
Abstract
A method is described for the reliable production of controlled hypotension in experimental animals. Reduction in arterial blood pressure was obtained in rabbits by withdrawing arterial blood using a computer-driven pump operating within a feedback control system. Arterial blood pressure, blood flow velocity in the basilar artery (measured using transcranial Doppler), and anterior cortical microcirculation (measured using laser Doppler) were monitored. The aim of the experiments was to compare stability of hypotension produced using arterial blood pressure or basilar flow velocity as feedback control variables. Basilar artery flow velocity provided the most stable profound hypotension and during reinfusion when animals were not autoregulating. However, arterial blood pressure provided the most accurate stepwise control in autoregulating animals.
Keywords
Low arterial blood pressure is a common cause of reduced cerebral perfusion and hence of brain ischaemia. Experimental models have been developed to study the cerebrovascular changes that accompany profound arterial hypotension induced using hypotensive drugs (Pickard et al., 1979; Tyson et al., 1982; Nelson et al., 1992), haemorrhage (Mendelow et al., 1984), or both (Pickard et al., 1979; Grøgaard et al., 1989). Hypotensive agents may have additional effects on cerebral haemodynamics and, in addition, may influence the integrity of the blood–brain barrier (Smith et al., 1973; Anderson et al., 1980; Fitch et al., 1988). Manual withdrawal of arterial blood can avoid these effects, but maintenance of stable conditions over a longer period is difficult. Automatic control of arterial blood pressure using a computer-driven pump has been achieved by the infusion or withdrawal of blood at variable rates (Chambers et al., 1991; Nafz et al., 1992). However, difficulties with maintaining the arterial line are frequently encountered at low blood pressures, which provoke instability within the system.
We have employed a mechanical pump in experimental animals that induces and maintains graded hypotension for sufficient time to study cerebral ischaemia in a controlled and reproducible manner. We have investigated the optimal way of controlling the pump so that the influence of such effects as arterial line failure could be overcome.
MATERIALS AND METHODS
Experiments were performed on 16 ventilated, anaesthetised New Zealand rabbits of both sexes (weight 2.8–4.3 kg) under the UK Animals Act (Scientific Procedures, 1986). Details of the experimental setup has been described elsewhere (Richards et al., 1995). Arterial blood pressure (ABP) was measured using a femoral catheter advanced into the dorsal aorta. A second catheter was also inserted into the dorsal aorta via the remaining femoral artery to allow blood withdrawal. Blood flow velocity in the basilar artery was measured using an 8-MHz transcranial Doppler (TCD) probe (PC DOP 842, Scimed), and the cortical microcirculation was assessed using laser Doppler flowmetry (LDF-MBF3D, Moor Instruments, England). All signals were digitalised and recorded on an IBM PC (Zabolotny et al., 1995).
The mechanical pump system consisted of an infusion pump (Pump 22, Harvard Instruments) driven by specific software on a PC computer. The controlling feedback signal was derived from either (a) the arterial blood pressure monitor or (b) the TCD basilar artery flow velocity (FV). The pump was instructed to infuse or withdraw at a specific rate by the computer programme, which monitored status reports from the pump and the measured control signal. The programme algorithm (to be published elsewhere) seeks to reach the target value of the control variable in minimal time and to keep this value stable over a specified time. To achieve this, the controlling algorithm has been written to the following specifications:
When the difference between the measured and target variable is large, the pump rate is set to extract or infuse blood at a maximum rate (10 ml/min).
When approaching the target, the pump rate is gradually decreased.
When the current value of the controlled variable is within a certain acceptable “hold” range around the target, the rate is set to 0.
To avoid instability triggered by spontaneous fluctuation of the controlled variable or superimposed noise, the variable is filtered by a lowpass filter (moving average filter with window length initially set to 2 s and subsequently readjusted to 8 s).
The program is easy to handle and gives the user total control of the pump and the control algorithm. It detects when the pump has stalled and is able to suspend the operation when the communication link is accidentally broken. The programme is constructed so that either the ABP or FV signal can be used as the controlling variable. All the parameters that determine the algorithm can be set and changed by the user during the experiment.
The aim of the experiments was to adjust the controlled parameters provided by the computer programme and to assess the stability of blood pressure for different feedback controlling signals at different levels of hypotension. Two series of experiments were performed:
Validation of the system in providing stable and profound hypotension (10 experiments); in each animal a 30-min period of deep hypotension was induced after 20 min recording under baseline normotensive conditions.
Investigation of the ability of the system to control FV or ABP at changing hypotensive levels in the same experimental animal (six experiments). The purpose of this group of experiments was to assess the stability of the system when operating against potentially intact autoregulatory mechanisms. In three animals ABP was gradually decreased and stabilised for 20-min periods at different levels of hypotension using the ABP signal as the control variable. During reinfusion, the FV signal was used as a control variable and stabilised for 20-min epochs at different levels. In the remaining three experiments the FV signal was the controlling variable during blood withdrawal, and the ABP the controlling variable during rein-fusion.
As a measure of stability of the system, the standard deviations of the ABP, FV, and LDF divided by their mean values were calculated for each period of controlled hypotension. The comparisons of stability between different types of control (ABP or FV) were performed using the t test.
RESULTS
Group A experiments
Using ABP as the controlling feedback variable. An example of time trends of the infusion rate and of ABP from this series of experiments is given in Fig. 1A. The target pressure was set to 30 mm Hg in three cases and to 25 mm Hg in two (below the limit of autoregulation in all cases). In these experiments, clotting of blood within the arterial catheter was frequently encountered despite flushing with heparinised saline. This resulted in instability during the planned hypotension in three of the five experiments (Fig. 1B).
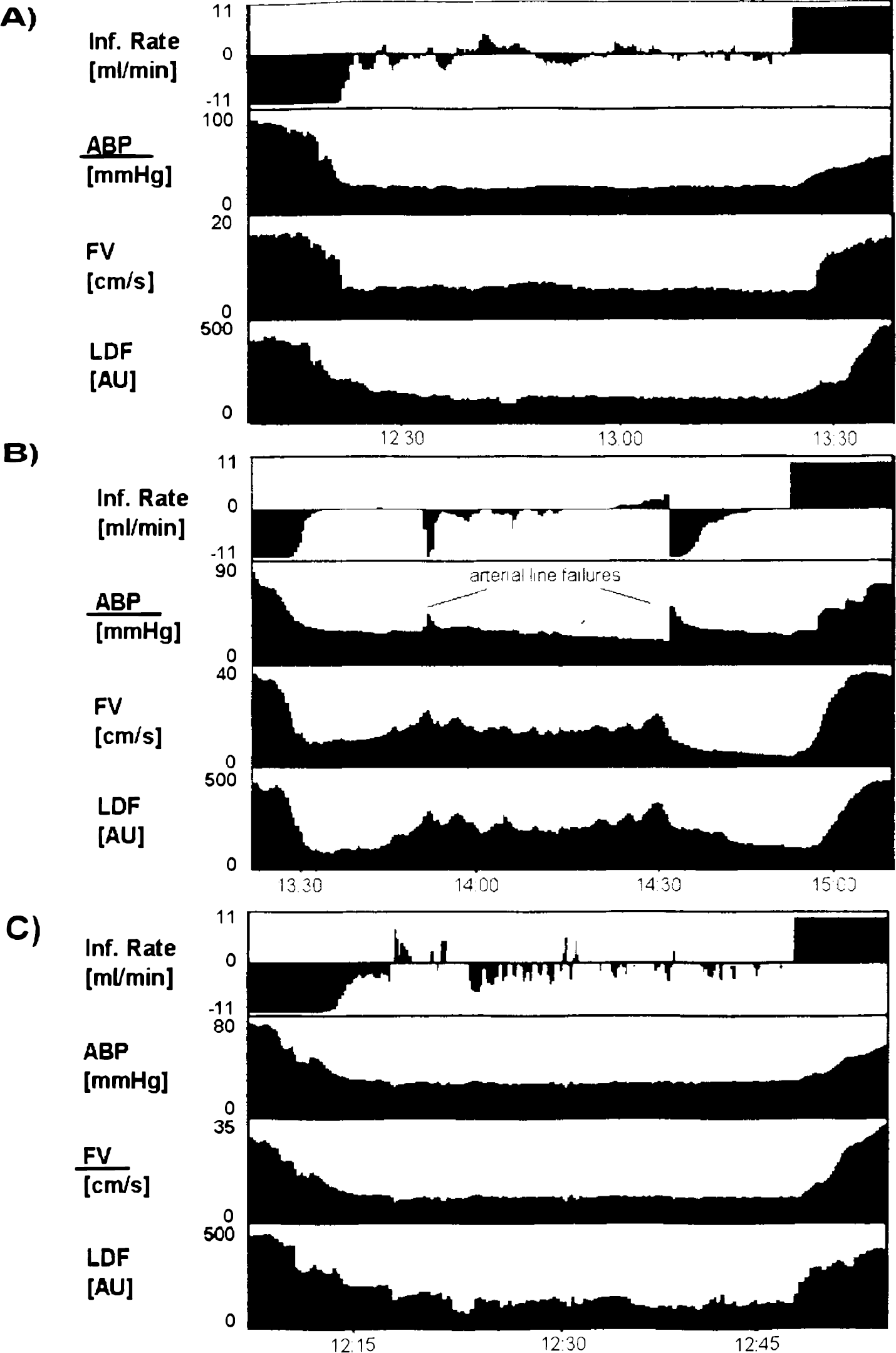
Example of three experiments assessing ability of the system to maintain stable level of severe hypotension (
Using TCD FV as the control variable. In view of the difficulties with using ABP as a control signal, the basilar artery FV was adapted as the control signal in the following five experiments (Fig. 1C). A target FV of 30% of baseline was chosen from experience gained in the initial five experiments for achieving an ABP close to 30 mm Hg. By adapting FV as a control variable, stable hypotension with an ABP close to 30 mm Hg was achieved in all five experiments. All parameters—ABP, FV, and LDF—were significantly more stable (p < 0.05) for the experiments using FV as the control signal compared with those using ABP as the control signal (Table 1).
Stability of arterial blood pressure (ABP), flow velocity (FV), and laser Doppler flowmetry (LDF) during severe hypotension (below the lower limit of autoregulation) using different controlling variables
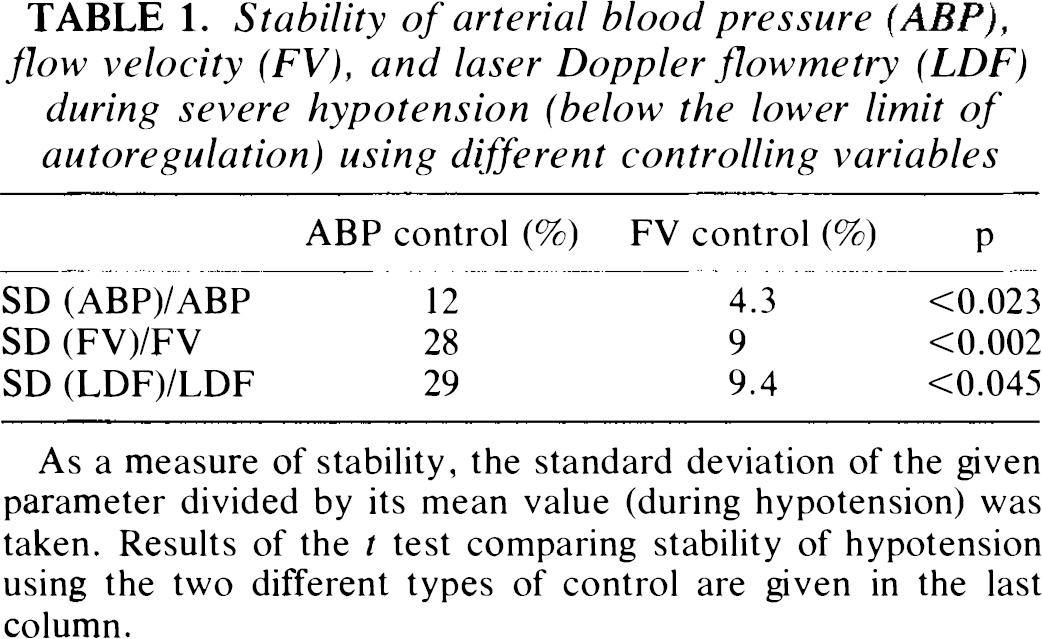
As a measure of stability, the standard deviation of the given parameter divided by its mean value (during hypotension) was taken. Results of the t test comparing stability of hypotension using the two different types of control are given in the last column.
Group B experiments
An example of ABP control during haemorrhage and subsequent FV control during reinfusion is shown in Fig. 2A. The animal's cerebral circulation demonstrated autoregulation (no correlation between ABP and LDF) until ABP decreased to 50 mm Hg (the last step), at which point LDF fell and FV started to respond passively to pressure waves. Once deep hypotension had been reached, both ABP and FV remained very stable. In contrast, when FV was used as a control variable to induce stepwise decreases in ABP in an autoregulating animal, a large volume of blood was removed before changes in FV were seen (Fig. 2B). This resulted in large changes in ABP until profound hypotension was reached. During reinfusion after the hypotensive insult, the animals displayed hyperaemia, which resulted in a disproportionately large rise in FV for a given rise in ABP (Fig. 2B)—a phenomenon well documented in the literature (Fitch et al., 1975). Using FV as a control variable therefore provided the most controlled stepwise increase in ABP and FV during reinfusion after profound hypotension.
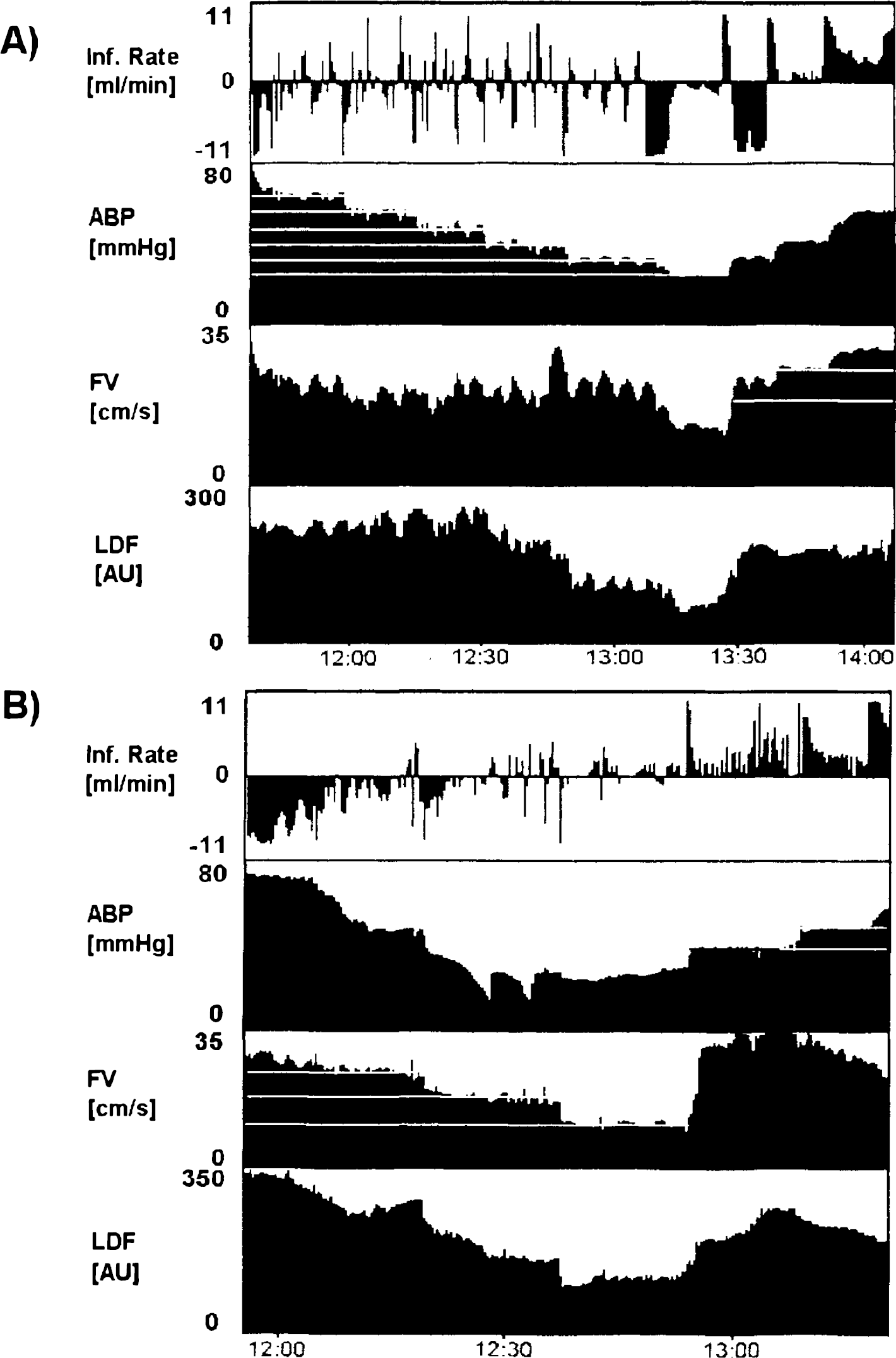
Examples of two experiments assessing the ability of the system to maintain the blood pressure at various levels during haemorrhage [
DISCUSSION
The provision of methods allowing tightly controlled hypotension of variable duration in experimental animals is important in studies of global ischaemia and for the assessment of putative brain-protective agents. Our findings indicate that a computer-driven mechanical pump with signal feedback can be used to provide highly controlled prolonged hypotension in experimental animals.
Consideration about the type of control signal is important. In our experiments the use of the basilar artery FV allows a higher degree of stability than when ABP was the feedback signal. The reason for this difference relates entirely to problems with maintaining the integrity of the ABP line. Occlusion of the arterial line prevented the system from achieving a stable hypotensive period when arterial ABP was used as a control signal. Uncontrolled rises in both the basilar artery FV and laser Doppler flux were observed in such situations. Because our initial observation indicated that the basal artery FV followed a predictable pattern during profound hypotension, we applied TCD FV as a control variable. This approach led to an improvement in the stability of controlled profound hypotension. During reinfusion of blood after a hypotensive period, our experience also indicates that the system is able to accommodate for the hyperaemic response only when FV is used as the feedback signal. In contrast, for controlling moderate hypotension in autoregulating animals only ABP can be used as the signal feedback variable because FV remains unchanged. In this range of hypotension, arterial line failure is far less likely and the ABP constitutes satisfactory feedback signal, an arrangement that proved capable of overcoming blood pressure autoregulation.
The use of laser Doppler confirmed that the system was capable of providing stable conditions of brain perfusion at the level of the capillary. The laser Doppler technique has been demonstrated in experimental animals to provide a reliable index of local capillary perfusion. Slow fluctuations of LDF demonstrated around the threshold of autoregulation (Florence and Seylaz, 1992) are commonly reflected in TCD basilar artery FV (Fig. 2B) The system provided high-quality control of both the macrovascular and microvascular circulatory blood flow.
In general the system proved to be flexible and enabled us to rapidly induce and maintain deep hypotension. We believe that the closed loop system based on TCD FV control for the induction of stable, profound hypotension is more reliable than ABP control avoiding frequent failure of the arterial line used for pressure monitoring. For experiments with moderate arterial hypotension, however, ABP control provides satisfactory stability.
Footnotes
Acknowledgment:
This study was supported by the TEMPUS program and Raymond and Beverly Sackler Studentship.