
Abstract

Introduction:
In recent years, endoscopic interventions have evolved as an effective alternative to treat esophageal anastomotic leaks. 1,2 Self-expanding fully or partially covered metal (SEMS) are now the first-line therapy. 3,4 Endoscopic vacuum therapy (EVT) has been introduced as an effective therapy for anastomotic leakages following esophageal resections. 5 Negative pressure therapy prevents bacterial contamination, clears secretions, and promotes perfusion and granulation. 6,7 This video illustrates EVT in a patient with an esophageal leak.
Methods:
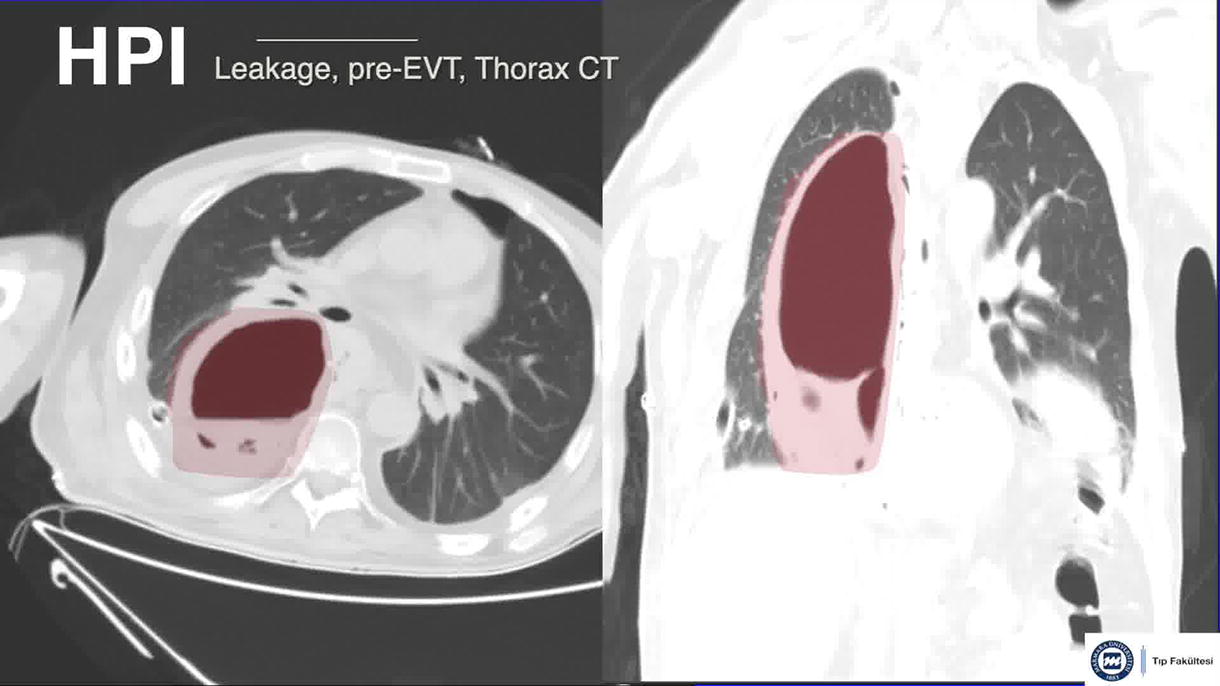
A 45-year-old male was admitted with dysphagia and vomiting. Endoscopy showed a 2 cm long circular lesion at 35 cm and biopsy confirmed adenocarcinoma. After neoadjuvant chemoradiotherapy, patient underwent an Ivor-Lewis procedure. An anastomotic leak was detected on postoperative day 9. Nonoperative management including NPO, nasogastric decompression, antibiotics and placement of drainage catheter were not sufficient for healing. Under conscious sedation, a nasogastric tube was inserted through the nose and exteriorized orally. A sponge trimmed to the size of the defect was secured to the end of the nasogastric tube and fixed with a suture. An additional suture loop was placed at the end of the sponge. This loop was grasped with endoscopic forceps and placed in the leak cavity. Negative pressure generated by an electronic vacuum pump system was applied via the nasogastric tube.
Results:
The sponge was changed twice a week for 1 month with pressure values of 75 or 100 mmHg. After 1-month, oral feeding was well tolerated by patient. Patient refused adjuvant treatment with no oncologic progression over 6 months. The leak was well healed based on radiographs, computed tomograms, and endoscopy at 6 months.
Conclusion:
EVT has the potential to replace SEMS therapy for esophageal anastomotic leaks. 8 –10 Recent meta-analyses reported that, EVT has a significantly higher success rate for esophageal leaks with lower major complications and mortality rates compared with SEMS. 11,12 Extensive data regarding EVT for esophageal anastomotic leaks is lacking and randomized controlled studies comparing SEMS and EVT may be necessary. 8
None of the authors have any competing financial interests
.
Exact Running Time:
08:31 minutes
Runtime of video:
8 mins 31 secs
Get full access to this article
View all access options for this article.