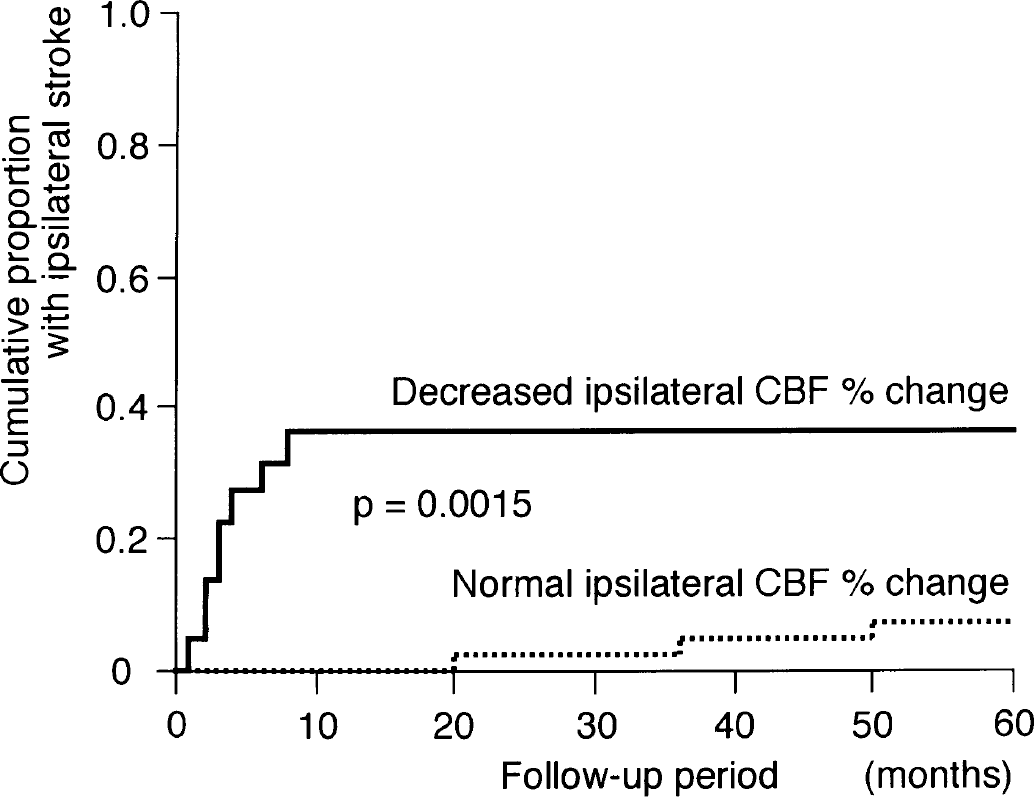
Kaplan-Meier cumulative failure curves for ipsilateral stroke in patients with decreased and normal ipsilateral cerebral blood flow (CBF) percent change.
Ischemic strokes occurred in 7 of 27 patients with decreased AI percent change and 6 of 43 patients with normal AI percent change. There were seven ipsilateral strokes in patients with decreased AI percent change, and four ipsilateral strokes in those with normal AI percent change. Death occurred in one patient with decreased AI percent change and in three patients with normal AI percent change. The cumulative recurrence-free survival rate was lower and the risk of ipsilateral stroke was higher compared to patients with decreased AI percent change and those with normal AI percent change, but the differences were not significant (P = 0.3186, Fig. 4; P = 0.0769, Fig. 5).
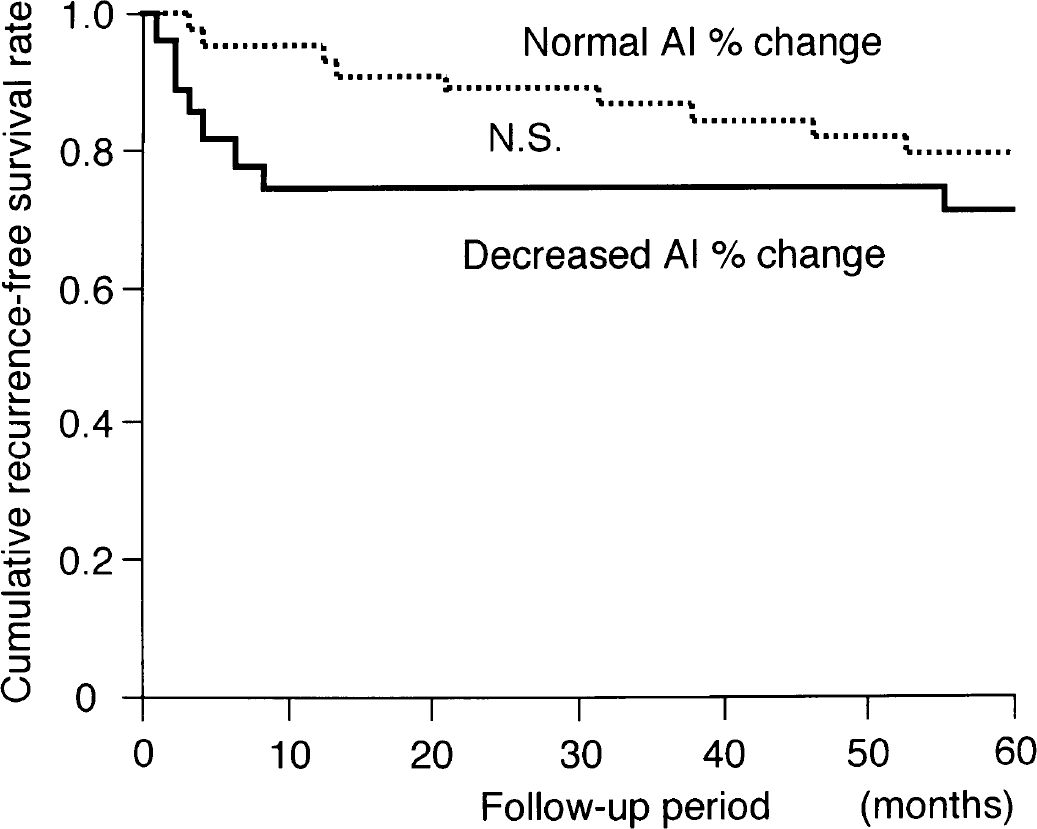
Kaplan-Meier cumulative recurrence-free survival curves in patients with normal and decreased asymmetry index (AI) percent change.
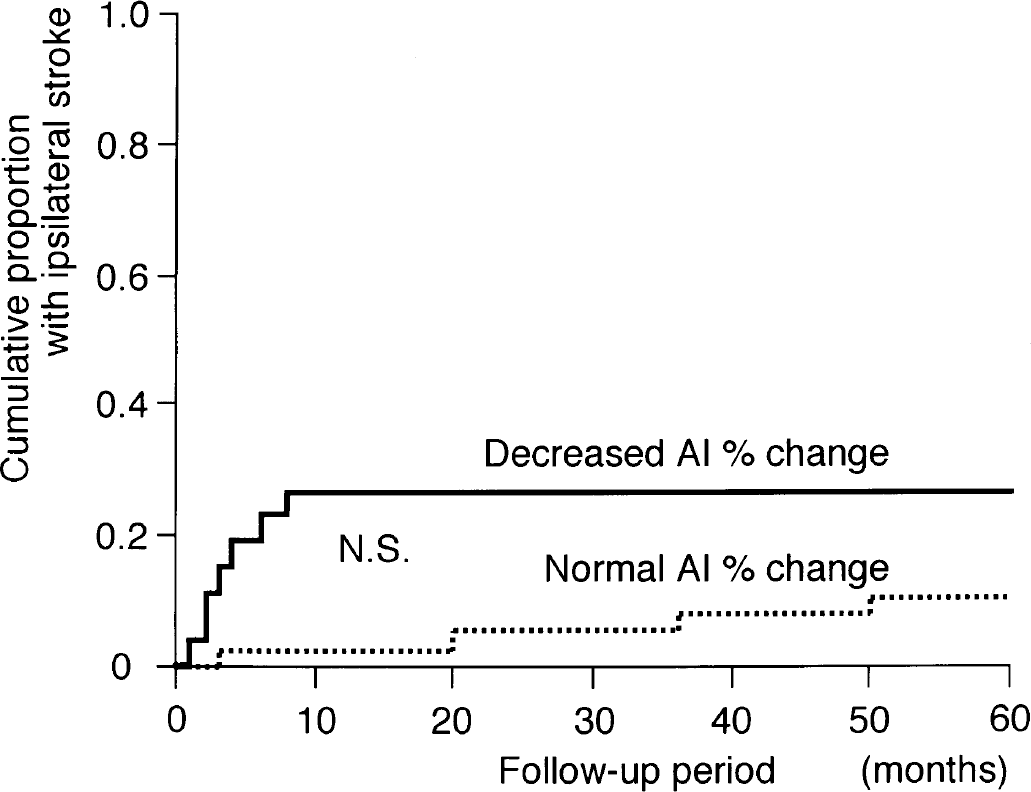
Kaplan-Meier cumulative failure curves for ipsilateral stroke in patients with decreased and normal asymmetry index (AI) percent change.
Multivariate analysis with the Cox proportional hazards model demonstrated that only decreased ipsilateral CBF percent change was a significant independent predictor of all strokes or ipsilateral strokes. Decreased AI percent change was not a significant independent predictor. The relative risk conferred by the decreased ipsilateral CBF percent change was 0.919 (95% CI, 0.865–0.972) for all strokes and 0.858 (95% CI, 0.775–0.949) for ipsilateral strokes (P = 0.0051 and P = 0.0030, respectively).
DISCUSSION
This study demonstrated that decreased regional cerebrovascular reactivity to acetazolamide, as determined by Xe SPECT, is an independent predictor of the 5-year risk of subsequent stroke in patients with symptomatic ICA or MCA occlusion. The high risk of ischemic stroke in patients with decreased ipsilateral CBF percent change, already described at 2-year follow-up, was confirmed at 5-year follow-up. The present study also demonstrated that a quantitative decrease in cerebrovascular reactivity to acetazolamide is a better predictor of recurrent stroke than a qualitative decrease. Qualitative change was not a significant independent predictor, which corroborates the findings of Yokota et al. (1998). Although AI percent change was significantly correlated with ipsilateral CBF percent change, 41% of patients with decreased AI percent change had normal ipsilateral CBF percent change, and 16% of patients with normal AI percent change had decreased ipsilateral CBF percent change. These findings indicate that the two SPECT methodologies (quantitative assessment using 133Xe SPECT and qualitative assessment using 123I-IMP SPECT) do not always identify the same patients as possessing hemodynamic compromise. Because relative 123I-IMP uptake normalized by contralateral uptake compared with relative CBF normalized by contralateral CBF shows a linear relationship (Nakano et al., 1989), the following factors, rather than difference in the tracer, may explain this disparity. First, normal ipsilateral CBF percent change with decreased AI percent change may occur when CBF increases asymmetrically after administration of acetazolamide (Yonas et al., 1998), and the qualitative assessment may incorrectly identify the ipsilateral cerebral hemodynamics as a “significant” compromise when CBF percent change is relatively higher in the contralateral side than in the ipsilateral side. Second, patients with unilateral ICA occlusion, especially with collateral circulation through the anterior communicating artery, may demonstrate hemodynamic disturbance in both hemispheres (Yamauchi et al., 1990, 1999). Further, mild and diffuse arteriosclerosis may impair cerebral hemodynamics on the contralateral side despite absence of lesion on angiography (Yamauchi et al., 1999; Yonas et al., 1998). Thus, the hemisphere ipsilateral to the occluded artery may be deemed normal when the value of the contralateral hemisphere is used as an internal control. In the present study, all seven patients with normal AI percent change and decreased ipsilateral CBF percent change had decreased contralateral CBF percent change, and five patients had ICA occlusion with collateral circulation through the anterior communicating artery.
The present study possesses several limitations regarding the SPECT methodologies. First, one tomographic plane, located above and parallel to the orbitomeatal line (50 to 75 mm for 133Xe SPECT images and 50 to 66 mm for 123I-IMP SPECT images) was analyzed for each patient. The difference in slice thickness between 133Xe and 123I-IMP SPECT may have influenced our results. In addition, an irregular ROI was manually drawn in the cerebral cortex perfused by the ipsilateral MCA using the atlas developed by Kretschmann and Weinrich (1986). Because of the age of the scanner, SPECT images could not be superimposed on CT and MRI images. A program for coregistration or anatomic standardization of SPECT data should be used to accurately compare 123I-IMP SPECT images with 133Xe SPECT images. Furthermore, whether only one selected tomographic plane reliably reflects the hemodynamic reserve on the entire territory perfused by the ICA or MCA is an important issue. However, the SPECT machine used in the present study can obtain only three tomographic slices for 133Xe SPECT imaging or six tomographic slices for 123I-IMP SPECT in a single scanning process. Further, the obtained SPECT tomographic slices are not sequential, and data are missing in every other slice. Therefore, we could not perform volumetric analysis of SPECT data in the present study. Second, each subject in the present study underwent four SPECT studies, which were performed over 8 days. The period between 133Xe and 123I-IMP SPECT studies is an important problem because baseline characteristics such as CO2 tension, O2 content of blood, blood pressure, and arousal level may have changed significantly between studies, and these variations may have affected regional CBF. Lastly, although we calculated cerebrovascular reactivity to acetazolamide in terms of CBF percent change, some investigators use absolute CBF change (Schmiedek et al., 1994). Because CBF percent change is defined as absolute CBF change (acetazolamide challenge CBF – CBF at rest) / CBF at rest, it is more difficult to detect reduction of cerebrovascular reactivity using CBF percent change than absolute CBF change when CBF at rest is lower and easier to detect if CBF at rest is higher.
Although SPECT can readily measure the three-dimensional distribution of CBF, qualitative methods using SPECT have been commonly used to detect hemodynamic compromise (Burt et al., 1992; Bushnell et al., 1991; Hoshi et al., 1994; Matsuda et al., 1991). Our results suggest that qualitative CBF measurement using SPECT may not be the optimum method for assessing cerebral hemodynamic compromise, and that quantitative CBF measurement using SPECT and acetazolamide challenge can identify patients at increased risk of subsequent stroke.