
Abstract
Introduction:
Long-term management of intermediate- and high-risk differentiated thyroid cancer (DTC) involves thyrotropin (TSH) suppression with thyroid hormone to prevent potential stimulation of TSH receptors on DTC cells, leading to tumor growth. However, the current guidelines recommending TSH suppression are based on low-to-moderate quality evidence.
Materials and Methods:
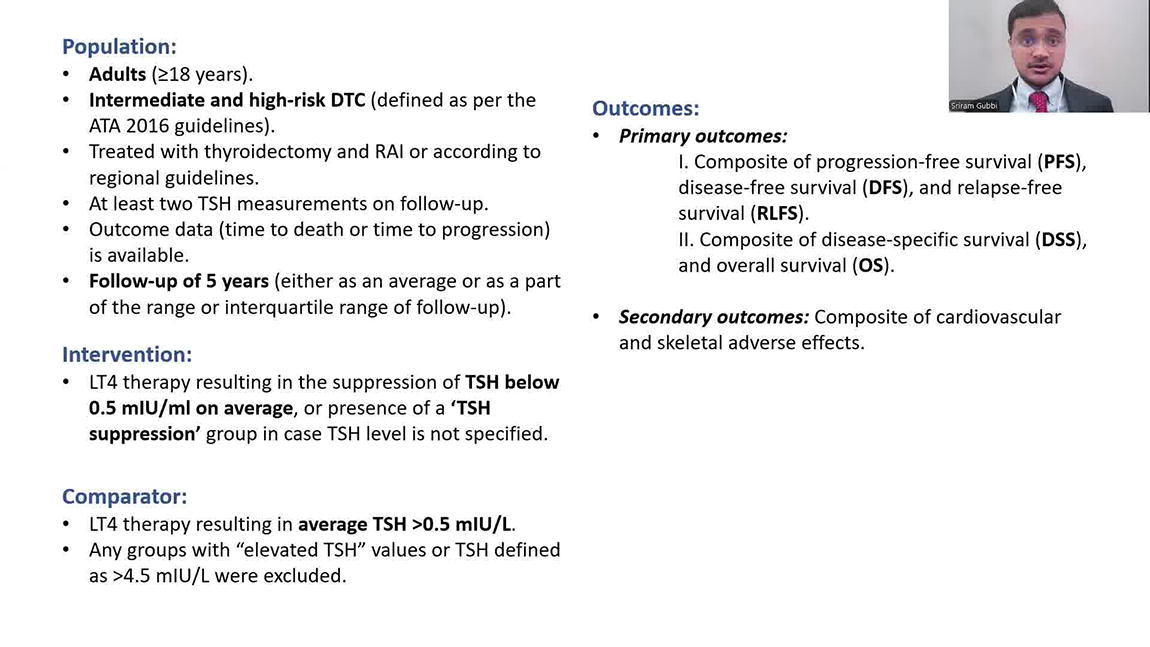
We performed a systematic review and meta-analysis of studies evaluating the role of TSH suppression in intermediate- and high-risk DTC patients (≥18 years) treated as per regional guideline-based therapy with a follow-up duration of 5 years (PROSPERO #252396). TSH suppression was defined as <0.5 mIU/L or “below normal reference range” if a specific value was not provided. Primary outcome measures included I. A composite of progression-free survival (PFS), disease-free survival (DFS), and relapse-free survival (RLFS), and II. A composite of disease-specific survival (DSS), and overall survival (OS). Secondary outcome included a composite of cardiac or skeletal adverse events. Study quality was assessed using the NHLBI study quality assessment tool, with studies being rated as “good,” “fair,” or “poor,” based on their risks for bias. All outcomes and comparisons were represented as TSH suppression versus TSH non-suppression (defined as a TSH value of 0.5–2 mIU/L or >2 mIU/L; with TSH values of >4.5 mIU/L being excluded). Randomized controlled trials (RCTs), cohort studies, and case-control studies were included for analysis. Pooled hazard ratio (HR) and 95% confidence interval (CI) were calculated using random-effects model, and heterogeneity among the studies was quantified by using the I2-statistic.
Results:
A total of 8043 records were identified from the database search, and 1674 duplicate records were excluded. Abstract screening was performed on 6369 studies. After the exclusion of irrelevant studies followed by full-text screening, nine studies were selected for the final meta-analysis. Based on seven studies (3591 patients), the composite outcome of PFS, DFS, and RLFS was not significantly different between TSH suppression and non-suppression groups (HR: 0.75; 95% CI: 0.48–1.17; I2 = 76%). Similarly, a DSS and OS composite outcome assessment based on four studies (3616 patients) did not favor TSH suppression (HR: 0.69; 95% CI: 0.31–1.52; I2 = 88%). When only the “good” quality studies were analyzed after excluding studies of “fair,” and “poor” quality, the primary outcomes were still not significantly different between the TSH suppression and non-suppression cohorts. The secondary outcome, obtained from two studies (1294 patients), was significantly higher in the TSH-suppressed groups (HR: 1.82; 95% CI: 1.30–2.55; I2 = 0%). Significant study heterogeneity was noted for primary outcomes, while low heterogeneity was noted for the secondary outcome.
Conclusions:
TSH suppression in intermediate- and high-risk DTC may not improve survival outcomes but may increase the risk of secondary complications. However, the presence of heterogeneity among the included studies, and the limited number of good quality studies warrant cautious interpretation of our results. Future, large-scale RCTs could potentially clarify the role of TSH suppression in the management of intermediate- and high-risk DTC.
Author disclosure statement:
All authors have no conflicts of interest to declare.
Funding:
This study was supported by the intramural program of the National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health (Grant No. 1ZIADK047053-17).
This video is a discussion of The Effect of Thyrotropin Suppression on Survival Outcomes in Patients with Differentiated Thyroid Cancer: A Systematic Review and Meta-Analysis, which was previously accepted at the Thyroid Journal. It can be found at https://www.liebertpub.com/doi/10.1089/thy.2023.0711.
Runtime of video: 10 mins 47 secs.
Get full access to this article
View all access options for this article.