
Abstract
Abstract
Introduction:
Papillary thyroid carcinoma (PTC) comprises over 80% of thyroid carcinomas. Generally, PTC has an excellent prognosis with a 10-year survival rate of up to 95%. 1 According to the American Thyroid Association guidelines 2015, surgery is the primary mode of therapy which can be followed by radioiodine remnant ablation after risk stratification. 2 However, up to 55% of cases can recur, with more than 90% of these recurrences being in the neck and cervical lymph nodes. 3 The recent consensus guidelines (2022) published by the American Head and Neck Society discuss the increasing trend and the promising role of radiofrequency ablation (RFA) in treating recurrent thyroid cancer with either curative or palliative treatment intent. 4 Multiple studies have shown this technique to be safe with rare complications.5,6 Emerging longer-term data have shown complete tumor disappearance by the final evaluation of up to 91.3% with RFA for locally recurrent PTC and 72% for recurrences in the central compartment.7,8 Here, we present a case of a patient with PTC who developed a local recurrence treated with RFA.
Materials and Methods:
Case Description. Our patient is a 38-year-old physician with a classical left-sided intra-thyroidal PTC sized at 1.2 cm which was removed via near-total thyroidectomy in 2013. In 2014, left central and lateral neck dissection was done for a recurrence in left level III and IV cervical lymph nodes, which revealed malignancy in 2 out of 10 nodes. Remnant ablation was done with I-131. In 2022, a new left central/thyroid bed node measuring 1.5 × 0.8 × 1.1 cm was discovered. The patient declined left neck dissection and elected for RFA treatment. RFA was decided upon as ≤3 nodes were involved and the tumor size was <1.5 cm. 9
Technique.
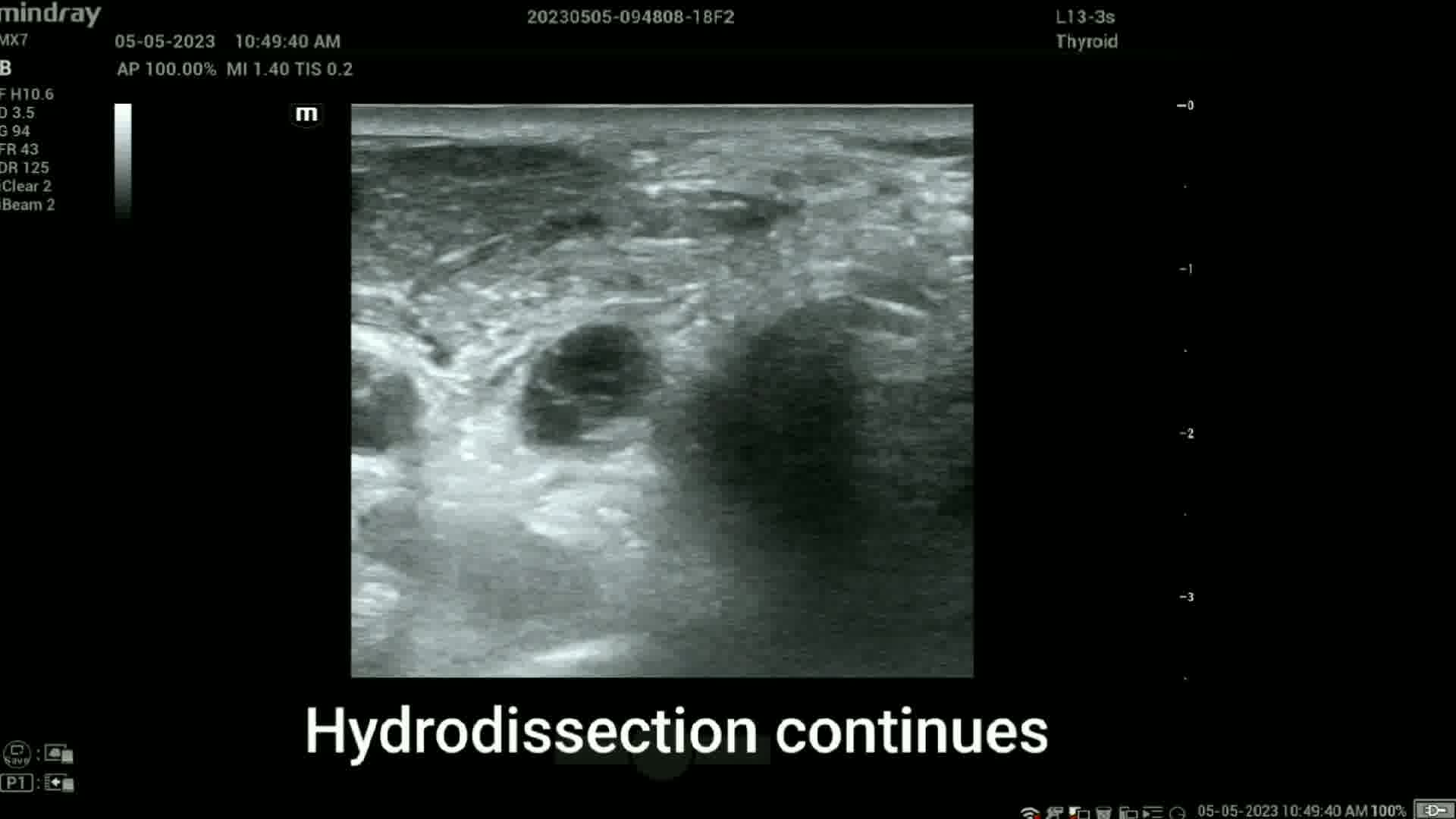
RFA was performed with an RFA system (Cambridge Interventional) using an 18-gauge internally cooled electrode with a 0.5 cm active tip powered at 35 W. The RFA procedure was started with perilesional and subcutaneous infiltration of 3–5 mL 2% lidocaine under ultrasound guidance. For hydrodissection, 25 mL of cold (0°C–4°C) dextose 5% water (D5W) was injected behind the lesion with a 25-gauge needle under ultrasound guidance, with the needle left in place connected to a tube with the D5W. This created a buffer zone with the intent to prevent thermal injury to the ipsilateral recurrent laryngeal nerve (RLN). 10 The electrode tip was advanced into the malignant node under ultrasound guidance using the medial-to-lateral approach. After identifying vital neck structures and establishing the presence of the tip in the treatment area, power was supplied to the electrode. Ablation was carried out until all visible parts of the lesion had changed to transient hyperechoic zones. To monitor RLN damage, the patient was asked to verbalize every minute. The procedure took 35 minutes and delivered 2065 joules of energy over a 59-second period of active ablation. Following the procedure, mobile vocal cords were identified via ultrasound.
Conclusion:
This video showcases the RFA technique for recurrent PTC in the thyroid bed performed in a private, outpatient endocrinology practice.
Patient Consent:
Authors have received and archived patient consent for video recording/publication in advance of video recording of procedure.
Disclaimer:
We report no Commercial associations that would create a conflict of interest in connection with this video.
The authors have no multiplicity of interest to disclose
.
Runtime of video: 5 mins 21 secs

Get full access to this article
View all access options for this article.