
Abstract
Background
Patients with hematologic malignancies undergo splenectomy for both diagnostic and therapeutic purposes. Although minimally invasive surgery continues to be increasingly utilized for a variety of abdominal operations, no large-scale data has compared the postoperative outcomes for laparoscopic vs open splenectomy in patients with hematologic malignancy.
Methods
Patients with a diagnosis of hematologic malignancy who underwent laparoscopic and open splenectomy between 2015 and 2020 were queried using the ACS-NSQIP database. 30-day outcomes of laparoscopic vs open splenectomy were compared.
Results
Out of 430 patients included in the study, 52.6% were male, with a mean age of 63.4 ± 13.1 years. 233 patients (54.2%) underwent laparoscopic splenectomy. On bivariate analysis, laparoscopic surgery was associated with lower rates of 30-day mortality [2.1% vs 11.7% (P < .001)] and morbidity [9.0% vs 24.4% (P < .001)]. On multivariate regression, elective operations (OR .255, 95%CI: 0.084-.778, P = .016) and laparoscopic surgery (OR .239, 95%CI: 0.075-.760, P = .015) were independently associated with lower mortality, while history of metastatic cancer (OR 3.331, 95%CI: 1.144-9.699, P = .027) was associated with higher mortality. Laparoscopic surgery (OR .401, 95%CI: 0.209-.770, P = .006) and steroid use (OR 2.714, 95%CI: 1.279-5.757, P = .009) were the only two factors independently associated with 30-day morbidity. Laparoscopic surgery was also associated with shorter hospital length of stay (median 3 [IQR:3] vs 6 [IQR:7] days).
Conclusion
Laparoscopic splenectomy was associated with lower 30-day mortality and morbidity, and shorter length of stay in patients with hematologic malignancies. These data suggest that laparoscopic approach, when feasible, may be preferred for splenectomy in this patient population.
Background
Patients with hematologic malignancies have been found to suffer from a nearly five times greater risk of mortality following surgery compared to the average patient. 1 For the general surgeon, caring for these patients is an uncommon and challenging endeavor particularly with regards to splenic pathology. Hematologic malignancies including lymphoma, leukemia, multiple myeloma, and other myeloproliferative disorders can lead to tumor infiltration of the spleen, symptomatic splenomegaly, or atraumatic splenic rupture—all of which can mandate splenectomy. This study sought to find differences in surgical practice patterns that could help mitigate the surgical risk encumbered by these patients from their systemic disease.
Although laparoscopy has become increasingly utilized for other procedures, the gold standard for splenectomy, in patients with hematologic malignancies or those who require tissue diagnosis of lymphoma, remains via laparotomy.2,3 While current trends in the general surgical patient undergoing splenectomy favors laparoscopic vs open splenectomy with regards to postoperative outcomes, 4 there is a paucity of data on the use of laparoscopy in patients with hematologic malignancy.
The objective of this study was to compare the laparoscopic approach to open approach for splenectomy in patients with hematologic malignancy. It was hypothesized that in this higher-risk patient population, laparoscopic surgery would be associated with reduced postoperative morbidity and mortality.
Methods
The Institutional Review Board at the Lundquist Institute at Harbor-UCLA Medical Center deemed this study as non-human subject. Patients with a diagnosis of hematologic malignancy (lymphoma, leukemia, multiple myeloma; ICD-10 codes C81-C96) who underwent laparoscopic or open splenectomy (CPT codes 38120, 38100) between 2015 and 2020 were queried using the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database.
All patients who underwent both elective and non-elective splenectomy were included. Patients were excluded if data was missing in the database set. Data was collected on patient demographics (sex, age, medical comorbidities), preoperative laboratory values (hemoglobin, platelet level, white blood cell count), preoperative events (transfusion history, presence of sepsis), whether surgery was elective vs non-elective, emergency vs non-emergency surgery, and perioperative morbidity and mortality.
The primary outcome was 30-day mortality. Secondary outcomes included overall 30-day morbidity, hospital length of stay, postoperative surgical site infection (SSI), and postoperative septic shock. 30-day morbidity was defined as the composite rate of postoperative complications present in the ACS-NSQIP database.
Continuous variables are shown as means with standard deviations and were analyzed using Student’s t-test. Continuous variables that have non-normal distributions are shown as medians with interquartile ranges. Categorical variables are shown as percentages and were analyzed using Pearson Chi-squared test or Fisher’s exact. Logistic multivariate regression was used to determine which variables were independently associated with postoperative morbidity and mortality. Statistical significance was defined as P-value <.05. All statistical analysis was performed using SPSS V24 (IBM Corp, Armonk, New York).
Results
Demographics and Preoperative Data for Patients with Hematologic Malignancy Undergoing Splenectomy.
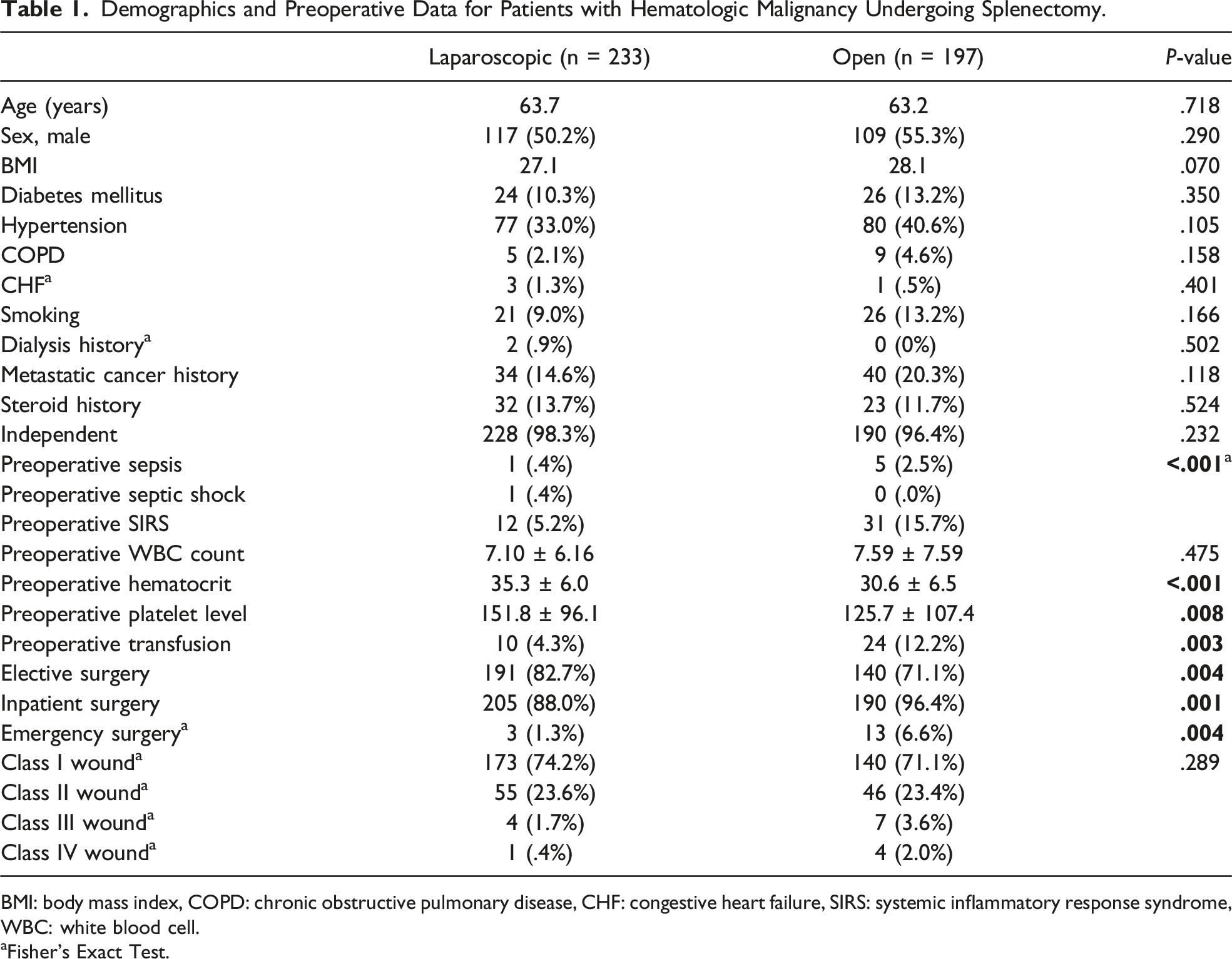
BMI: body mass index, COPD: chronic obstructive pulmonary disease, CHF: congestive heart failure, SIRS: systemic inflammatory response syndrome, WBC: white blood cell.
aFisher’s Exact Test.
Postoperative Outcomes for Patients with Hematologic Malignancy who Underwent Splenectomy.
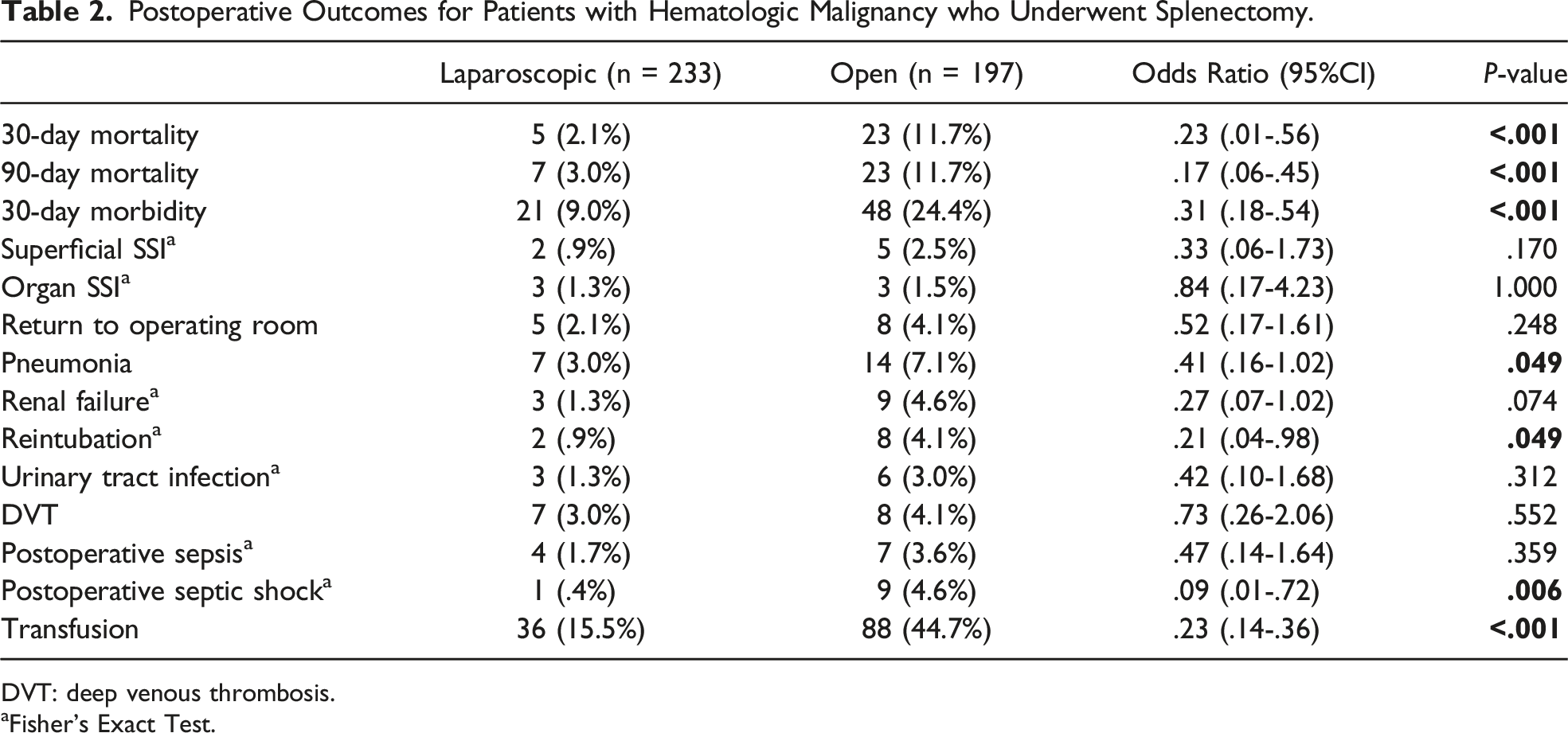
DVT: deep venous thrombosis.
aFisher’s Exact Test.
Laparoscopic surgery was also associated with lower overall postoperative 30-day morbidity [9.0% vs 24.4% (P < .001)]. On multivariate regression, laparoscopic surgery (OR .401, 95% CI: 0.209-.770, P = .006) was independently associated with lower 30-day morbidity while steroid use (OR 2.714, 95% CI: 1.279-5.757, P = .009) was independently associated with higher morbidity.
From a blood count standpoint, white blood cell count was similar in the laparoscopic and open groups [7.10 ± 6.16 vs 7.59 ± 7.59 (P = .475)]. Both preoperative hematocrit [35.3 ± 6.0 vs 30.6 ± 6.5 (P < .001)] and platelet level [151.8 ± 96.1 vs 125.7 ± 107.4 (P = .008)] were higher in the laparoscopic surgery group.
Laparoscopic splenectomy was associated with a shorter hospital length of stay [median 3 days (IQR:3) vs 6 days (IQR:7)]. Additionally, mean operating times were longer for laparoscopic splenectomy compared to open splenectomy [159.1 ± 81.2 vs 131.1 ± 54.9 minutes (P < .001)].
Rates of preoperative sepsis, septic shock, and systemic inflammatory response syndrome (SIRS) were higher in the open surgery group (Table 1). Rates of SSI (superficial or organ space) did not differ significantly between laparoscopic and open surgery patients (Table 2). No patients had a deep SSI in either group.
Discussion
In patients with hematologic malignancies undergoing splenectomy, laparoscopic approach was found to be associated with lower rates of postoperative morbidity and mortality. Minimally invasive surgery has continued to be increasingly utilized for a variety of abdominal operations. However, there is no study using large-scale data that has compared the postoperative outcomes for laparoscopic vs open splenectomy in patients with hematologic malignancy. These patients are different from the typical patient as they often have widespread disease associated with bone marrow infiltration and subsequent aberrancies in the various blood cell lines including leukopenia, leukocytosis, anemia, and thrombocytopenia. Whether on chemotherapy or not, given the proliferation of dysfunctional, immature white blood cells or clonal production of diseased myeloid cells, hematologic malignancies confer an elevated infection risk and poorer nutritional status to patients. 5
The mortality difference found between the laparoscopic and open groups could be explained by multiple findings. Open surgery patients had higher rates of postoperative pneumonia, a finding that is consistent with the current literature that shows laparotomy has been linked with a higher rate of postoperative pneumonia in patients undergoing abdominal surgery.6,7 This complication has been shown to be associated with a nearly 30% risk for postoperative mortality. 8 Open surgery patients also had higher rates of septic shock which could explain the mortality difference as postoperative sepsis is also a known risk factor for mortality following surgery. 9 In examining the higher rate of septic shock following open splenectomy, it is difficult to speculate why this occurred with more frequency in the open surgical group. Multiple studies have found greater pro-inflammatory states in open vs laparoscopic surgery.10,11 A dysfunctional immune response in patients with hematologic malignancy who have poorer physiologic reserve and reduced ability to combat infection could be an explanation. Clearly, further research is needed to determine if the source of septic shock in these post-splenectomy patients was intraabdominal, pulmonary, blood stream related, or from other locations.
There are numerous reasons why laparoscopic surgery was associated with improved outcomes when compared to open abdominal surgery in this cohort. Laparoscopic approach is usually associated with less intraoperative blood loss (as was in this cohort), lower postoperative pain scores, and lower rates of wound complications. 12 Interestingly, the 90-day mortality rate did not significantly differ clinically from the 30-day mortality rate between patients undergoing surgery, suggesting that the majority of poor postoperative outcomes happened in the short-term instead of long-term. This finding emphasizes the importance of providing surgical options for patients with the lowest rate of short-term mortality.
While the findings of the study show significant mortality and morbidity advantages with laparoscopic splenectomy, it is unknown in which patients the different surgical approaches were used. Because many patients with hematologic disease undergo splenectomy for therapeutic purposes due to symptomatic splenomegaly, it is likely that this was the indication for many of the non-emergency surgeries. Historically, splenomegaly has made it significantly more challenging to perform splenectomy laparoscopically and an open approach was favored. However, recent studies including a systematic review and meta-analysis by Rodriguez-Luna et al showed that laparoscopic splenectomy was safe in patients with splenomegaly with a median size of 22.5 cm. 4 Nevertheless, technical limitations to laparoscopic surgery including increased operative difficulty from unfavorable anatomy may have led to more challenging operations being performed via an open approach.
Data was not available on splenic size and this factor was not able to be controlled for in this study. In examining surrogates for splenic size, splenomegaly and hypersplenism are often accompanied by laboratory derangements. Values such as platelet level and hemoglobin, however, have not been found to reliably correlate to spleen size and were therefore not used as surrogates for splenomegaly. 13 However, patients in the open surgery group had lower preoperative hematocrit and platelet levels which has been associated with a more severe phenotype or stage of hematologic malignancy14,15 that could have led to a difference in outcomes. Although the specific indication for emergency surgery is not provided in the NSQIP database, emergency open splenectomy—which was associated with lower preoperative hematocrit and platelet levels—may have been performed due to splenic hemorrhage.
Limitations to this study include its retrospective nature and the selection bias that accompanies a database study. Although the rate of surgical site infection was higher in the open splenectomy group, the difference was not statistically different. Importantly, wound classification did not differ significantly between the open and laparoscopic surgery groups and therefore did not have a major impact on the postoperative SSI rate. The findings of this study are consistent with current literature on the rate of SSI following laparoscopic and open splenectomy,16–18 but if the study had higher power, a statistical difference may have been detected. Furthermore, because the NSQIP database phased out the variable for preoperative chemotherapy use, this study was not able to control for this confounding factor. Additionally, specific postoperative complications such as pancreatic leak or fistula and intraabdominal bleeding requiring return to the operating room were not recorded in the database.
The results from this study must be used appropriately—although laparoscopic approach was shown to have improved outcomes, it is unclear what anatomic or technical expertise limitations led to the surgeon’s choice of approach. Additionally, it is unknown if cases coded as laparoscopic included hand-assisted laparoscopy or not, an important subset of minimally invasive procedures which may have different outcomes when compared to standard laparoscopic surgery alone. Laparoscopic surgery should only be performed in the hands of experienced surgeons, particularly in cases of splenomegaly.
Conclusion
In this study, laparoscopic splenectomy for patients with hematologic malignancy was associated with improved postoperative mortality and morbidity. This data suggests that when feasible, laparoscopy may be the preferred approach for this subset of patients undergoing splenectomy.
Footnotes
Author Contributions
Naveen Balan: study design, data analysis, manuscript writing and editing
Christian M. deVirgilio: manuscript writing and editing
Junko Ozao-Choy: manuscript writing and editing
Ashkan Moazzez: study design, data analysis, manuscript editing
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Disclaimer
The American College of Surgeons National Surgical Quality Improvement Program and the hospitals participating in the ACS NSQIP are the source of the data used herein; they have not verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors.