
Abstract
In some circumstances, cerebral blood volume (CBV) can be used as a measure for cerebral blood flow. A new near infrared spectroscope was used for determining the reproducibility of CBV measurements assessed by the O2-method. Twenty-seven healthy subjects were investigated. An intrasubject coefficient of variation (CV) was calculated, based on four identical episodes of desaturation–resaturation (O2-method) procedures for CBV measurements. Two trials were performed, with (trial 1) and without (trial 2) disconnecting the equipment. A mean CV of 12.6% and 10.0% was found in trial 1 and 2, respectively. Cerebral blood volume values yield 3.60 ± 0.82 mL 100 g−1. Cerebral blood volume could be measured reproducible in adults using near infrared spectroscopy, if the arterial desaturation is limited to approximately 5% from baseline level.
Near infrared spectroscopy (NIRS) is a noninvasive continuous method of monitoring brain oxygenation and hemodynamics. It has been used as a monitoring device during carotid, cerebrovascular, and cardiopulmonary bypass surgery, and on head-injured and other intensive care patients (Madsen and Secher, 1999). By using oxyhemoglobin (O2Hb) as an intravascular tracer, it is possible to calculate cerebral blood volume (CBV) using the desaturation–resaturation method, or “O2-method” (Wyatt et al., 1990). A gradual change of arterial oxygen saturation (SaO2) of approximately 10%, measured by pulse oximetry, induced by changing the inspired oxygen fraction (FiO2), is related to a small change of [O2Hb] and allows calculation of an absolute value of CBV (Wyatt et al., 1990; Elwell et al., 1994). However, the reproducibility of the measured values of CBV in adults is being questioned (Elwell et al., 1994). Faster sampling rates and a good signal-to-noise ratio has been suggested to improve reproducibility. Furthermore, a constant wide distance between emitter and detector (interoptode distance) is necessary to distinguish intracerebral from extracerebral tissue oxygenation (Harris et al., 1994; Germon et al., 1998). A new continuous wave (CW) NIRS instrument integrating these properties was used in this study (Van der Sluijs et al., 1997). The authors set out to test the reproducibility of CBV assessment using the O2-method using NIRS. Absolute CBV values were compared with those found in other studies using NIRS.
MATERIALS AND METHODS
After obtaining local research Ethics Committee approval and informed consent, the authors studied 27 healthy subjects (14 men, 13 women; mean age = 31 years, range 21 to 54 years).
The principles of CW NIRS and the O2-method are described in detail elsewhere (Wyatt et al., 1990; Elwell et al., 1994; Colier et al., 1997). The CW NIRS instrument (Oxymon, Physiology and Instrumentation Departments, University Medical Center Nijmegen, The Netherlands) measures changes in optical density (OD) in the near infrared region at three different wavelengths. The instrument has been compared with some others using a standardized phantom (Firbank and Delpy, 1993). It showed to be more sensitive (more than 9 OD). With this instrument it is, for example, possible to show the vascular response to a single finger opposition task in the motor cortex area without any averaging (Colier et al., 1999). Furthermore, it allows sampling average times down to 20 milliseconds without deteriorating the sensitivity (Van der Sluijs et al., 1997). Changes in OD are converted into concentration changes of O2Hb ([O2Hb]) and deoxyhemoglobin ([HHb]), using a modified Lambert–Beer law algorithm (Delpy et al., 1988). Total hemoglobin concentration ([tHb]), which is a measure for blood volume, is defined as the sum of [O2Hb] and [HHb]. The sensitivity of the NIRS data is improved by measuring the change in the difference between [O2Hb] and [HHb], defined as the oxygenation index (OI) and provided there is no change in [tHb] (Elwell et al., 1994). Sampling was performed at 10 Hz. Transmitting and receiving fibers were placed on the left side of the forehead with the receiving probe 2 cm from the midline. A constant interoptode distance of 5.5 cm was used. The optodes were held in position by an elastic band around the head. To correct for light scattering in the tissue, a fixed differential path length factor of 6.0 was used (Van der Zee et al., 1992).
The subjects were in a supine, comfortable position during the entire experiment. For each subject, a tryout desaturation–resaturation episode preceded the actual measurements. Cerebral blood volume measurements were repeated four times. Mean arterial blood pressure (MABP), end tidal CO2 (P
Reproducibility of CBV measurements might be worsened, due to optode displacement. To determine the effect of repositioning of the optodes on the reproducibility of the measurements, two different trials were performed. In the first trial, the optodes were disconnected after two episodes, to continue with the other two episodes after a short break. The second trial involved four consecutive episodes without disconnection of the equipment.
SaO2 and fH were monitored with a pulse oximeter (N200; Nellcor Puritan Bennett, St. Louis, MO, U.S.A.), with the sensor attached to the right frontal forehead. Mean arterial blood pressure was measured from the middle finger of the right hand noninvasively with a finger plethysmographic device (Finapres, Ohmeda, U.S.A.). Subjects breathed through a one-way facemask. Changes in inspiratory gas mixture were induced by means of a computer controlled mass flow system (Bronckhorst Hitec, Veenendaal, The Netherlands). FiO2 was monitored using an oxygen analyzer (OM −11; Beckmann, Fullerton, CA, U.S.A.). At the expiratory port of the system, P
RESULTS
The individual and mean (±SD) results of both trials are displayed in Table 1. The average decrease of SaO2 was 12% (range 10% to 15%). The mean intrasubject CV of both trials was 11.7%. The intersubject CV of CBV of both trials was 22% (20.2 to 24.4, 95% confidence interval). Mean values of CBV were significantly greater (P < 0.05) in females relative to males, 3.99 ± 0.91 and 3.34 ± 0.64 mL 100 g−1, respectively. Significant differences between sexes (P < 0.05) were seen in age and P

Reproducibility measurements of 27 subjects
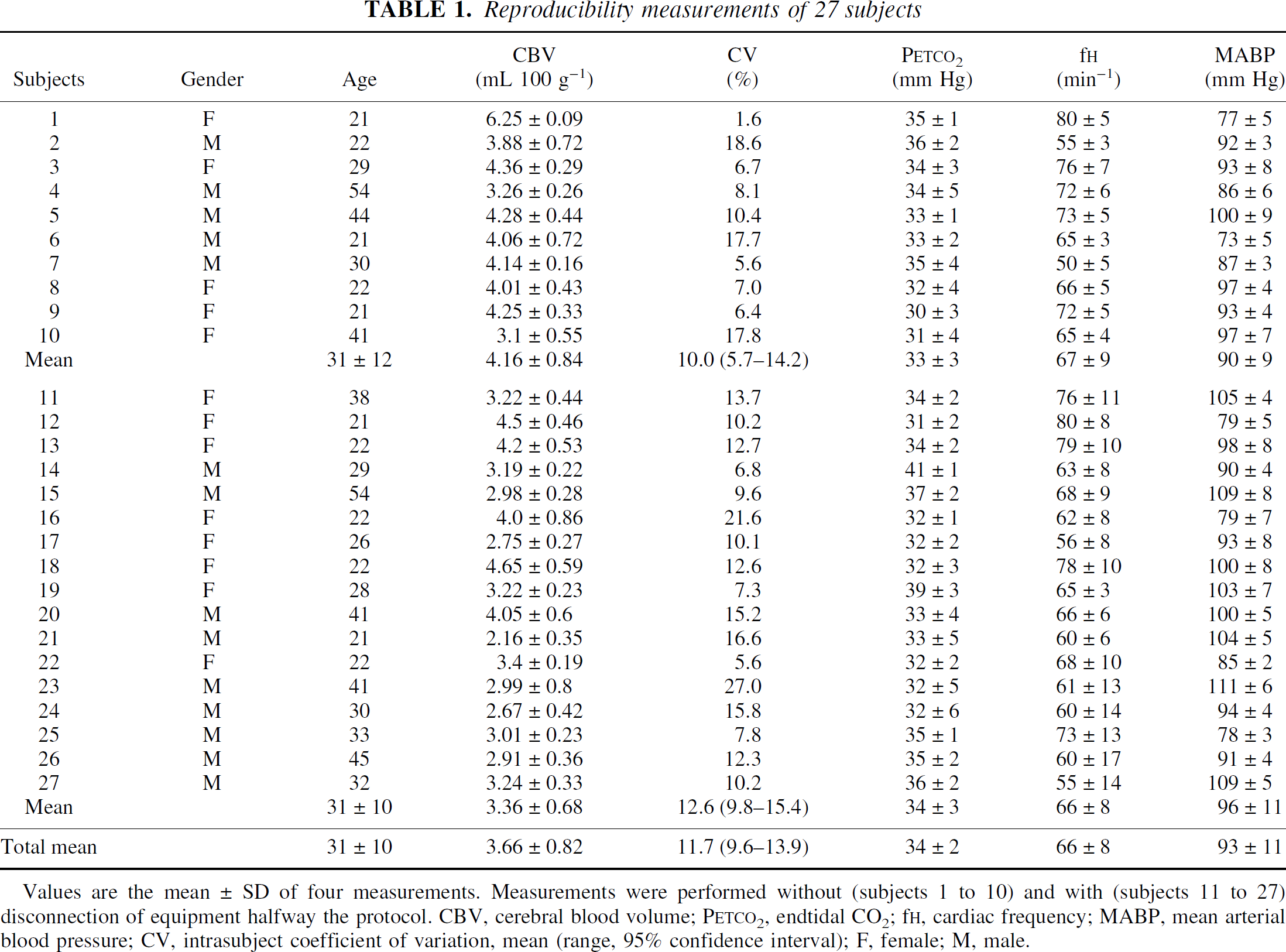
Values are the mean ± SD of four measurements. Measurements were performed without (subjects 1 to 10) and with (subjects 11 to 27) disconnection of equipment halfway the protocol. CBV, cerebral blood volume; P
DISCUSSION
In the current study, the reproducibility of CBV measurements in a large population of human adults was investigated with an improved CW NIRS instrument. The current study showed good reproducibility, even after reconnecting the equipment. Furthermore, this study showed sexual differences in CBV.
The experimental design to assess CBV followed Elwell's experimental setup (1994). An interoptode distance of 5 cm and a NIRO 500 (Hamamatsu Photonics KK, Japan) instrument with a sampling rate of 2 Hz was used. On each of the 10 subjects, 5 CBV measurements were performed using the O2-method. Only 22 measurements proved suitable for calculating CBV. A high intrasubject CV for the CBV measurements of 24% (range 6% to 38%) was found.
The current study also used the O2-method to calculate CBV. There is controversy whether the O2-method or the [tHb]-method is better for monitoring CBV. The latter method measures changes of [tHb] invoked by respiratory hypercapnia. Both methods can be used to measure cerebrovascular reactivity. However, baseline values during normocapnia can only be determined with the O2-method. Firbank et al. (1998) compared both methods, evaluating hypercapnic responsiveness. The O2-method was found to have a high CV (23%), whereas the other method had a low CV (3%). In contrast with the [tHb]-method to determine CBV, the O2-method was not able to distinguish CBV values on different levels of Paco2 in the analysis. The explanation of the high CV was mainly based on the accuracy of the pulse oximeter, which is 3% (Taylor and Whitwam, 1988). In contrast to Firbank, Totaro et al. (1998) found a good reproducibility for Δ[OI] and a bad reproducibility for Δ[tHb] while evaluating cerebrovascular reactivity. The authors favor the use of the O2-method to determine CBV at different Paco2 levels; moreover, significant (P < 0.001) changes of CBV were found during hyper- and hypocapnia, as compared with normocapnia (Van de Ven et al., 1999).
The absolute CBV values (3.66 ± 0.82 mL 100 g−1, n = 27) were comparable with values (3.51 ± 0.71 mL 100 g−1) found in earlier studies performed on 15 healthy subjects (5 men, 10 women; mean age 56 years) (Van de Ven et al., 1999). Values of CBV were slightly greater than CBV results of Elwell et al. (1994) (2.85 ± 0.97 mL 100 g−1, n = 10, mean age 27.5 years), but less than those found by Gupta et al. (1997) (5.38 mL 100 g−1, n = 13, mean age 35 years). As discussed by Gupta, an arterial desaturation of 10% to 15% may have crossed the threshold for hypoxic vasodilatation. In the current study, negligible values of Δ[tHb]/Δ[OI] were seen, suggesting a constant CBV during the applied hypoxia even during mild hypocapnia (mean P
The greater value of CBV in women in the current study is in line with the greater value of cerebral blood flow in other studies (Rodriguez et al., 1988). They suggest differences in functional organization of the cortex to be primarily responsible. Although the younger age of women could contribute to a higher CBV, this effect is counteracted by both a lower P
In conclusion, CBV assessed by the O2-method can be measured reproducibly in adults using near infrared spectroscopy. The required desaturation to calculate CBV preferably should be limited to 5% from baseline saturation level to avoid confounding hypoxic cerebral vasodilatation.