
Abstract
Introduction:
In the past few decades, urologists have advanced minimally invasive surgery, implementing endourology, percutaneous renal surgery, laser technologies, and more recently robot-assisted surgery. 1 Robot-assisted laparoscopic partial nephrectomy (RPN) is the preferred option to treat small renal masses when technically feasible. However, this procedure is subject to surgeon's expertise and skills. The learning curve has been pointed out as a limitation for a high diffusion of this surgical technique. 2 Therefore, efforts should be made to simplify this technique for wider dissemination. This procedure gets even more challenging when performed on a kidney graft, because of the difficulty of dissection of transplant vessels to allow clamping of the artery, and risk of thrombosis of the iliac artery at clamping. At the same time, interventional radiology has progressed and has become accessible to urologists in the fields of oncology, andrology, and functional urology. We reported the first RPN without pedicular dissection using reversible endovascular clamping of segmental branch of the renal artery using a balloon catheter on a kidney graft.
Materials and Methods:
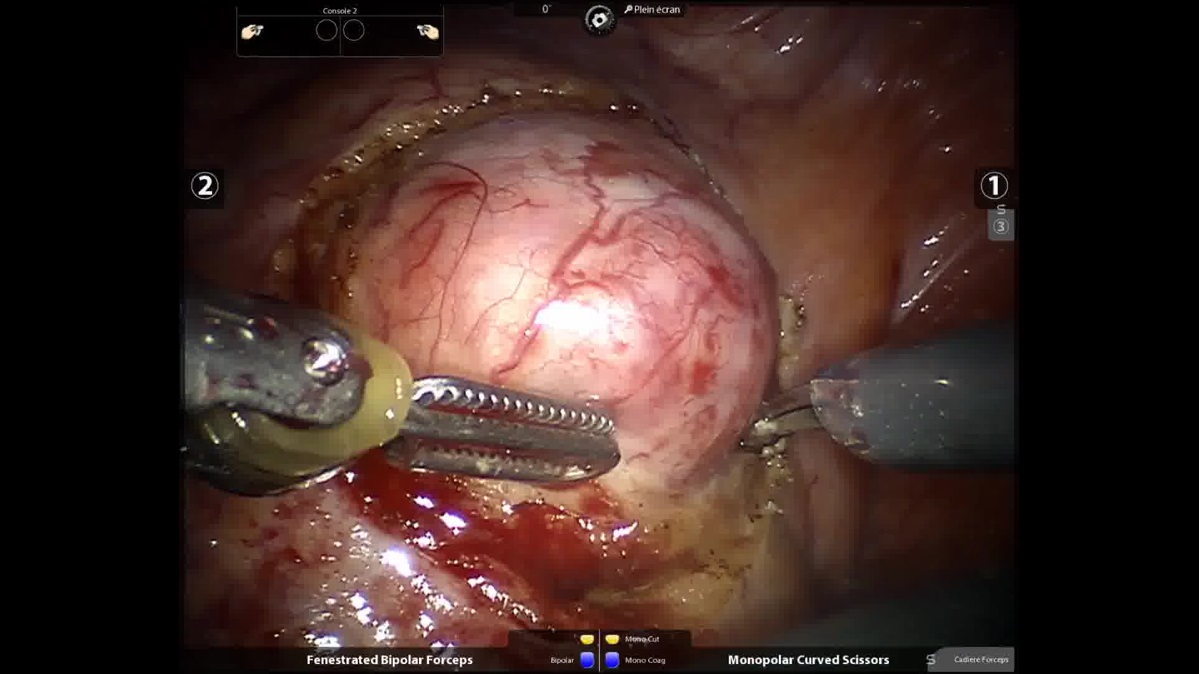
A 69-year-old man with history of multiple cardiovascular risks and a diabetic nephropathy end-stage kidney failure underwent kidney transplantation in 2012. During the kidney transplant follow-up, a 2.3 × 2.6 cm solitary tumor was discovered on ultrasonography, later confirmed by CT scan. Preoperative serum creatinine was 140 μmol/L with an estimated glomerular filtration rate (eGFR) of 50 mL/min per 1.73 m2. Decision was made to proceed with RPN after the multidisciplinary consultation meeting. We performed RPN through the transperitoneal approach with selective endovascular balloon clamping. First, the patient underwent an endovascular angiography under local anesthesia to identify the segmental branch vascularizing the tumor. A Pacific Plus Percutaneous Transluminal Angioplasty balloon catheter Other The Wire 0.018, 4 mm in diameter and 20 mm long at a pressure of 16 atm, was used to temporarily occlude the selective renal artery branch during tumor excision. The total time of the angiography procedure was 10 minutes. The balloon was tested to see if a complete occlusion of the segmentary artery was performed during inflation. After the correction position of the occlusive balloon was found, it was deflated, then secured by being strapped to the patient's right leg, allowing the transfer from the interventional radiology (IR) to the operative room (OR) without any misplacement complications. Second, the patient was transferred to the main operating theater where surgery was performed under general anesthesia. We used a 4-arm Si HD da Vinci robot (Intuitive Surgical, Inc., Sunnyvale, CA) with the patient in a supine position and port placement similar to a pelvic robotic surgery (camera trocar placed at the umbilic, two robotic trocars on the same horizontal line as the camera trocar on the right side of the patient, one robotic arm on the same horizontal line at the left of camera trocar, and two assistant trocars on the left side, one placed on the same horizontal line as the robotic trocars, close to anterior iliac spine, and one between camera trocar and left robotic arm). The following procedural steps were performed sequentially: a transperitoneal approach with a 4-arm trocar placement, a perioperative ultrasonographic border demarcation of the tumor, selective endovascular control of the renal artery, tumor excision, and renal reconstruction using the sliding-clip renorrhaphy technique. The occlusive balloon was inflated during surgery, after demarcation of the tumor, when the surgeon was ready for tumor excision.
Results:
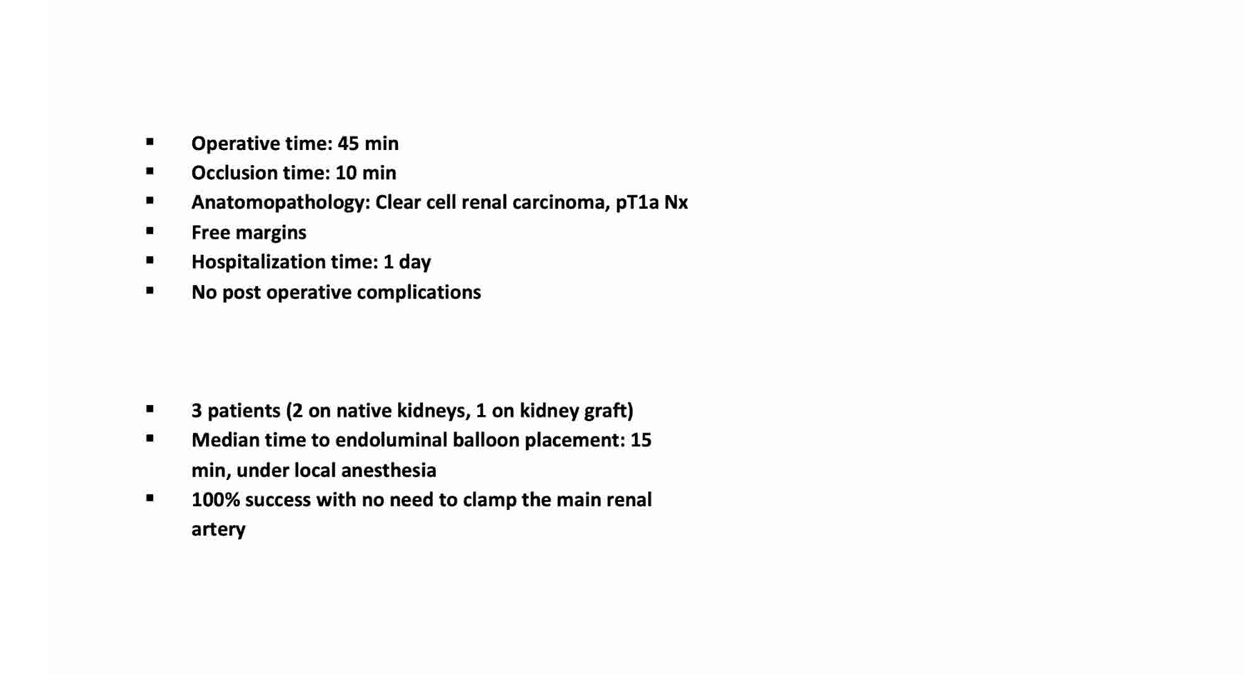
The total operating time was 45 minutes with an occlusion ischemia time of 10 minutes. Estimated blood loss was ∼100 mL. No perioperative complications occurred. The patient was discharged from the hospital 1 day after the procedure without any complication. Postoperative serum creatinine levels were 158 μmol/L with an eGFR of 44 mL/min per 1.73 m2. The pathologic analysis revealed a 3 cm clear cell renal cell carcinoma with negative margin (pT1a). Two additional cases were performed using this technique, with similar results (two on native kidneys, one on kidney graft).
Discussion:
For clinically localized renal masses, European 3 and North American 4 guidelines recommend preference for partial nephrectomy (PN) whenever technically and oncologically safe and feasible. Therefore, an optimal PN should maximize functional and oncologic outcomes, whereas minimizing procedure-related complications. Clampless laparoscopic PN without pedicular dissection after previous tumoral embolization is a technically safe and oncologically efficient, minimally invasive alternative for the management of localized renal tumors. 5 Minimally ischemic and off-clamp PN are established procedures that may be particularly applicable for patients with decreased baseline renal function. 6 In a previous report, we reported our experience on RPN with endovascular control of the main renal artery using a balloon catheter for an allograft kidney tumor. 7 To our knowledge, this is the first RPN without pedicular dissection and super-selective clamp using an endovascular balloon catheter for a solitary kidney tumor on a kidney graft. The procedure seems to be feasible and safe. There are some limitations to this technique, as the balloon could move during the transfer between IR and OR, and, therefore, not to completely occlude the segmentary arteries selected for tumor vascularization. It would also be interesting to compare blood loss and renal function between occlusion of the main renal artery and a selective clamping of a segmentary artery. A larger cohort is necessary to confirm the safety of this technique on a bigger scale. In the next few years, interventional radiology may play a larger role in the care of urologic patients. To maintain our leadership in the management of urologic conditions, we will require the rapid learning, adoption, and promotion of these innovations on urologic educational programs. Interventional radiology has progressed and become available to urologists in the fields of oncology, andrology, and functional urology. Most interventional radiologists have a working relationship with their local urology department. Building on an existing relationship, development of training program for urologist will be beneficial to both specialties and can help mitigate any perceived threat. Therefore, the real challenges in the future will be to reinforce the identity of our discipline and train competent individuals on urologic imaging techniques. This goal can be reached only by realizing a targeted educational strategy focused on undergraduate, postgraduate, and fellowship programs for urologists.
Conclusion:
Robotic PN with reversible endovascular balloon occlusion on a kidney graft seems like a feasible and safe technique for kidneys tumors on grafts. More patients should be included to have a learning curve analysis on this technique.
No competing financial interests exist.
Authors have received and archived patient consent for video recording/publication in advance of video recording of procedure
.
Runtime of video: 07 mins 47 secs
Keywords
Get full access to this article
View all access options for this article.