
Abstract
Introduction:
Percutaneous entry is the initial and most important part of percutaneous nephrolithotomy. Needle puncture directly into the fornix of a calix is the safest route of percutaneous entry into the renal collecting system. The ultrasonographic approach has the advantages of minimizing radiation exposure and allowing imaging of intervening structures between skin and kidney. The ultrasonic depiction of the dilated calices is easily obtained. However, when the pelvicaliceal system is not dilated, localization and puncture of the specific calix may require special expertise. Improper site selection can lead to difficulty performing the procedure at best and devastating complications at worst. The present study investigated the usefulness and safety of contrast-enhanced ultrasonography (CE-US) using Sonazoid® (Daiichi-Sankyo) in the needle puncture to the renal calix. Sonazoid consists of an aqueous dispersion of lipid-stabilized perfluorobutane-filled gas microbubbles, and it can show enhanced images without destroying the contrast media, which enables a continuous observation of the target organs.
Materials and Methods:
All study protocols for this clinical investigation were approved by the ethics review board of Kurashiki Medical Center, and fully informed consent about the needle puncture to the renal calix using CE-US with intracaliceal and intravenous injection of Sonazoid was obtained from each patient before enrolment. The study comprised two patients (one antegrade and one retrograde approach). The contrast agent Sonazoid was used intravenously at a dose of 0.0015 mL/kg by a manual bolus injection after a flush with 3 mL normal saline, and simultaneously injected intracaliceally at a dose of 0.1 mL diluted with 100 mL normal saline through the instrument port of flexible ureteroscope. This study used TOSHIBA Aplio MX ultrasonic diagnostic equipment (TOSHIBA Medical Systems) with a 3.5-MHz microconvex transducer. Acoustic power of CE-US was set to the default setting with a mechanical index of 0.2; the dynamic range was fixed at 45–60 dB. A single focus point was set at a depth 6–10 cm. This machine sets out dual vision with real-time monitor mode (Sonazoid-mode, B-mode) simultaneously.
Results:
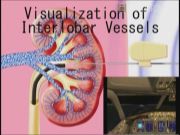
General anesthesia was administered with monitoring by blood pressure, heart rate, and saturation pulse oximetry. Immediately after the intracaliceal injection of Sonazoid, enhancement in the desired calix and flow down to the ureter was observed. Hybrid imaging (radiopaque and echopaque) was gained. Approach flash lighting of interlobar Sonazoid was attained 5–90 min after intravenous Sonazoid injection. The needle was safely punctured between interlobar vessels indicating as Sonazoid stream on the Sonazoid-mode, into the desired calix (antegrade or retrograde approach with Lawson's wire; COOK Medical) in the single session.
Conclusions:
There is no adverse effect of Sonazoid administration or postoperative complications (fever or blood loss necessitating blood transfusion) of caliceal needle puncture after percutaneous nephrolithotomy. A new needle puncture technique to the renal calix with intracaliceal and intravenous injection of Sonazoid is safe and effective even when the pelvicaliceal system is not dilated.
No competing financial interests exist.
Runtime of video: 7 min

Keywords
Get full access to this article
View all access options for this article.