
Abstract
Task-induced changes in regional cerebral blood flow (rCBF) during verbal episodic memory activation were compared in 17 right-handed patients with dementia of the Alzheimer's type (DAT) and 20 healthy volunteers. Regional cerebral blood flow was assessed using single photon emission computed tomography (SPECT) and an injection of 133Xe (xenon, isotope of mass 133) in 21 regions of interest (ROI) during rest, passive listening to 36 words, and memorizing of a 12-word list repeated three times. In healthy subjects, memory—listening comparison showed activation of a distributed system involving several left-sided ROI, especially the posterior inferior frontal region. In patients with DAT, the same pattern of activation was found for listening—rest comparison, and no significant changes were found in memory—listening comparison. During listening compared with rest, significant activation was observed in left-sided hypoperfused regions. A significant correlation between memory performance and rCBF recorded in patients with DAT during the memory task was found only in the right lateral frontal region, a region that was not hypoperfused significantly in patients. The involvement of this region might relate to either retrieval effort or actual performance of patients with DAT on the memory task.
Keywords
Although there have been a variety of studies of resting regional cerebral blood flow (rCBF) and regional cerebral metabolic rate of glucose in patients with dementia of the Alzheimer's type (DAT), few imaging studies have been performed using activation paradigms. Most of these studies used verbal episodic memory tasks (Miller et al., 1987; Duara et al., 1992; Becker et al., 1996) because secondary memory is particularly affected in DAT whereas short-term memory can remain relatively preserved, as demonstrated by neuropsychological studies (Becker et al., 1988).
Two main questions have been addressed in such activation studies in DAT. The first one concerns the pattern of activation and, more particularly, the reactivity of hypometabolic regions in patients during a memory activation. Duara and colleagues (1992) have shown that regions in the DAT group that were classified individually as hypometabolic during rest exhibited metabolic activation during a reading memory task. The second question concerns the possible activation during memory tasks in patients with DAT of cortical areas that were not activated in healthy elderly subjects. A recent study from Becker et al. (1996) showed an activation in the right frontal cortex, a region that, for these authors, was not involved in the pattern of activation observed in healthy controls. The present study addressed these issues as well as how functional reactivity of cortical regions may reflect the range of memory performance in a group of patients with DAT.
This study is based on our previous works (Celsis et al., 1991; Démonet et al., 1994) using the same verbal memory activation task and single photon emission computed tomography (SPECT) that demonstrated in healthy subjects a specific activation pattern in the left hemisphere involving cortical and subcortical regions and functional reorganization of activation patterns in patients mildly impaired with parkinsonism. The present work focused on the following three points: 1) do patients with DAT exhibit significant changes in rCBF on memory task, 2) is this activation pattern different from that observed in healthy subjects who performed well on memory task, and 3) does the pattern of activation observed in patients with DAT depend on the level of performance?
SUBJECTS AND METHODS
Subjects
The patient group included 17 right-handed French-speaking subjects (8 women and 9 men), with a diagnosis of probable DAT based on the National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer's Disease and Related Disorders Association criteria (McKhann et al., 1984). Mean age (± standard deviation) was 65.6 ± 7.9 years, the mean score on the Mini-Mental State Examination was 18.9 ± 6, with a range of 6 to 26.
Controls were 20 right-handed French-speaking healthy volunteers (13 women and 7 men), aged from 54 to 74 years (mean age, 64.3 ± 5.4 years). The volunteers underwent clinical and neuropsychological evaluations to exclude any neurologic disorder or acquired cognitive impairment; all had normal computed tomography scans.
Activation paradigm
The paradigm activation consisted of three experimental conditions lasting 4 minutes—rest, passive binaural listening, and memorizing. These were presented in this order to all subjects, who underwent the three cerebral blood flow (CBF) measurements in the same day, with a 60-minute interval of between conditions.
Rest. Subjects were asked to lie quietly, with eyes closed but ears unplugged. Most of the background noises that they could hear came from the rotating part of the tomograph.
Passive listening. This condition consisted of listening to words via earphones. Thirty-six concrete, bisyllabic, frequent words were presented at a rate of 9 words/minute. The subjects were told just to listen to the words without processing them in any particular way.
Memorizing. A list of 12 concrete, bisyllabic, frequent words, all differing from the words used for the passive listening condition, was presented in a binaural manner three times in the same order. Subjects were asked to try to remember as many words as they could because they would be asked to recall the words at the end of the procedure (after CBF measurement). Memory performance was assessed first by free recall, with the subjects' responses being tape-recorded. All subjects, including patients with DAT, gave at least one correct response on free recall in this study. Further, recognition of the target words among 12 distractors was assessed. A memory score (maximum score 24) then was built up by applying the following formula: number of hits in free recall + (number of hits in recognition – number of false alarms).
Cerebral blood flow measurement
Regional cerebral blood flow was measured using a fast-rotating single photon emission computed tomograph (Tomomatic 64, Medimatic, Copenhagen, Denmark) and an intravenous injection of 133Xe (xenon, isotope of mass 133; 2200 MBeq). Data were collected from three transverse slices simultaneously, each 2 cm thick, parallel and centered 1, 5, and 9 cm above the orbitomeatal plane, respectively. The in-plane resolution was 1.7 cm.
The subject's head was positioned in the appropriate position according to an external grid. Marks also were drawn on the skin of the subject's face, and a photograph of the head and of these different marks was used to readjust the head's position from one scan to the other.
During the 4-minute data collection, arterial partial pressure of carbon dioxide (Pa
With respect to the spatial resolution of our tomography system, it was not possible to perform a group analysis on a pixel-by-pixel basis. For this reason, we chose to analyze the results using 21 regions of interest (ROI) (Fig. 1). The ROI were determined according to a visual analysis of the images and based on data from an anatomic atlas (Talairach and Tournoux, 1988). The main topographic features used were based on two horizontal lines easily visible on the rCBF image of the mid slice. An anterior line corresponded to the posterior edge of the mesial frontal cortex, and a posterior line corresponded to the posterior pole of the thalamus. Once the shape and topography of the ROI were determined, the different ROI were superimposed on each of the corresponding rCBF slices using an interactive software. Because of the spatial resolution of the tomograph, the values in such ROI may represent only a partial value of the specified anatomic regions.
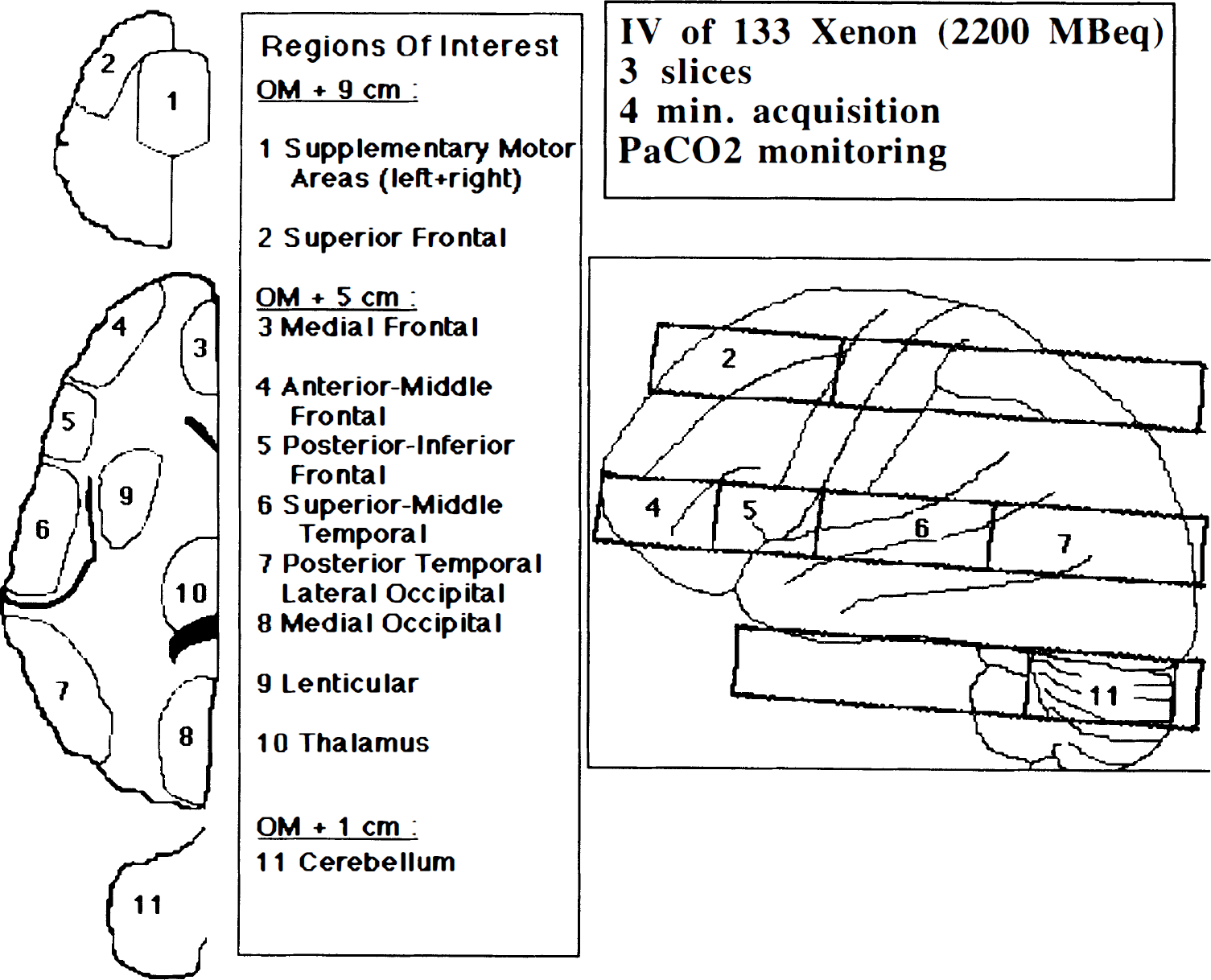
Regions of interest in the three axial slices.
Statistical analysis
To study functional activity changes, a three-factor (condition × ROI × group) analysis of variance (ANOVA) for absolute rCBF was performed. Then, for each ROI, across-condition comparisons were designed in each group of subjects using a one-factor ANOVA. Pair-wise comparisons between conditions were performed using post hoc Scheffé test.
To overcome the problems posed by the well-known heterogeneity of hemodynamic patterns in DAT, and according to a method described by Duara et al. (1992), resting state z scores for the normalized rCBF (ratio of the regional CBF over the grand mean CBF in the three slices for each subject) in the DAT group were computed by using the means and standard deviations obtained for the control group during the resting state. Then, on a subject-by-subject basis in the DAT group, any region with a z score less than −1.65 (P ≤ 0.05) in the resting state was classified as hypoperfused. Subsequently, the absolute rCBF at rest in the hypoperfused regions in these subsets of patients was compared with rCBF recorded in activation conditions. Finally, the relationship of performance to rCBF distribution during the memory task in the DAT group was assessed by Spearman rank order correlations.
RESULTS
Subjects' performance on memory task
Healthy subjects accurately performed the memory task, with a mean memory score of 22 ± 2.8 of 24, whereas mean score in the demented patients was only 8.7 ± 6.4 of 24. The observed range in patients with DAT was 0 to 19, with two patients scoring 0. Although all patients gave at least one correct response on free recall, the corresponding memory score could have been lower because of negative values attributed to false alarms. The difference between controls and patients with DAT was highly significant (Student's t test, P < 0.0001). No correlation was found between Mini-Mental State Examination score and memory score in the DAT group (P < 0.29, r2 = 0.075).
Across-task regional cerebral blood flow changes
No significant change in PaCO2 was observed among the conditions. Using absolute flow values (Table 1), a three-factor (condition × ROI × group) ANOVA for absolute rCBF revealed significant differences according to condition (P < 0.0001), ROI (P < 0.0001), and group (P < 0.0001). Significant interactions were as follows: group × condition (P < 0.0009) and group × ROI (P < 0.0005). No interactions were found between condition × ROI and between condition × ROI × group.
Mean and SD of cerebral blood flow (mL/100g/min) in the 21 regions of interest, according to experimental conditions in each group of subjects.
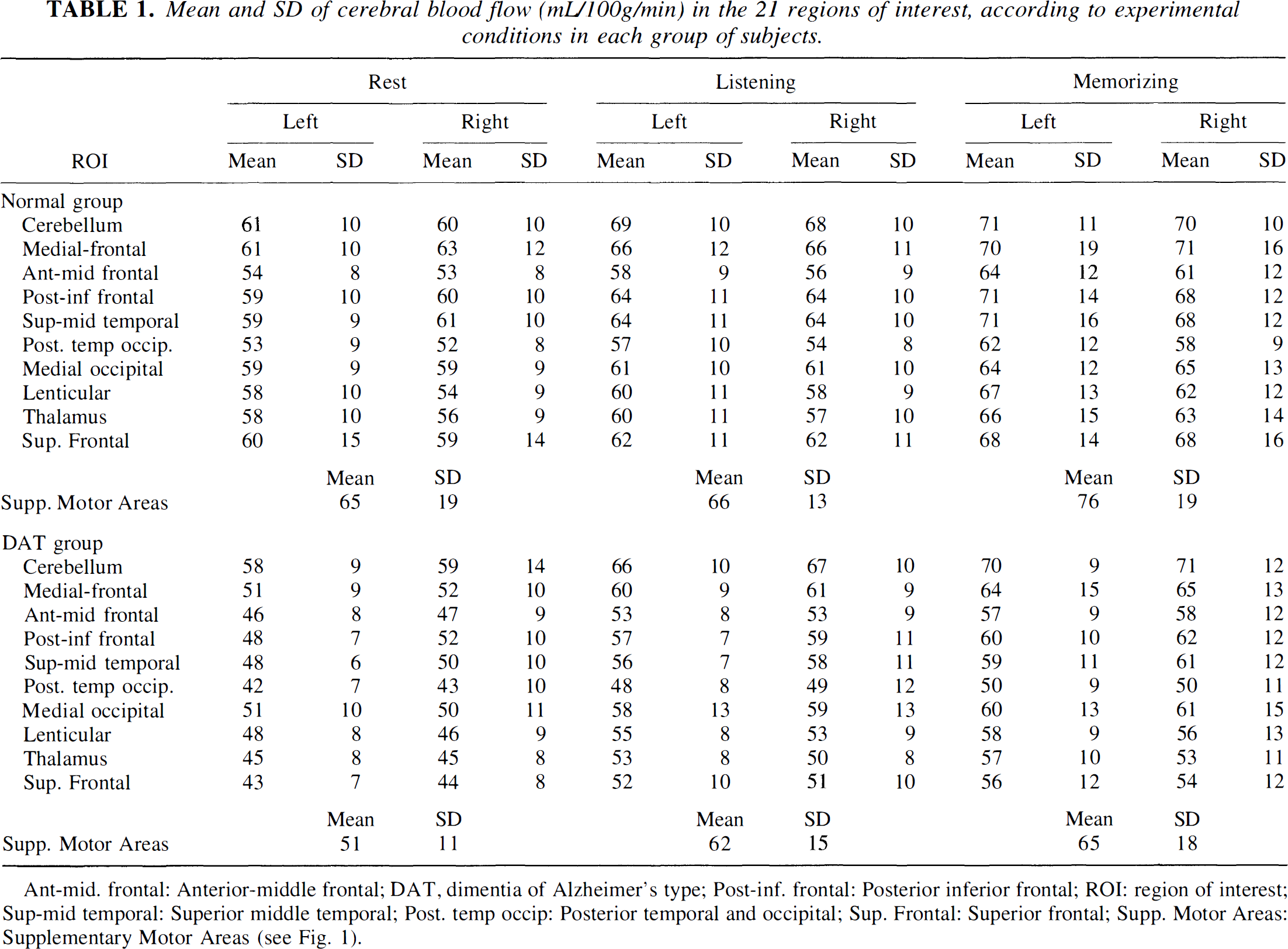
Ant-mid. frontal: Anterior-middle frontal; DAT, dimentia of Alzheimer's type; Post-inf. frontal: Posterior inferior frontal; ROI: region of interest; Sup-mid temporal: Superior middle temporal; Post, temp occip: Posterior temporal and occipital; Sup. Frontal: Superior frontal; Supp. Motor Areas: Supplementary Motor Areas (see Fig. 1).
In each group of subjects and in each ROI, a one-factor ANOVA showed significant across-condition differences in absolute rCBF in most of the ROI. In the control group, differences were not significant in only four ROI: the superior frontal regions, the supplementary motor area, and left medial occipital region. In the DAT group, differences were not significant in the following four regions: right posterior temporo-occipital region, the left and right medial occipital regions, and right thalamus. Post hoc pair-wise comparisons (Scheffé tests) between conditions revealed differences between the two groups of subjects.
In healthy subjects (Fig. 2), comparisons between the rest and listening conditions revealed significant rCBF increases for listening only in the cerebellar hemispheres, whereas comparisons between the memorization and listening conditions revealed massive activation in several left-sided regions, notably the left posterior inferior frontal region (P < 0.002).
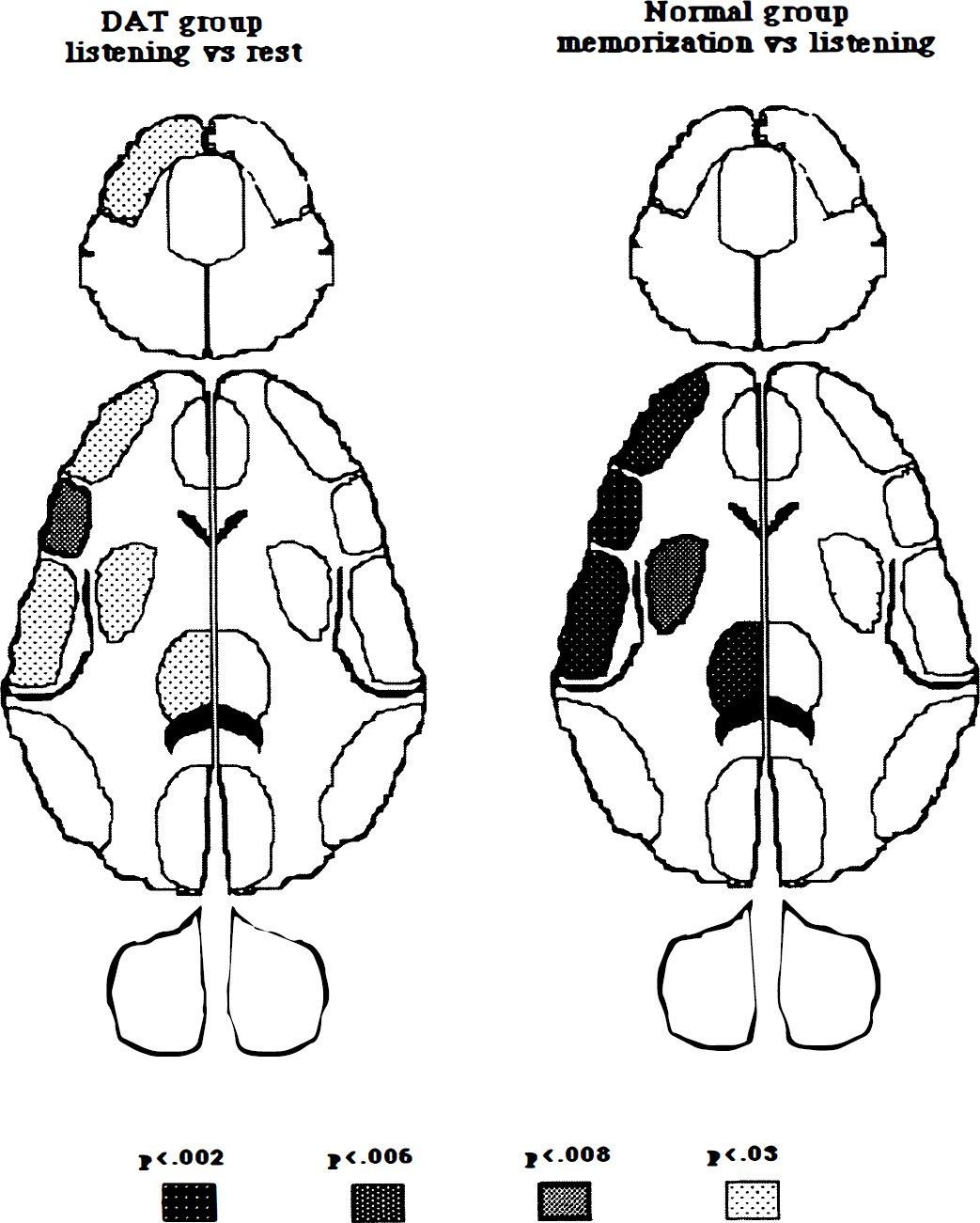
Increases in regional cerebral blood flow in the listening versus rest comparison in the dementia of Alzheimer's type group (left) and in the memorization listening comparison in the control group (right) demonstrated by Scheffé tests in each region of interest; maps of P values of each group are shown.
In patients with DAT (Fig. 2), significant rCBF increases for listening versus rest were found in the left posterior inferior frontal region (P < 0.008) and, to a lesser extent, in several left-sided regions (i.e. cerebellar hemisphere, thalamus, lenticular, anterior middle frontal, superior middle temporal, superior frontal); no significant change was found for comparison between memorization and listening.
These results indicate similar patterns of activation in both groups, but for different comparisons, that is, memorization versus listening in healthy subjects and listening versus rest in patients with DAT. This pattern was noted in patients with DAT no matter what the hemodynamic status observed at rest in a given region by comparison to normal values, as shown in the following section.
Table 2 shows the three ROI that were affected predominantly by the pathology (z scores for resting state in patients by reference to healthy subjects—i.e., left posterior temporal occipital [9/17 patients], left superior middle temporal [7/17 patients], and right posterior temporal occipital [5/17 patients]). Moreover, no patient presented significant hypoperfusion in the following ROI: right frontal regions (medial frontal and lateral frontal) and the left medial occipital region. Table 2 shows the amount of hemodynamic activation during experimental conditions in the regions frequently affected in patients with DAT. There was a significant activation in the left posterior temporal occipital region when listening was compared with rest (5.11 ± 2.89, P < 0.0007) in the nine subjects in whom this ROI was hypoperfused and in the left superior middle temporal region in the seven subjects demonstrating hypoperfusion for the same comparison (9 ± 4.2, P < 0.0012). No significant activation however was found for the right posterior temporal occipital region (5.8 ± 6.3, P < 0.11).
Hemodynamic activation in abnormally hypoperfused regions in DAT patients
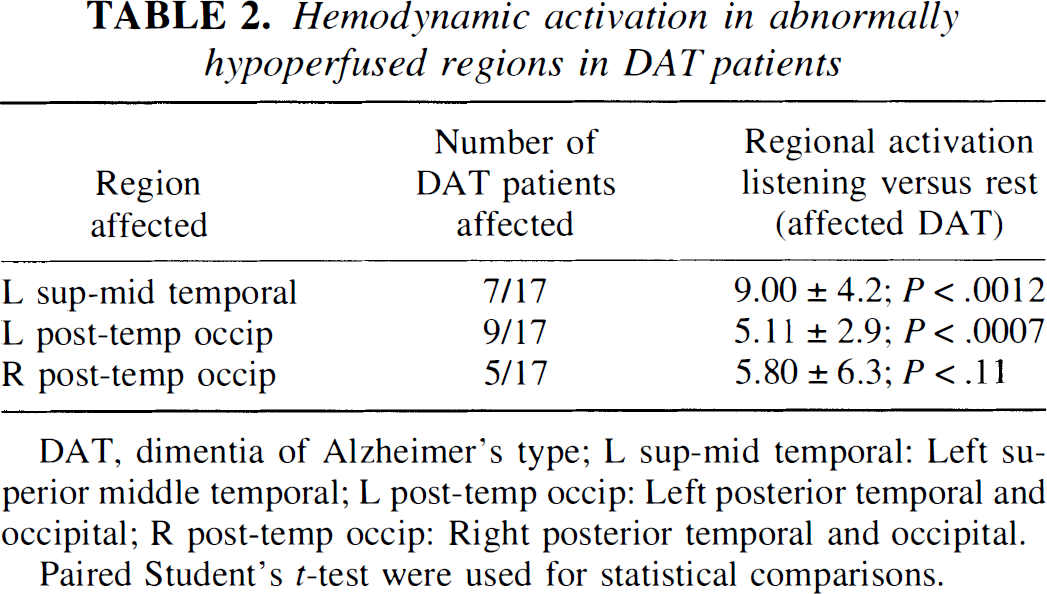
DAT, dimentia of Alzheimer's type; L sup-mid temporal: Left superior middle temporal; L post-temp occip: Left posterior temporal and occipital; R post-temp occip: Right posterior temporal and occipital.
Paired Student's t-test were used for statistical comparisons.
By contrast to findings in healthy subjects, no significant activation was noted in patients with DAT in these regions for the memorization versus listening comparison.
Correlations between memory performance and regional cerebral blood flow recorded in the dementia of Alzheimer's type group during the memorization task
No correlation could be studied in the control group between performance and rCBF distribution during the memorization task because of ceiling effect in the memory performance. Therefore, such correlations were sought in the DAT group only. Massive across-subject variability of absolute CBF values was controlled for by studying normalized values on memorizing and their correlations with memory performance.
Nonparametric Spearman rank order analysis performed on each ROI revealed only one significant correlation that concerned the right lateral frontal region (r = 0.675, P < 0.007) so that high performance corresponded to high normalized CBF values.
No significant correlation was found for either the rest or the listening conditions.
DISCUSSION
In the present study, activation tasks elicited significant hemodynamic effects in both groups of subjects. However, the main activation effect was observed between rest and listening in demented patients, whereas this effect was found between listening and memorizing in healthy subjects. Further, the activation pattern dedicated to the memory task in controls was identical to that observed in demented patients for both listening and memory tasks. This pattern involved left-hemispheric cortical and subcortical ROI likely to represent regions subserving language and verbal memory functions (Grasby et al., 1993; Fletcher et al., 1995). Such an unexpected activation during listening might be caused by the patients' impairment to understand, memorize, and follow the instructions given for the test. Consequently, it might be that the subjects tended to process the stimuli the same way during listening and memorizing tasks. As in controls, during efficient memorization of heard words, the most activated region in demented patients during listening was the left posterior inferior frontal region, roughly corresponding to Broca's area. This region has been associated repeatedly with rehearsal of auditorily presented words (e.g., Démonet et al., 1996; Fiez et al., 1996). Therefore, it may be suggested that demented patients rehearsed heard words during both listening and memorizing tasks. Such an automatic process, known to be preserved even in severely demented patients (Cummings et al., 1985), did not result in efficient memorization because of a massive damage to information encoding in long-term memory.
Cognition-related activation was observed even in significantly hypoperfused ROI in demented patients. This finding was reported previously in the literature (e.g. Duara et al., 1992). It implies that cortical areas affected by degenerative changes still may have functional reactivity. Furthermore, the reactivity observed in our study appears to be specific for cognitive processes involved by activation tasks. This activation in hypoperfused regions was observed in the left posterior temporal-occipital and superior middle temporal regions that were likely to participate in neural networks subserving verbal processes but not in the right posterior temporal occipital region, a region that is not likely to be involved in these networks. Thus, addressing the first two questions proposed in introduction, 1) demented patients did exhibit significant changes on memory task, but the same pattern also was observed on a passive listening task, and 2) this pattern is identical to that found in healthy subjects. However, such a preserved and specific activation pattern was not related to satisfactory memory performance in demented patients, just as if the functioning of left-sided neural networks (or their remaining parts) was inefficient and no more associated with memory processes.
When addressing our third question concerning the relationships between cognitive activation in demented patients and their memory performance, only one region, the right lateral frontal region, was identified in which the higher the rCBF, the better the performance. This correlation was found only in memorizing and not in listening or resting conditions; therefore, this correlation results from a task-dependent specific effect. Because of the obvious technical limitations of our study and the poor spatial resolution of the SPECT camera used, this result should be interpreted cautiously. However, the reliability of this finding is reinforced by three sources of evidence. First, no such correlation was found in neighboring regions, namely the right posterior inferior frontal region and right medial frontal regions, despite preserved rCBF in the latter. Second, in our previous SPECT studies (Celsis et al., 1991; Démonet et al., 1994), the right lateral frontal region was just below significance threshold in healthy subjects and in parkinsonian patients during the memory task that was near-ceiling performed. Third, this region has been identified repeatedly as the outcome of a variety of activation studies devoted to episodic memory (Buckner and Tulving, 1995, for review) using positron-emission tomography. However, its functional significance still is a matter of controversy because it has been related to either retrieval effort (Shacter, 1996) or retrieval success (Rugg et al., 1996) in healthy subjects. In the present study of demented patients, although mental effort obviously had to be a source of the observed right frontal involvement, our results showed that the reactivity of this region is due merely to the actual performance. A compensatory role for this region that was interpreted as the outcome of functional neuroplasticity recently was evoked by Becker et al. (1996), in an activation positron-emission tomography study of patients with DAT. Alternatively, these findings might correspond to remaining activities in the right lateral frontal cortex, a long-lasting preserved part of memory-linked neural networks whose other components undergo earlier damage. Follow-up activation studies using refined imaging methods in very early cases of DAT might help clarify the point.
Footnotes
Abbreviations used
Acknowledgments
The authors thank Thérèse Pujol and Chantal Blanchard for their technical assistance.