
Abstract
Introduction:
The aim of this video is to describe four alternatives for early ligature of the renal artery during transperitoneal laparoscopic radical nephrectomy.
Materials and Methods:
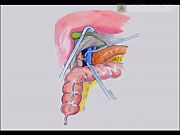
(i) Standard early right renal artery ligature: Patient is placed in the extended lateral decubitus position. Four 12-mm ports are used. The first is placed just to the right of or inside the umbilicus, the second at the midclavicular line 2 cm below the costal margin, the third on the anterior axillary line 3 cm below the umbilicus, and the fourth along the midaxillary line. The visceral posterior peritoneum is incised in the mesocolic space along the anterior vena cava wall. The duodenum is reflected medially. The right renal vein is identified and the medial margin of Gerota's fascia is dissected from the lateral wall of the vena cava. The right renal artery is identified, isolated, and closed with a Hem-o-Lok® clip. (ii) Early right renal artery ligature in the interaortocaval space: The patient and ports are positioned as above. The duodenum is completely kocherized to allow identification and exposure of the biliary ducts. The vena cava and both the left and the right renal veins are identified. The interaortocaval space is dissected with scissors. The left renal vein is lifted upward with forceps, and the right renal artery is isolated with a dissector and then clipped. (iii) Standard early left renal artery ligature: The patient is placed in the extended lateral decubitus position. Three 12-mm ports are used. The first is placed just to the left of or inside the umbilicus, the second at the midclavicular line 2 cm below the costal margin, and the third on the anterior axillary line 3 cm below the umbilicus. The line of Toldt is incised; pancreas, spleen, and colon are mobilized medially. Gerota's fascia is exposed and incised medially to expose the left renal vein, which is isolated. Gerota's fascia is incised and dissected from the lateral wall of the aorta to identify the left renal artery, which is isolated and ligated. (iv) Early left renal artery ligature at level of the ligament of Treitz: The patient and ports are positioned as above. The fourth part of the duodenum and the inferior mesenteric vein are identified. The ligament of Treitz and posterior peritoneum are incised along the inferior mesenteric vein. The left renal vein is retracted with forceps where it crosses over the aorta, the anterolateral surface of the aorta is identified, the aortic wall is freed of lymphatic tissue, and then renal artery is identified and secured with a suture ligature or Hem-o-lok clips. This approach can be helpful in case of large hilar tumors that could complicate the standard control of renal artery.
Results and Conclusions:
In our experience, the proposed techniques were equally safe. 1 We cannot draw definitive conclusions about the oncological efficacy of early renal artery ligature with direct access in comparison with standard technique, but we believe that this technique adheres most strongly to the classical principles of radical nephrectomy. 1 –4
No competing financial interests exist
.
Runtime of video: 8 min 54 sec


Get full access to this article
View all access options for this article.