
Abstract

Objectives:
To investigate the strategies to optimize surgical exposure during retroperitoneal robotic partial nephrectomy for complex renal tumors, and verify its clinical significance.
Methods:
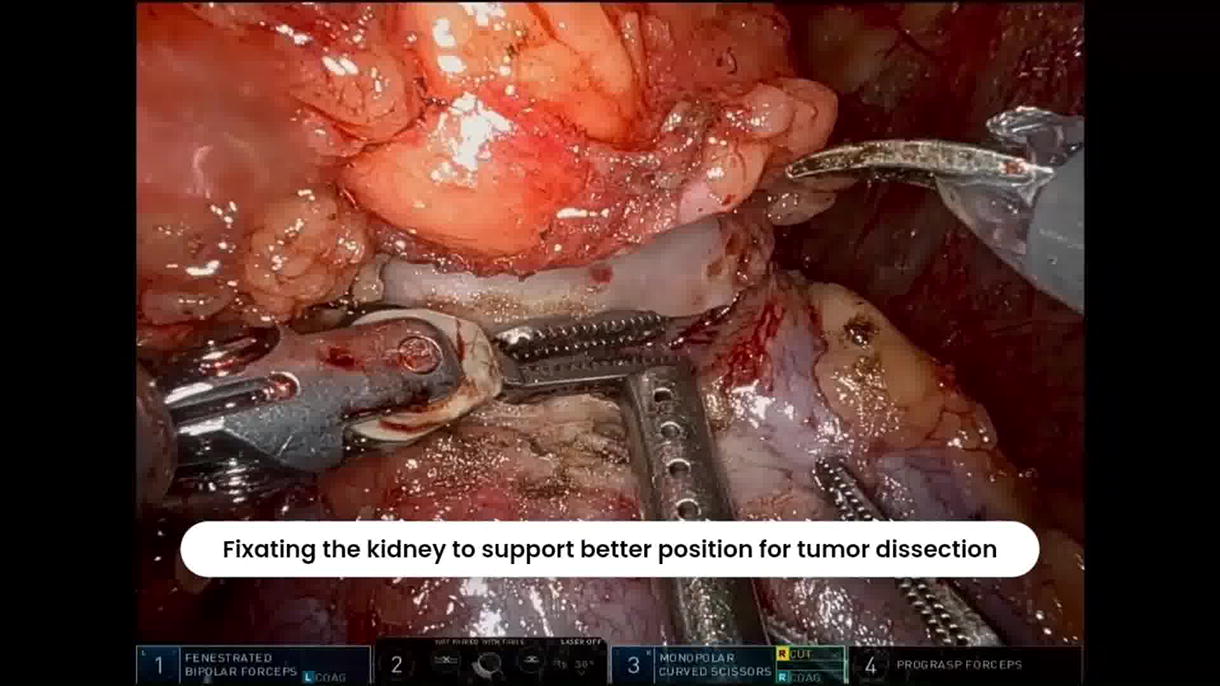
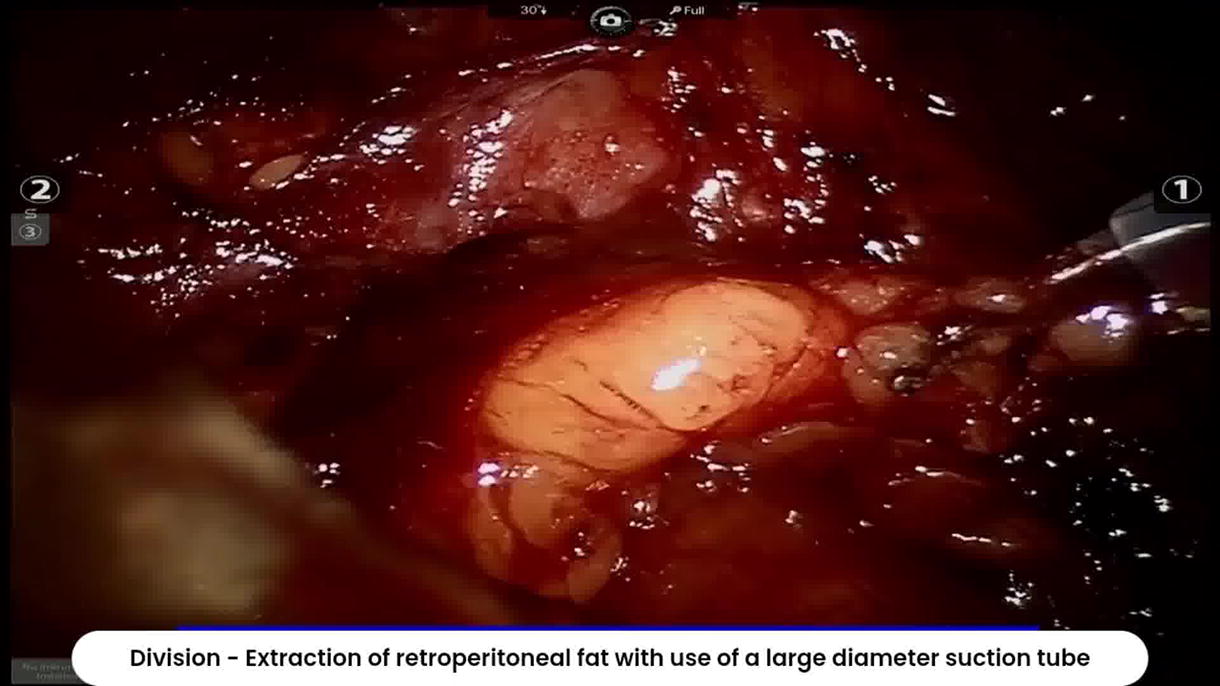
From January 2019 to August 2024, we retrospectively analyzed the clinical data of 201 patients who had undergone retroperitoneal robotic partial nephrectomy (rRPN) performed by the same console surgeon, with or without the “ASMD” techniques to optimize surgical exposure. The ASMD technique, named after the four basic arithmetic operations (i.e., addition, subtraction, multiplication, and division), resembles four techniques adopted for different situations during rRPN. The A (addition) technique is featured by addition of auxiliary instruments, e.g., the 4th robotic arm or additional suspension devices, so as to provide more tension for hilar mobilization and reduce visual obstruction of the peritoneal reflection; the S (subtraction) technique is featured by additional anatomical dissection of the peritoneal reflection, to push the peritoneum away from the Gerota or Zuckerkandl fascia; the M (multiplication) technique is featured by a hybrid, or posterior transperitoneal access to amplify the retroperitoneal space; and finally the D (division) technique, is featured by maximal extraction of retroperitoneal fat with use of a large diameter suction tube or GelPOINT Mini single-site port. Patients included in the present study were all with clinically identified renal tumor with a R.E.N.A.L. score of ≥7. Baseline data, operative time, warm ischemia time, estimated blood loss, postoperative complication and length of hospital stay, were collected.
Results:
A total of 96 patients in ASMD group and 105 patients in standard technique group were included. All procedures were carried out successfully without conversion to open surgery or total nephrectomy. The body mass index (BMI) of the two groups were (24.2 ± 4.4) kg/m2 and (23.5 ± 4.8) kg/m2, respectively, showing statistical difference. R.E.N.A.L scoring was not markedly different (8.8 ± 1.5 vs. 8.9 ± 1.3). Operative time (144.7 ± 38.5 min vs. 122.5 ± 47.3 min), warm ischemia time (22.3 ± 4.6 min vs. 27.2 ± 5.5 min), estimated blood loss (50.3 ± 26.6 mL vs. 43.6 ± 37.5 mL), and length of stay (7.3 ± 1.9 d vs. 7.8 ± 1.8 d) were not statistically different. No Clavien Grade III+ complications were recorded in both groups.
Conclusions:
The ASMD technique may effectively expand retroperitoneal space and improve surgical exposure during retroperitoneal robotic partial nephrectomy for complex renal tumor, and may also reduce warm ischemia time.
Funding:
This study is supported by the 2022 National Natural Science Fund (Youth Fund, No. 82203138, YC), and the Shanghai “Rising Stars of Medical Talents” Youth Development Program (SHWSRS(2025)_071, YC).
Conflicts of Interest:
The authors declare no conflicts of interest regarding this study.
Author Disclosure Statement:
The authors have received and archived patient consent for video recording/publication in advance of video recording of procedure.
Runtime of video: 2 mins 51 secs.
Get full access to this article
View all access options for this article.
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.