
Abstract
Introduction:
Retzius-Sparing robotic assisted radical prostatectomy (RS-RARP) is a safe and efficient approach to treat localized low- and intermediate-risk prostate cancer. 1 An RS-RARP may be associated with shorter continence recovery times with similar oncologic outcomes. Initial reports described an intrafascial plane resection, but patients with extraprostatic extension are not ideal candidates to the current technique. 2,3 There are two recent series reporting RS-RARP in high-risk patients, 4,5 but the literature lacks a detailed surgical guide suitable for locally advanced disease. This video describes a modified surgical technique applied to high-risk prostate cancer to achieve negative surgical margins.
Materials and Methods:
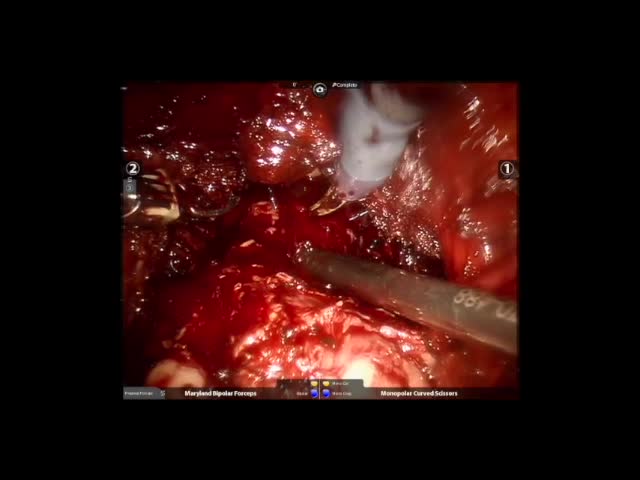
Cohort analysis of 45 men with nonmetastatic high-risk prostate cancer, who underwent RS-RARP extrafascial dissection as first-line treatment. Twelve patients underwent unilateral bundle preservation. In brief, the rectoprostatic space is developed through the prerectal fat within an extrafascial posterior plane. The anterior and lateral isolation of the prostate are performed after the periprostatic fat plane. Lateral dissection of the prostate surface is performed to open the endopelvic fascia to isolate the neurovascular pedicles. The pedicles are ligated and divided without neural preservation. In selected cases, bundle preservation is possible. The apex is isolated, and the dorsal venous complex is ligated and divided above the anterior surface of the prostate. The urethra is incised after elongation without impinging on the apical margins. The vesicourethral anastomosis is performed using a continuous barbed suture and reinforced by a modified Rocco stitch and suture of the posterior peritoneum.
Results:
At 1 and 12 months after surgery, 73% and 93% of the men used one safety pad or less, respectively. No major complication or blood transfusions were reported. Fifty percent of the nerve sparing group reported adequate erectile function. Pathology report showed pT2 31%, pT3 58%, and pT4 11%. The mean prostatectomy Gleason 8, mean lymph nodes 22, mean positive surgical margins 28%, and positive lymph nodes were identified in 14%. At a minimum follow-up of 1 year, there were no oncologic-related deaths.
Conclusion:
RS-RARP provides favorable continence and oncologic outcomes in high-risk cases. Further well-designed studies are necessary to validate our oncologic outcomes.
No competing financial interests exist.
Runtime of video: 9 mins 10 secs

Get full access to this article
View all access options for this article.