
Abstract
Introduction:
In duplex anomalies, the upper pole system is often associated with obstruction at the ureterovesical junction (UVJ) associated with an ureterocele or intrinsic UVJ obstruction. 1 Given the likelihood of a poor functioning upper moiety, varying surgical options have been described including upper pole heminephrectomy, distal ureteroureterostomy (U-U), ureteral reimplantation, and simple ligation of the upper pole ureter. The factors that aid this decision process include a combination of upper pole function, ureteral size disparity, presence of reflux, and surgeon and family preferences. U-U has been shown to be a safe and effective technique for reconstruction irrespective of ureteral size or upper pole function. 2 –5 For the past decade, with the introduction of the da Vinci Surgical System, there has been a gradual increase in performing complex reconstructive procedures using the da Vinci System. 6,7 A technique for robot-assisted laparoscopic U-U has been previously described for the pediatric population with ectopic insertion of the upper pole ureter. 8,9 Often there is a considerable disparity in the diameters of the upper and lower pole ureters and a U-U can potentially be obstructive when anastomosing a very dilated upper moiety ureter to a normal nonrefluxing lower moiety ureter. Our video shows a robot-assisted distal U-U for upper pole UVJ obstruction wherein a tapering of the obstructed upper moiety ureter was performed to aid the distal U-U.
Materials and Methods:
Three symptomatic patients with duplex collecting system and UVJ obstruction of the upper pole moiety secondary to an ectopic upper pole insertion constituted this series. Patients ranged between 5 and 7 years, with a minimally functioning upper pole moiety with grade 4 hydronephrosis and hydroureter and no reflux to either moiety. After discussing the pros and cons of each approach and factoring in possible implications of retaining a poorly functioning upper pole, the parents in each case decided to proceed with a distal robot-assisted U-U.
Results:
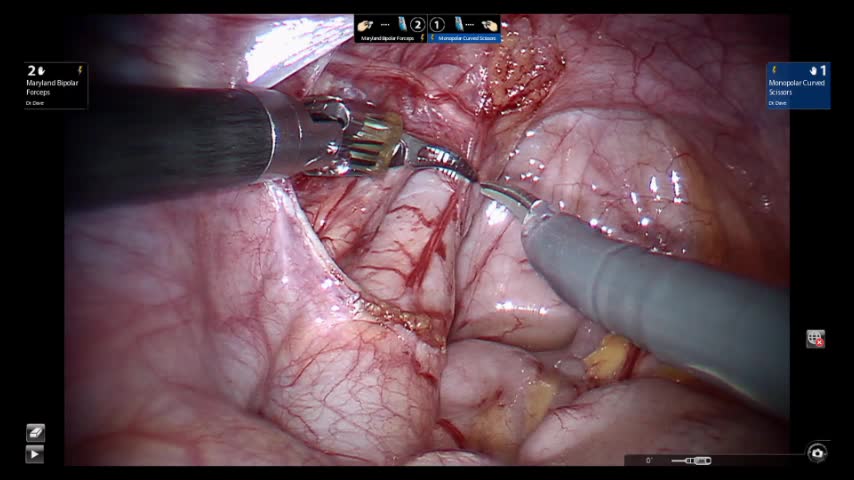
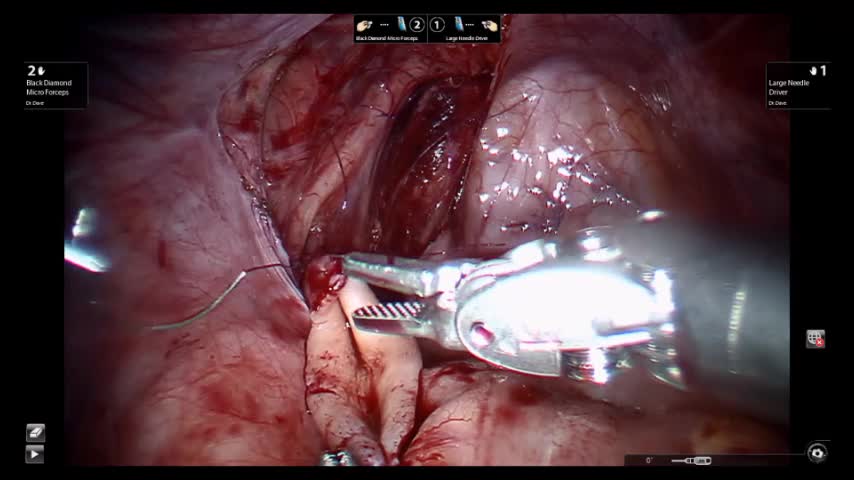
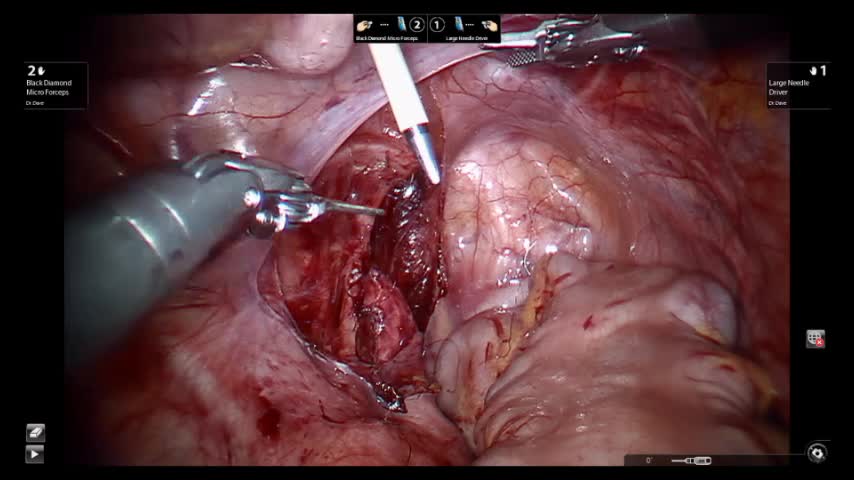
All patients underwent a robot-assisted distal end-to-side upper pole to lower pole U-U with tapering of the upper pole ureter while leaving the lower pole ureter in situ. A three-port technique was performed, with use of an assistant port to provide retraction and allow the tapering. The video describes the relevant technical aspects of the procedure. A Double-J stent was placed across the anastomosis into the bladder in an antegrade manner and across the anastomosis into the upper pole ureter. A Foley catheter was left in situ for 24 hours. Stent was removed 4 to 6 weeks after the procedure. Follow-up at 4 months' poststent removal showed significant decrease of the upper moiety hydronephrosis and resolution of the hydroureter.
Conclusion:
We demonstrate a technique for robot-assisted distal U-U with tapering of the obstructed upper moiety ureter for duplex systems with an obstructed upper pole moiety. This is a viable and effective minimally invasive option for surgical correction of duplex systems with upper pole UVJ obstruction.
Patient Consent Statement:
The authors have received and archived patient consent for video recording/publication in advance of video recording of the procedure.
The authors do not have any conflicts of interest in connection with the submitted article or commercial interests. No competing financial interests exist.
Runtime of video: 7 mins 54 secs
A video abstract of one of the cases was previously published at World Congress of Endourology 2017. Ni L, Dave S. Robotic assisted extravesical ureteric reimplantation with psoas hitch for primary obstructed megaureter. World Congress of Endourology 2017, Vancouver, CA, September 2017.
Get full access to this article
View all access options for this article.