
Abstract
Introduction:
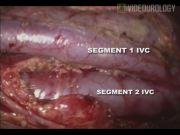
Retrocaval ureter, also called circumcaval ureter, is a rare congenital anomaly with an incidence of 1 in 1100. The ureter becomes entrapped behind the inferior vena cava (IVC) because of the abnormal persistence of the right subcardinal vein as opposed to the supracardinal vein. This forces the right ureter to encircle the inferior vena cava from behind. The retrocaval ureter has been classified based on intravenous urography (IVU) or retrograde pyelographic (RGP) findings. Bateson and Atkinson classified a ureter with a fish-hook appearance as type I. The ureter typically overlies or is medial to the lower lumbar vertebral processes and eventually crosses anterior to the iliac vessels, where it then assumes a normal distal course in this setting. A less-angulated sickle-shaped ureteral deformity is classified as type II. 1 Laparoscopic reconstruction of retrocaval ureter is gaining acceptance in view of less operative morbidity compared to an open approach. 2 We present a video demonstration of reconstruction of the retrocaval ureter in different scenarios. Port positions are depicted in the illustration. After achieving the pneumoperitoneum, the ascending colon was mobilized, and the ureter and vena cava were identified. Ureter mobilized on either side of the vena cava and disconnected lateral to the vena cava. The distal and proximal ends were spatulated after excising the unhealthy segment. Tension-free ureteroureterostomy was carried out using 4-0 polyglactin suture. Interrupted sutures were placed, and the Double-J stent was placed in a retrograde fashion. The technique is similar for type 1 and type 2 variants. We encountered with the rare variant of the retrocaval ureter in which ureter was entrapped between two segments of the vena cava. The ureter was passing beneath the lateral segment of the incompletely duplicated vena cava. In this scenario, instead of doing ureteroureterostomy, the lateral segment of vena cava that was causing ureteral obstruction was clipped and disconnected. This maneuver was sufficient to relieve ureteral obstruction. Hemostasis achieved, and the drain was placed.
Material and Methods:
All patients who underwent laparoscopic reconstruction for the retrocaval ureter at our center were analyzed. A detailed evaluation (IVU, RGP) was carried out to reach diagnosis. Laparoscopic reconstruction of the retrocaval ureter through the transperitoneal route was contemplated. The operative and postoperative details were recorded.
Results and Conclusion:
Totally, eight patients underwent laparoscopic reconstruction of the retrocaval ureter at our center from 2003 to 2011. Type 1 and type 2 were present in five and two patients, respectively; one patient had a retrocaval ureter with a twin-segment vena cava. M:F was 6:2; the mean age was 26.5 years; the mean operative time was 110 minutes; the mean blood loss was 100 mL; the mean requirement of analgesic was 105 mg (tramadol hydrochloride); the mean duration of hospital stay was 45 hours; and the mean duration of follow-up was 32 months. Till last follow-up, all patients were asymptomatic, and follow-up imaging showed satisfactory drainage and function of the affected renal unit. Laparoscopic reconstruction is feasible in all varieties of the retrocaval ureter. In a rare variety in which ureter becomes entrapped between the two segments of IVC, clipping and disconnecting the obstructing segment of vena cava may be sufficient to relieve the obstruction. A minimally invasive approach offers less morbidity with a good outcome.
No competing financial interests exist.
Runtime of video: 6 mins 50 secs


Keywords
Get full access to this article
View all access options for this article.