
Abstract

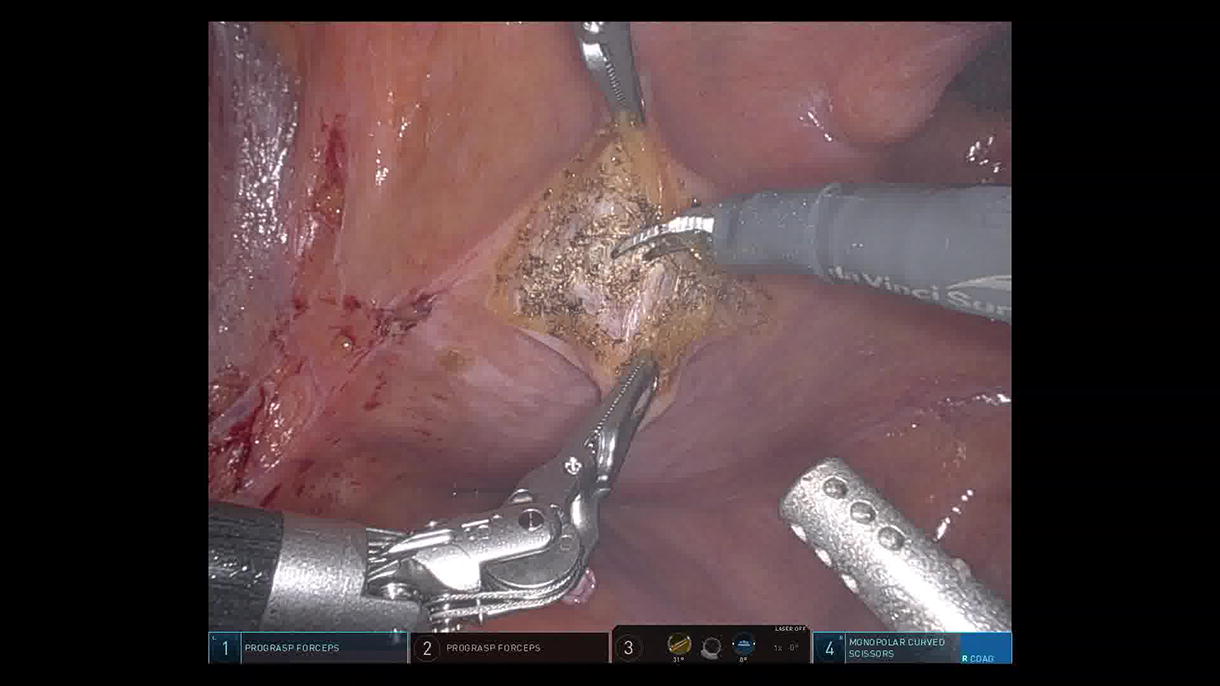
This is the unique case of an octogenarian male who presented with 122 bladder stones managed via robot-assisted laparoscopic (RAL) cystolithotomy. Medical history included multiple comorbidities such as nephrolithiasis, hypertension, diabetes, hyperlipidemia, and coronary artery disease treated surgically with coronary artery bypass graft on antiplatelet therapy. The patient’s preoperative workup included a computed tomography (CT) that revealed innumerable 10 mm bladder stones filling the entire bladder volume; interestingly, the patient was able to void appropriately before surgery. He was taken to the operative theater and was placed in a supine position; a 16 French Foley catheter was inserted under sterile conditions. The abdomen was insufflated in the standard fashion using the Veress needle. A supraumbilical trocar site for the camera was utilized and positioned with an 8-mm port. On either side of the midline trocar site approximately 8 cm away, the robotic 8-mm trocars were inserted under direct vision. An additional 8 mm robotic trocar was inserted on the left side for the 4th robotic arm. On the patient’s right lateral side, a 12 mm trocar was inserted under direct vision as the assistant port. A 0-Vicryl suture was placed in the 12 mm trocar location with the Carter Thomason device for closure at the end of the case. During placement of trocars, the patient was in a steep Trendelenburg position. At this point, a transverse bladder incision was made. The bladder was irrigated with 120 mL of normal saline. Upon entering, there were innumerable 10 mm bladder stones. Further visualization revealed an enlarged prostrate with an intravesical median lobe. At this point, all the bladder stones were removed intact with the assistance of a ProGrasp™ forceps and a fenestrated bipolar and placed into an EndoCatch™ bag. Hemostasis was obtained with electrocautery. A final 16-Fr Foley catheter was introduced in the bladder. At this point, a cystorrhaphy was performed with 3-0 V-lock sutures in a running fashion. The peritoneum was closed with another layer using 3-0 V-lock suture. The bladder was inflated, and there was no leak identified. There appeared to be a watertight anastomosis with no significant clots or hematuria. The procedure took 180 minutes with minimal blood loss. Given his age and comorbidities, he was admitted for overnight observation for a total length of stay of <24 hours. The critical Foley was removed on postoperative day 14 at his next office visit with no need for prior cystogram. The stone analysis returned as uric acid dihydrate (80%) and calcium oxalate monohydrate (20%), accounting for a total weight of 132.26 grams. RAL cystolithotomy is a safe and effective minimally invasive approach for the management of exceedingly large bladder stone burden, demonstrated by a stone-free outcome in postoperative CT scan follow-up. This approach also avoids the inherent risks of urethral stricture and bladder neck contracture, which can result from repetitive scope passage with alternative endoscopic modalities.
Author Disclosure Statement:
The authors of this article have no commercial associations during the last two years that might create a conflict of interest in connection with the video.
Statement:
We the authors of this video have received and archived patient consent for video recording/publication in advance of video recording of procedure.
Runtime of video: 4 mins 37 secs.
Get full access to this article
View all access options for this article.