
Abstract
A 42-year-old female presented at the urology clinic for evaluation of an incidentally discovered 4.6 × 2.8 cm right solid renal mass. Her medical history was significant for of severe obesity, c-section, gastric bypass, abdominoplasty, and appendectomy. The patient underwent a CT-guided renal biopsy, revealing grade 2 clear cell renal cell carcinoma. After discussing surveillance versus intervention, she ultimately chose to pursue a single-port retroperitoneal robot-assisted partial nephrectomy.
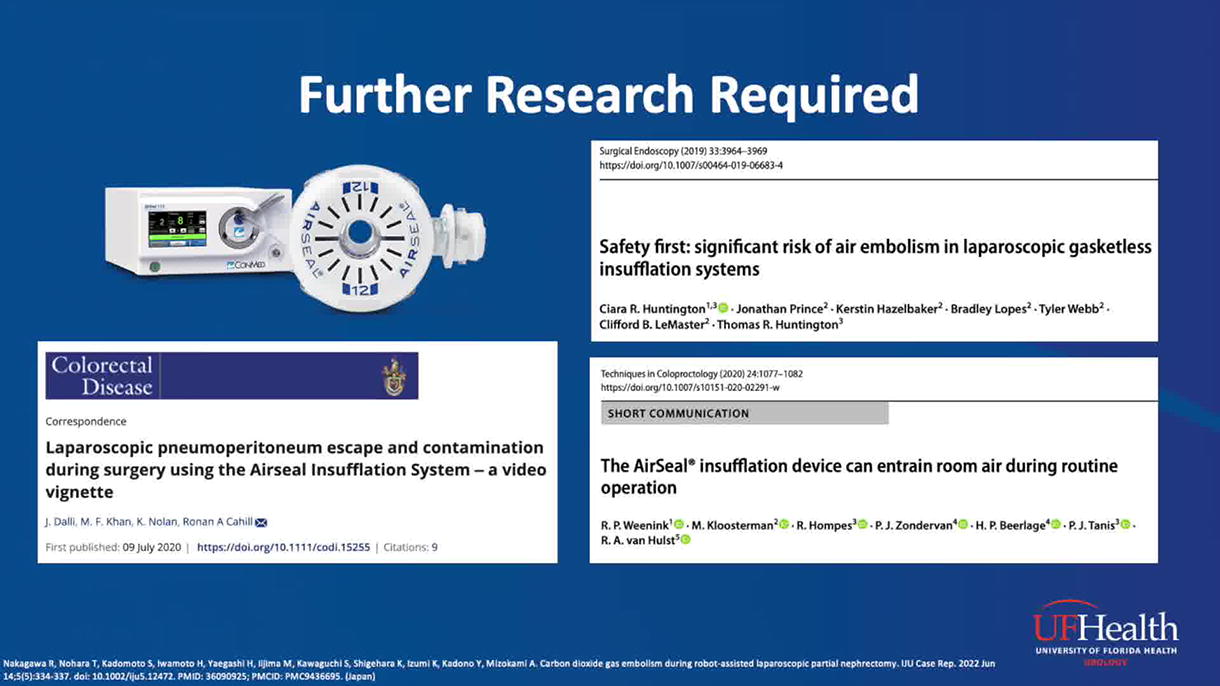
During surgery the hilar vessels were isolated and given the exophytic nature of the mass with lower bleeding risk an off-clamp tumor excision was deemed appropriate to maximize preservation of renal function. Excision was performed at an insufflation pressure of 15 mmHg, with intermittent suctioning from the remotely operated suction irrigation system (ROSI) tube to maintain a clear visual of the surgical field. During excision, bubbles were noted emanating from the venous sinuses of the resection bed. This phenomenon was the first indication of gas embolism, likely caused by the intermittent gas and blood exchange in the venous sinus resulting in some of the gas entering and exiting from the sinus. Simultaneously, the anesthesia team noted concern for CO2 gas embolism due to an abrupt onset of hypotension and loss of end-tidal CO2, indicative of a V/Q mismatch.
The resection bed was packed with Tachosil® and gauze, and insufflation was turned off. The patient’s hemodynamic status recovered after a few minutes, and re-insufflation was attempted at a lower pressure of 8 mmHg. The packed gauze was removed, and excision was resumed; however, due to recurrence of bubbling and dropping end-tidal CO2, the surgery was converted to on-clamp open partial nephrectomy.
The mass was excised with negative margins and confirmed to be the clear cell subtype. The patient was extubated without incident and kept overnight in the PACU for observation. She maintained stable vitals with no further concerns and was discharged home the next day. At her 1-month follow-up, she had made a complete recovery. To prevent future incidences of gas embolism during such procedures, (1) operate at the lowest possible insufflation pressure, especially in small spaces such as the retroperitoneal cavity, and (2) utilize intermittent suction sparingly versus frequent or continuous suction to reduce variability in insufflation pressure and flow rate.
Source of work:
University of Florida, Shands Hospital. There are no conflicts of interests or obligations resulting from the source of the work.
Author Disclosure Statement:
The authors do not have any commercial associations that might create a conflict of interest in connection with the video.
Authors have received and archived patient consent for video recording/publication in advance of video recording of procedure.
Runtime of video: 5 mins 0 secs.
*Presented at the 2024 FTS-SURS Joint Meeting
Get full access to this article
View all access options for this article.