
Abstract
Introduction:
Surgical technical error is a modifiable cause of positive surgical margins (PSMs) for robot-assisted laparoscopic prostatectomy (RALP). Retrospective intraoperative video review has the potential to evaluate technique. Gross pathology can be used to identify PSMs, which can then be correlated with the retrospective video review to identify where in the operation the positive margin took place. Technical errors, however, have not been well published. We present a 6:48 minute video comparing whole-mount pathology to surgical technique for RALP with a specific focus of evaluating the technical error of each operation at the prostate base.
Materials and Methods:
We reviewed the patients with PSMs who had video recordings for a single surgeon at our institution (P.M.) at our institution from 2008–2011.
Results:
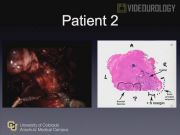
We identified two patients with a PSM at the prostate base after RALP at our institution. Both operations utilized the posterior approach for clinical T2 disease. The whole-mount pathology was reviewed and then compared to the dissection of the prostate base. In both videos, we were able to identify the disruption of the prostate due to technical error. The first patient had a PSM at the left posterior base that occurred during dissection of the posterior lateral pedicle. Upon review, we believe that this could have been avoided by opening Denonvillier's fascia before dissecting the posterior lateral pedicles. The second patient had a positive margin was at the right posterior base that occurred at the junction of the seminal vesicle and prostate. This area was exposed during division of the bladder neck. Upon review, we believe that this could have been avoided by extending dissection along the lateral seminal vesicle until the prostate base was established.
Conclusions:
Video review has the potential to standardize training, improve surgical technique, and ultimately reduce technical error. Touijer et al evaluated positive margins in 12 cases and identified that technical error resulted in 8 positive margins. As a result, their group eliminated blunt teasing of the neurovascular bundles and instead controlled the capsular vessels by dividing them after the dissection plane was defined as well as control the prostatic pedicle higher on the prostate base to better delineate the limits of the neurovascular bundles and prostate. This resulted in a lower PSM rate in the next 90 patients.1 Open prostatectomy has also been evaluated with retrospective video. Walsh et al. retrospectively blinded reviewers to 62 videos and was able to identify four key steps that correlated with the recovery of sexual function. Ultimately, this exercise resulted in modification of surgical technique used by their institution.2 Simulation and video have already been integrated in many teaching programs and has been found to be successful.3,4 At our institution, we hope to improve upon simulation and use retrospective evaluation of robotic prostatectomy to improve resident teaching and outcome. For these two reviewed cases, surgeon technical error resulted in PSMs. A better understanding of previous errors will hopefully decrease future PSMs at this critical step.
The authors have no significant financial interest or other relationship with the manufacturers of any products or providers of any service mentioned in this article.
Runtime of video: 6 mins 48 secs


Keywords
Get full access to this article
View all access options for this article.