
Abstract
Introduction:
The main extrathyroidal manifestation of Graves’ disease (GD) is Thyroid Eye Disease (TED). 1 Although it can be considered a rare condition (0.54–3.3 cases/100.000 person/year), TED has a striking impact on patient’s quality of life. 2 Treatment depends on inflammation, assessed by Clinical Activity Score (CAS) and disease severity. If active, mild TED should be managed with local treatment, selenium (if deficient), and risk factors control. Intravenous (IV) glucocorticoid is the first-line therapy for active, moderate-to-severe TED. 2 As second-line options, we have several medications depending on the remaining treatment goal (e.g., teprotumumab, tocilizumab, rituximab, azathioprine, cyclosporin, oral prednisone, a second course of IV glucocorticoid or orbital radiotherapy). Sight-threatening TED should be managed with high-dose IV glucocorticoids (500 mg to 1 g daily for 3 consecutive days) and referred to urgent orbital decompression if unresponsive to medical treatment. 2 Here, we present a case of a patient with sight-threatening TED, unresponsive to clinical treatment, who was referred to urgent orbital decompression by the ear, nose, and throat (ENT) team.3,4
Case Description:
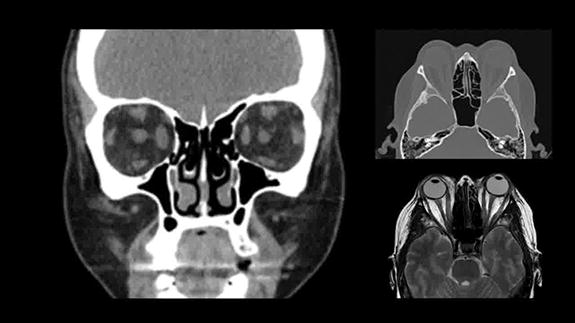
A 47-year-old female patient with a 10-month history of thyrotoxicosis, diagnosed with Graves’ disease and treated with oral methimazole and beta-blockers, developed TED 3 months before admission. Visual acuity was progressively lower when she presented to the Ophthalmology ER with sight-threatening orbitopathy (CAS = 6 and fundoscopy showing optic nerve compression on the left eye). Treatment with IV methylprednisolone 1 g for 3 days was initially chosen. However, there was no response. Thus, one week later, she was referred to orbital decompression surgery through an endonasal approach while on weekly IV glucocorticoids (methylprednisolone 500 mg) and oral cyclosporine 100 mg bid.
Surgical Technique:
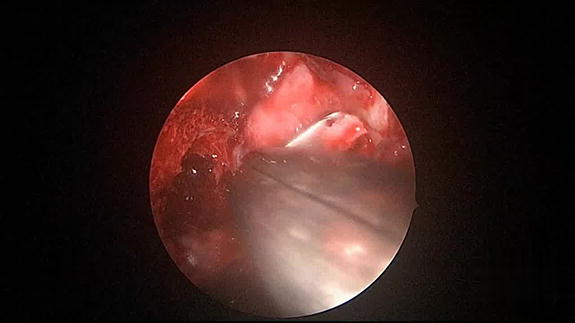
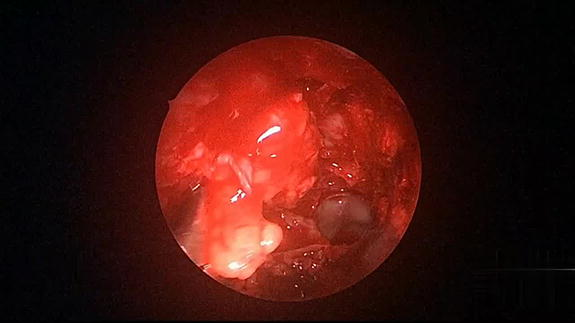
Under general anesthesia, the patient was positioned supine on the operating table, with the head slightly elevated (about 15°–30°) to reduce venous pressure and minimize bleeding. Local anesthetic with lidocaine with epinephrine was injected into the nasal mucosa and around the nasal turbinates to reduce bleeding and provide additional anesthesia. A spray nasal decongestant was applied to the nasal cavity to shrink the nasal mucosa and reduce bleeding. Then the nasal cavity was carefully inspected to clear any mucus or crusts. With the aid of a 4 mm zero-degree endoscope, we used a microdebrider to provide access through the facial sinuses allowing a posterior ethmoidectomy. After broad exposure of the entire orbital cone, the papyraceous lamina was removed, exposing the periorbita, which was opened to access the fat tissue on the middle meatus region. Then, the lower medial orbital strut was removed in its posterior third, along with the bone floor of the nasal cavity and the lateral limit of the infraorbital nerve, decompressing the cavity. The most posterior part of the decompression was the annulus of Zinn, therefore it was not necessary to open the lateral wall of the sphenoid sinus.
Results:
Before surgery, the patient had a CAS of 6, could only count fingers from 1 m on the right eye (RE), and had light perception on the left eye (LE). Immediately after the procedure, visual acuity measured by the Snellen Scale was 20/25 on the RE and 20/160 on the LE. After one week of in-hospital admission, she presented a CAS of 3. Her visual acuity was 20/25 on the RE and 20/40 on the LE, and she was discharged with an important functional improvement, without diplopia. There was no need for prism glasses after the procedure.
Conclusions:
This video showcases the transnasal orbital decompression technique for urgent orbital decompression in a case of severe sight-threatening TED unresponsive to clinical treatment. 3
Author Disclosure Statement:
We report no commercial associations that would create a conflict of interest with this video. The patient signed a consent form to allow the publication of the case report.
Runtime of video: 2 mins 28 secs.
Get full access to this article
View all access options for this article.