
Abstract
Introduction:
Renal artery pseudoaneurysm (RAP) and urinary fistula (UF) after partial nephrectomy (PN) have been the major complications that urologists should overcome. The incidence of symptomatic RAP and UF after PN has been reported to be ∼1%–2% and 1%, respectively. 1 –3 The mechanism of RAP formation after surgery has not been fully elucidated. However, some investigators have suggested possible causes of RAP, including incomplete hemostasis of the resection surface and laceration of arterioles caused by suturing to the renal sinus or parenchyma. 4,5 Kondo et al. reported that early unclamping might reduce the risk of RAP. 5 In contrast, the cause of UF is thought to be incomplete closure of the renal collecting system and isolated calix because of deep inner suture. 6 Kundu et al. described that tumor size, estimated blood loss, and ischemia time were all associated with an increased risk of UF formation. 7
Methods:
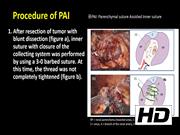
The parenchymal suture-assisted inner suture (PAI) method is performed as follows: (1) Blunt dissection and small vessels clipping (or sealing) with ischemia were performed in the resection phase. (2) Inner suture with closure of the collecting system was performed by using a 3-0 verbed suture. At that time, the thread was not completely tightened. (3) Only one stitch of parenchymal suture was made and tightened. (4) The thread of the inner suture was completely tightened. (5) When the thread of the inner suture was difficult to tighten, an additional stitch of parenchymal suture was performed. (6) Renal arteries were unclamped after the inner suture was completely tightened. (7) After hemostasis of the arterial bleeding on the resected surface by additional suturing or electrocoagulation, the parenchymal suture was completed. We performed a retrospective review of patients at our institution undergoing PAI method. Patient demographics, operative outcomes, and postoperative renal function are presented.
Results:
We have performed >70 robot-assisted partial nephrectomies (RAPNs) using this method since we started using it in October 2018 (∼30% of all RAPNs in our institutions). We summarize 40 cases of RAPN with the PAI method that were performed between October 2018 and March 2020. Only one tissue fracture occurred during tightening of the inner suture thread (0.0025 time per case). Furthermore, only two cases of mild hematuria occurred, which was improved conservatively, and no case of RAP or UF was found. Postoperative renal function deteriorated slightly. This method seemed to enable a reliable but shallow inner suture. Furthermore, the presence or absence of arterial bleeding on the resected surface can be confirmed in the same way as with the normal early unclamping technique, as only one (or two) stitch of parenchymal suture is placed. This might also contribute to decrease in the incidence of RAP.
Conclusion:
The PAI method may be effective support for achieving a reliable inner suture in RAPN. It may be useful when tissue tearing is likely during inner suture, especially in the case in which the resected surface is widely opened.
All the authors have nothing to disclose to any commercial associations during the past 3 years that might create a conflict of interest in connection with the video.
For the patients: We have received and archived patient consent for video recording/publication in advance of video recording of procedure.
Runtime of video: 9 mins 31 secs


Get full access to this article
View all access options for this article.