
Abstract
Objective:
This prospective cohort study aimed to determine the relationship between serum vitamin C, D, and zinc on foot wound healing and compare time to healing in individuals who are deficient versus those who have adequate levels.
Approach:
One hundred adults with foot wounds were recruited from Blacktown high-risk foot service with a follow-up period of 12 months. Serum vitamin C, D, and zinc as well as routine baseline blood testing was undertaken. Wounds were measured using a three-dimensional wound camera and classified using the Wound Ischemia and Foot Infection system at regular intervals.
Results:
Vitamin C deficiency was present in 75% of participants, 50% had vitamin D deficiency, and 38% had zinc deficiency. Diabetes was present in 91% of participants, and 50% had a history of previous amputation. Wound chronicity (
Innovation:
Deficiencies in vitamin C, D, and zinc were highly prevalent in participants with active foot ulceration. Wound chronicity was predictive of healing outcomes, highlighting the importance of rapid access to best practice care.
Conclusion:
This cohort had high deficiency rates of vitamin C, D, and zinc consistent with previous literature; however, there was no relationship between these deficiencies and wound healing or time to heal. Large randomized controlled trials are required to comprehensively determine if adequate levels of these nutrients improve wound healing outcomes.
Nada Bechara
INTRODUCTION
Wound healing is a complex process that is influenced by a range of modifiable and nonmodifiable risk factors, including nutrition. 1 Foot wounds are a common chronic wound, with most associated with diabetes but also occur as a result of neuropathy, critical limb ischemia, pressure injury, or malignancy. 2 The outcomes of chronic foot wounds can be devastating, with significant impacts on quality of life, frequent hospitalizations, lower extremity amputation, and premature death. 3 It is, therefore, important that foot wounds are managed optimally, as timely healing can reduce the likelihood of adverse outcomes. 4
Nutrition is widely recognized as an important part of managing individuals with wounds, particularly supporting vitamins and minerals that are known to be critical in wound healing. 5 A previous pilot retrospective cohort study demonstrated 86% of participants with a diabetes-related foot ulceration (DFU) had substantial vitamin C deficiency (<40 µmol/L), compared with 25% of individuals with diabetes and no foot ulceration having a vitamin C deficiency. 6 The high prevalence of micronutrient deficiency has also been reported in two larger Australian studies with 73% of participants with DFU having suboptimal serum vitamin C levels, up to 59% were vitamin C deficient, 56% vitamin D deficient, 27% zinc deficient, 11% vitamin A deficient, and 6% had low ferritin levels.7,8 Previous research has also shown that fluid and protein intake is also frequently inadequate for people with ulcers, and energy intake is commonly either excessive or inadequate relative to demands for wound healing. 9
Deficiency of vitamin C in its severest form causes scurvy. 6 Symptoms can include bleeding gums, petechiae, arthralgia, tiredness, delayed wound healing, and an ability to bruise easily. 6 Vitamin C is a co-factor in lysine and proline hydroxylation on collagen molecules, and hydroxylation of these amino acids is essential in stabilizing the triple-helix structure of mature collagen. 10 This is especially important in the proliferation phase of wound healing when fibroblasts produce collagen, which forms the scaffolding structure to support healing. Anderson advocates that vitamin C is the most essential micronutrient in wound healing because of its role in collagen synthesis and angiogenesis. 11 Zinc has roles in protein synthesis and cell replication, as well as antioxidant properties. 12 Zinc is a cofactor for many enzymes required for cell membrane repair, cell proliferation, growth, and immune system function. Zinc deficiency affects all phases of wound healing and causes a reduction in mature B cells. Vitamin D is important for normal skin function. Vitamin D binds to the vitamin D receptor through calcitriol. 13 Through this, it stimulates the production of mitogenic growth factors, epidermal growth factor receptors, and keratinocyte growth factor receptor. Previous animal studies in mice have demonstrated that deletion of the vitamin D receptor results in a number of skin problems and poor wound healing. 14
Micronutrient deficiencies are common in individuals with chronic wounds, particularly in DFU. However, it is not currently comprehensively understood if specific micronutrients impact wound healing and time to wound healing in individuals with foot ulceration. Therefore, the aim of this study was to determine the relationship between serum vitamin C, vitamin D, and zinc and wound healing in adults with an active foot wound. Furthermore, this study compared time to healing in adults with active foot ulcers and serum vitamin C, D, and zinc deficiencies versus those with adequate serum levels.
INNOVATION
To our knowledge, this is the first article looking at serum vitamin C, vitamin D, and zinc and ulcer healing trajectory. This is also the first article to assess and report on deficiency rates in this population at Blacktown Hospital. We found that vitamin C deficiency was significantly associated with a history of previous amputation.
We also found that deficiency in zinc was associated with greater wound severity according to the Wound Ischemia and Foot Infection (WIfI) classification system. Deficiency was widely prevalent, with vitamin C deficiency present in 75% of participants, vitamin D deficiency in 50%, and zinc deficiency in 38%.
CLINICAL PROBLEM ADDRESSED
Foot wounds are a common complication of diabetes, peripheral neuropathy, and ischemia. Vitamin C, vitamin D, and zinc are essential micronutrients that play a critical role in tissue repair and regeneration. However, the impact of these nutrients on foot wound healing is unclear. This study aimed to determine the relationship between serum vitamin C, D, and zinc on foot wound healing and compare time to healing in individuals who are deficient versus those who have adequate levels. Future trials should be undertaken to investigate correction of micronutrient deficiencies and healing of foot wounds.
MATERIALS AND METHODS
This was a prospective single center cohort study, which took place at Blacktown high risk foot service (HRFS) in Sydney, Australia, between August 2021 and October 2022. Ethics approval was granted by Western Sydney Local Health District Human Research Ethics Committee (Approval Number 2111-02). A convenience sample included adult participants who presented to the service with active tissue loss of the foot (defined as a break in the skin including part of the dermis, below the level of the malleoli 15 ). These participants were eligible for inclusion and provided their informed written consent. Participants were excluded if they did not attend the HRFS for follow-up to monitor healing within the 12-month study period.
Participants attended a baseline session where demographic and clinical information was collected. This included age, sex, medical history, medications, diabetes status and duration, history of vascular surgery, smoking status, history of ulceration or amputation, and whether the presenting ulcer was a first ulcer or recurrence. Microvascular complications (retinopathy and nephropathy) and macrovascular complications (cardiovascular and cerebrovascular disease) were extracted from hospital medical records. Socioeconomic status was calculated from postcodes using the Australian Bureau of Statistics Index of Relative Socio-economic Disadvantage (IRSD), with the participants’ residential postcodes populated into the interactive map and an IRSD quintile assigned with 1 being the most disadvantaged.
Height and weight measurements were extracted from hospital medical records. These measurements were taken at the patients’ most recent admission to Blacktown or Westmead Hospital using a SECA® electronic scale and stadiometer, by a registered or enrolled nurse. If patients did not have an admission within 12 months, height and weight were self-reported. Body mass index (BMI) was calculated using these measurements. Serum blood samples were taken in all participants at their initial baseline visit including vitamin C, vitamin D, zinc, full blood count, liver function tests, C-reactive protein (CRP), glycated hemoglobin (HbA1c), and kidney function tests. In the event that participants had more than one wound, the worst (highest WIfI grading and cross-sectional area) was used. Wound measurements were taken at baseline and subsequently calculated at each clinic visit, which ranged between 2 and 4 weeks apart. Number of days to wound healing was collected for all participants. An image of the wound was captured using the SilhouetteStar (ARANZ Medical, NZ), which is a three-dimensional wound camera and gives the length (mm), width (mm), depth (mm), and area (cm2) of the ulcer. This specific type of camera has been shown to have acceptable reliability and validity. 16 Wound characteristics such as etiology, location, duration, and WIfI classification were also recorded by the treating clinician. 17 Wound healing was defined as complete epithelialization (skin closure) as determined by the treating podiatrist. All wound care was standardized in line with local guidelines. 18 Best-practice knee-high offloading was offered to all patients, except those with dorsal foot wounds or in the presence of other contraindications.
Loss of protective sensation (LOPS) was determined using two testing methods, monofilament and vibration perception, with failure of either test considered indicative of LOPS. 19 A Semmes–Weinstein (North Coast Medical, USA) 10-g monofilament was tested at 10 sites of each foot, with failure to detect 4 or more locations indicative of LOPS. 19 Vibration perception was tested using a neurothesiometer (Wilford Industrial, UK) with neuropathy classified at unable to detect >25 volts. 20 Ischemia was determined using systolic toe pressures and classified using the ischemia grading in the International Working Group on the Diabetic Foot classification guidelines. 21 The Smartdop 30EX (Hadeco Inc., Japan) device, an automated photoplethysmography unit, was used to measure toe pressure on both limbs following a standardized clinical procedure. 22 If clinically indicated, patients were referred for further testing by arterial duplex at a specialist vascular lab.
Statistics
Data was entered into Microsoft Excel (Microsoft Corp., USA), where it was cleaned and prepared, with analysis performed using Statistical Package Social Science v29.0 (SPSS Science, USA). Electronic laboratory notebook platform was not used. Data were checked for normality using descriptive methods, with histograms generated to visually inspect the distribution, and skewness was computed to quantify the asymmetry. Descriptive statistics for group data were presented using frequencies and percentages or means and standard deviations. Means were compared between baseline and participants who healed at 12 months (Table 1). The relationship between vitamin C and wound healing, zinc and wound healing, and vitamin D and wound healing was explored using Spearman’s Rho correlation coefficient. Three Cox proportional hazards models were used to explore the relationship between vitamin C, D, and zinc and time to wound healing. We compared participants with adequate levels of vitamin C to those with inadequate levels, adequate levels of vitamin D to those with inadequate levels, and adequate levels of zinc to those with inadequate levels.
Participant demographic and medical characteristics
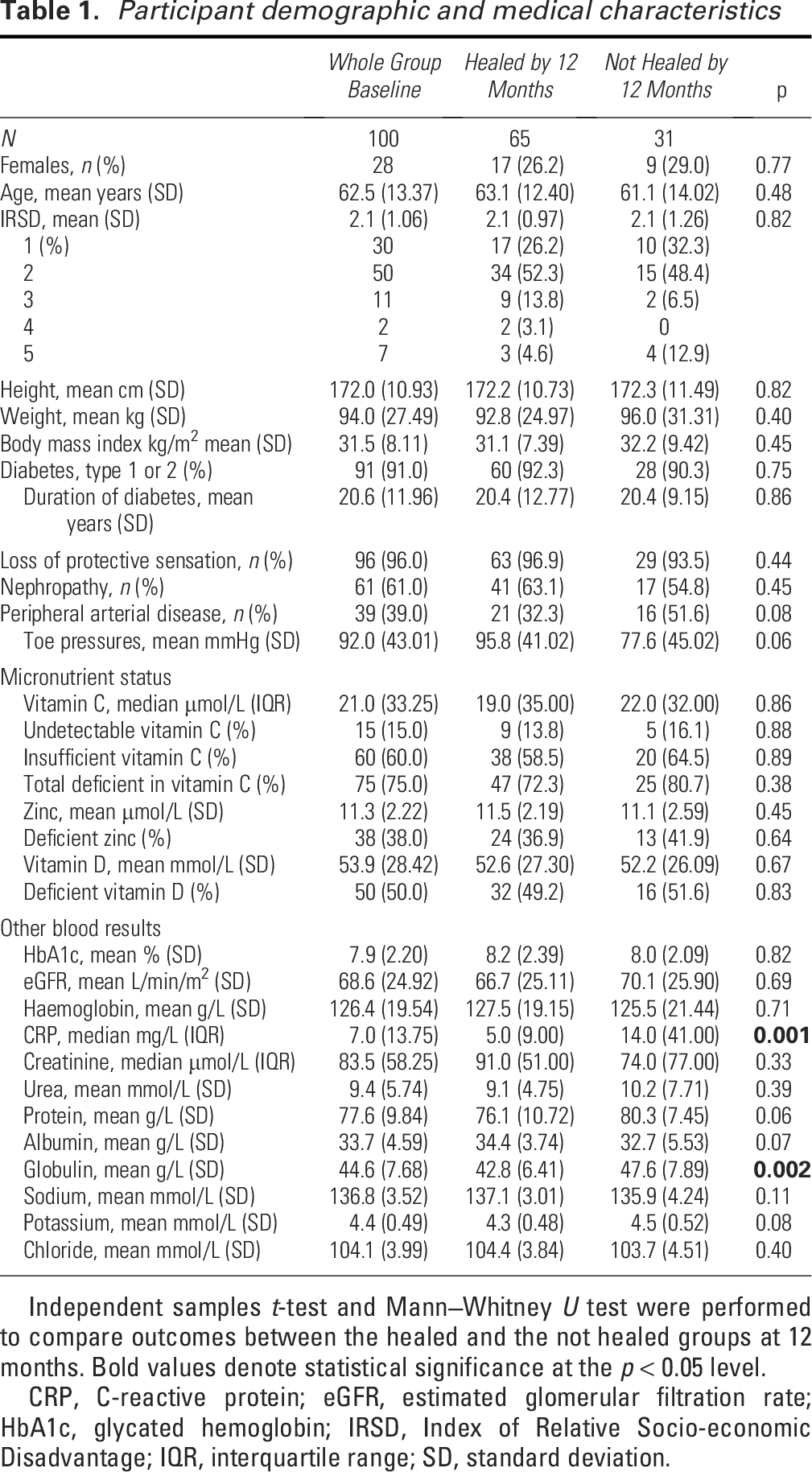
Independent samples
CRP, C-reactive protein; eGFR, estimated glomerular filtration rate; HbA1c, glycated hemoglobin; IRSD, Index of Relative Socio-economic Disadvantage; IQR, interquartile range; SD, standard deviation.
To explore the impact of a range of clinical variables on the likelihood of healing, we used a binary logistic regression model with cumulative healing at 12 months as the dependent variable. The independent variables were vitamin C, presence of diabetes, past amputation, infection, toe pressure, and age of the wound prior to baseline. Subsequent regression models were used to determine the independent contribution of zinc and vitamin D to healing, holding all other variables in the model constant. All models were checked for goodness of fit using the Hosmer–Lemeshow test. Participants lost to follow-up were excluded pairwise. The level of significance was set at 0.05 for all analyses.
RESULTS
Patient characteristics
One hundred participants were included, 72 male and 28 female with a mean age of 62 (standard deviation [SD] 13.37) years. At 12 months, 65 participants’ wounds had healed, and 31 were either not healed or had undergone an amputation. Those who were lost to follow-up were excluded from analysis (
Overall, 75% of all participants were considered deficient in vitamin C (<40 µmol/L) with a median of 21 µmol/L. Of participants with vitamin C deficiency, 15% were in the undetectable range (<5 µmol/L). Zinc deficiency (<10.7 µmol/L) was prevalent in 38% of participants, and vitamin D deficiency (<50 nmol/L) in 50%. CRP at baseline was significantly different between those who healed at 12 months and those who didn’t heal (5 mg/L vs. 14 mg/L,
Wound characteristics
Fifty participants (50%) had a history of a previous amputation at baseline and did not differ between the groups. Most common wound types were neuropathic wounds (71%), followed by neuro-ischemic (26%) and ischemic (3%). Wound location was predominantly at the plantar forefoot (44%), 57% in the healed group and 43% in the not healed group. Wound area at baseline was an average of 2.9 cm2 in those healed by 12 months and 4.8 cm2 in the not healed group (
Wound characteristics
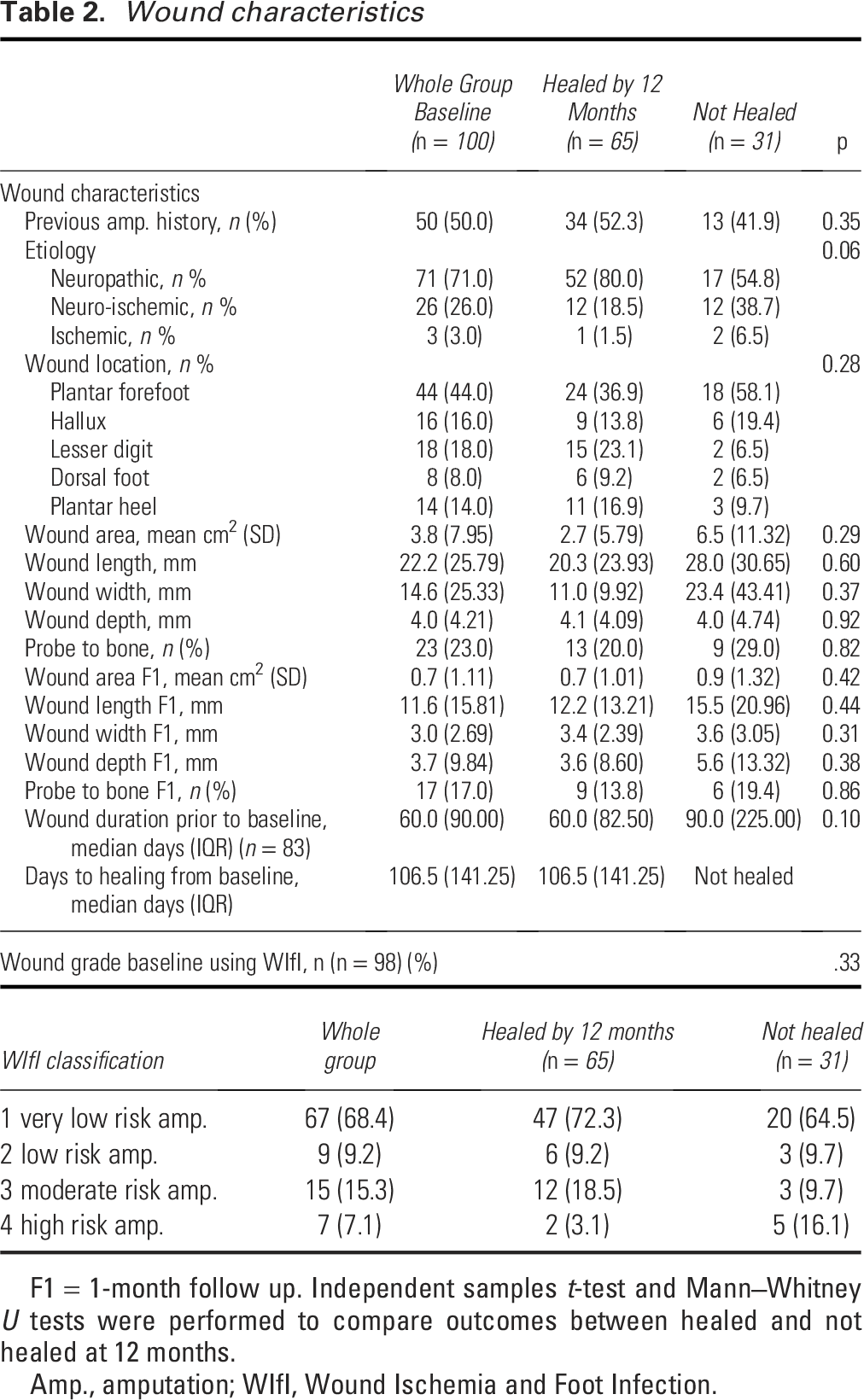
F1 = 1-month follow up. Independent samples
Amp., amputation; WIfI, Wound Ischemia and Foot Infection.
Statistics
Univariate analyses were conducted to determine the relationship between serum nutrient levels and healing using Spearman’s Rho correlation coefficient because of the data being not normally distributed. Zinc deficiency was significantly correlated with WIfI at baseline (
Results of the Cox proportional hazards model demonstrate that there were no significant differences in time to healing for participants deficient in zinc (hazard ratio [HR] 1.05, 95% confidence interval [CI] 0.94–1.17,
Factors associated with wound healing
Binary logistic regression determined the relationship between key clinical variables and the relationship to wound healing (dependent variable) (Table 3), accounting for factors known to influence wound healing. Hosmer–Lemeshow test indicated no evidence of poor fit (
Results of logistic regression models for variables in foot ulcer healing
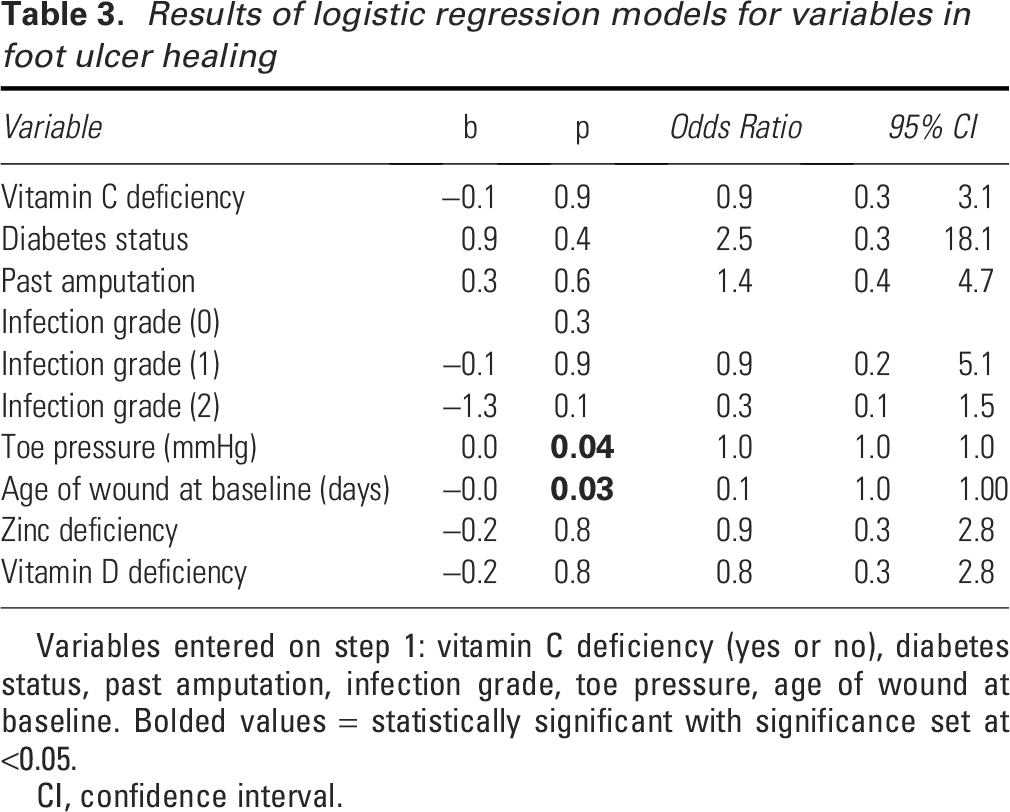
Variables entered on step 1: vitamin C deficiency (yes or no), diabetes status, past amputation, infection grade, toe pressure, age of wound at baseline. Bolded values = statistically significant with significance set at <0.05.
CI, confidence interval.
DISCUSSION
Chronic foot wounds are a challenging complication seen in patients with peripheral neuropathy, foot deformity, diabetes, and/or critical limb ischemia. To the best of our knowledge, this is the first prospective cohort study to investigate the relationship between deficiencies in serum vitamin C, D, and zinc measured and determine differences in time to healing. This study did not demonstrate any significant relationships between micronutrient deficiencies and wound healing or differences in time to healing. However, an overwhelming finding was the large proportion of participants with foot wounds and concurrent substantial deficiencies in vitamin C, D, and zinc, with some participants demonstrating vitamin C deficiencies that were considered to be so low that they were undetectable. This finding is consistent with previous cross-sectional Australian studies in patients with DFU.7,8 Given the high prevalence of nutritional deficiencies in these patients, referral to a dietitian for nutrition screening and treatment as part of a holistic wound management plan should be considered, in line with international wound healing guidelines. 5
Chronic wounds are increasing in incidence globally and markedly increase the risk of lower limb amputation and furthermore can result in prolonged hospitalizations with an increased burden to the health care system and the patient.24,25 Delayed referral to specialized wound clinics for optimal care has been demonstrated to increase time to healing, with previous research demonstrating patients referred to a specialized wound clinic after 52 days had a 58% decreased healing rate, compared with those who were referred earlier. 26 Two other studies found that the duration (age) of foot wounds was also significantly associated with healing at 52 days and the other at 20 weeks, confirming the relationship between wound duration at referral and relationship with healing.27,28 Our findings also confirm this, with a negative correlation between the age (days) of the wound at baseline measurement and healing outcomes at 12 months, indicating that wounds that were less chronic were associated with increased odds of healing. This confirmatory finding reinforces the importance of early detection and prompt referral to a multidisciplinary service for the management of foot wounds. 27 Furthermore, another confirmatory finding was that higher toe systolic pressures (per 1 mmHg) were associated with significantly increased odds of wound healing, consistent with previous studies. 29 Higher toe pressures indicate better lower limb arterial status, with lower toe pressures in conjunction with tissue loss as an indicator of chronic limb threatening ischemia, which is known to be detrimental to wound healing. 17
The current study did not demonstrate statistically significant differences in time to wound healing or demonstrate a statistically significant relationship between vitamin C deficiency and healing outcomes. However, it is not currently known if adequate serum vitamin C levels result in improved wound healing outcomes. Previous pilot studies have proposed that supplementation of vitamin C is associated with faster wound healing, with other larger cohort studies demonstrating that nutritional supplementation of any kind is associated with increased odds of wound healing.29,30 The findings of the current study suggest that adequate vitamin C was not associated with faster wound healing; however, the low numbers of participants with adequate vitamin C make it difficult to draw robust conclusions. Furthermore, the cohort design of this study does not make it possible to infer causation. There is a need for large-scale randomized controlled trials to comprehensively determine if adequate vitamin C levels are associated with more timely wound healing and furthermore determine if correction of vitamin C deficiency through medical nutrition therapy or supplementation is effective at improving wound healing outcomes.
Our study demonstrated that deficiency in serum zinc was common, a finding consistent with previous research in DFU. 31 The current study demonstrated no difference in time to healing between participants with adequate and deficient zinc levels. This differs from previous studies that have demonstrated delayed wound healing in participants with zinc deficiencies. A study conducted on patients with spinal cord injury found that zinc deficiencies were associated with poor immune function and delayed wound healing, with another study on aged care residents showing significant zinc deficiencies were associated with increased incidence of pressure injuries.32,33 Similarly, another study in a sample of 50 participants with large ulcers in the lower extremity showed zinc deficiency was associated with delayed wound healing. 34 These differences are most likely related to the different participant populations and wound types. Zinc is known to be important for healthy immune system function, playing an important role in infection and inflammation. 35 In the current study, there was a relationship between zinc deficiency and elevated CRP levels. Increased CRP levels indicate inflammation or infection systemically. 36 Zinc is proposed to provoke changes in Langerhans cells, which boost immune function exerting an anti-inflammatory effect. 37 This highlights the association between zinc and its ability to regulate inflammation and infection in the body, aiding in reduction of CRP levels.
This study demonstrated that vitamin D deficiency was associated with a 1.20 increased odds of nonhealing compared with those with sufficient vitamin D levels; however, this failed to reach statistical significance. A previous randomized controlled trial led by Razzaghi et al. in 50 participants using supplemented Vitamin D in individuals with active diabetes-related foot ulceration. The trial showed significant reductions in HbA1c levels and improved wound healing parameters over a 12-week intervention period. 38 Vitamin D is an essential nutrient, which can be obtained by exposure to sunlight, foods, and supplements. Vitamin D deficiency is frequently reported globally, with the prevalence in some countries ranging from 20% to 90%. 13 Vitamin D is proposed to have favorable effects on wound healing by stimulating phagocytosis and subsequent killing of bacteria, suppression of interferon-γ-mediated macrophage activation, and downregulation of cytokine generation. 39 The results of the current study failed to demonstrate differences in time to healing between participants with adequate vitamin D and those who were deficient.
The current study, along with multiple previous studies, has consistently struggled to demonstrate a clear substantial relationship between poor nutritional status, including deficiencies in specific nutrients, and wound healing outcomes.7,40,41 This may be due to a variety of different reasons. First, individuals with wounds tend to be complex, often presenting with multiple comorbidities, polypharmacy, complex social situations, frequently high levels of socioeconomic disadvantage, and subsequent poor health behaviors.29,42,43 Taking a reductionist approach, attempting to determine how one very specific factor contributes to an individual’s wound healing capacity is therefore challenging within such a complex clinical context. Second, it is difficult to standardize clinical care in this patient cohort, because of the variety of clinical presentations. This makes conducting trials in this cohort difficult, as being able to control for all clinical variables is not always possible. This results in more pragmatic, real-world studies being completed more frequently, such as the current study. This variety in study designs and lack of clinical trial data makes it impossible to determine causality. Finally, measuring dietary intake and nutrient deficiencies is best performed using serum blood levels; however, this is expensive, and many studies resort to patient-reported measures of dietary intake as a surrogate way to determine deficiency. This is suboptimal and contributes to the variety in results and potentially the lack of findings across many studies. Measuring nutrient deficiencies also tends to be at a single point in time, and this may vary from week to week as individuals’ diet may also vary. Therefore, although individuals may have adequate nutritional status at a single time point, this is not guaranteed to be consistent throughout their wound healing journey, which can be very long for many. Finally, measurement of the primary outcome, wound healing, is also incredibly heterogenous within the published literature, making meta-analysis difficult. Regardless, a variety of trials have attempted to address deficiencies with supplementation of various nutrients, with similarly heterogenous results. 44 Large, population-based studies, conducted across multiple sites, are required to answer this question in a robust way.
LIMITATIONS
As this was a pragmatic cohort study, all participants were offered best practice care in a homogenous clinic with standard treatment protocols, including standardized wound care; however, there may have been instances of slight variations in response to delivering person-centered care. Participants are offered gold-standard offloading (nonremovable knee-high offloading devices), but some declined or may not have been suitable and were fitted with ankle-high devices or therapeutic footwear instead. This treatment decision making is in line with current guidelines. 45 Another limitation is the high number of participants with deficiencies, making it difficult to determine how adequate micronutrient status would have influenced healing. Participants were not blinded to the aims of the study, and this may have influenced behavior over the study period. However, given the long follow-up period, this is unlikely to have influenced results. Furthermore, participants may have taken vitamin supplements during the trial period without the knowledge of researchers; however, this is unlikely and, again, given the long follow-up period, unlikely to have influenced results. Finally, our results demonstrate wide CIs indicative of imprecision related to our small sample, and therefore, results are preliminary and should be interpreted with caution. Strengths of the study include the pragmatic nature of the research in a real-world cohort, the prospective design with extensive and regular follow-up points, the use of serum blood levels to measure nutrient deficiency, and the standardized delivery of care.
Future trials looking to address micronutrient deficiencies in individuals with foot ulceration should be of large scale, preferably multicenter, and look at medical nutrition therapy or micronutrient supplementation and the effects on healing of foot ulceration over a period of time. Recurrence is also of interest, and secondary analysis of the current cohort may elucidate if micronutrient deficiencies are associated with recurrence of DFU. This future research may have the ability to strengthen the evidence that is currently available and, in turn, improve outcomes for those with foot wounds and reduce amputation rates.
ACKNOWLEDGMENTS AND FUNDING SOURCES
This work was supported by the
Serum vitamin C deficiency was present in 75% of participants, 50% had vitamin D deficiency, and 38% had zinc deficiency. Wound chronicity and toe pressures were predictive of wound healing at 12 months. There was no significant difference in time to healing between individuals with adequate levels of vitamin C, D, or zinc and those with adequate levels. Inadequate levels of vitamin C, D, or zinc were not associated with healing outcomes at 12 months.KEY FINDINGS
AUTHOR DISCLOSURE AND GHOSTWRITING
There are no ghostwriters involved in the writing of this paper.
ABOUT THE AUTHORS
AUTHORS’ CONTRIBUTIONS
N.B.: Conceptualization, methodology, software, validation, formal analysis, investigation, resources, data curation, writing—original draft, writing—reviewing and editing, visualization, project administration, and funding acquisition. P.T.: Methodology, software, validation, formal analysis, data curation, writing—original draft, writing—reviewing and editing, visualization, supervision, and project administration. J.E.G.: Conceptualization, methodology, data curation, writing—reviewing and editing, supervision, and project administration.