Abstract
Abstract
Introduction:
Recent studies report the incidence of intrathyroidal parathyroid adenomas to be between 1.3% and 2.4% in patients with primary hyperparathyroidism.1,2 The standard treatment for hyperparathyroidism caused by an intrathyroidal parathyroid adenoma has been surgery that often requires a lobectomy. 1 Treating primary hyperparathyroidism with radiofrequency ablation (RFA) has increasingly become an option as it has shown to be both safe and effective.3–7 We present a patient with primary hyperparathyroidism caused by a right-sided intrathyroidal parathyroid adenoma localized with fine needle aspiration (FNA) biopsy and parathyroid hormone (PTH) washout who is treated with RFA.
Case Description:
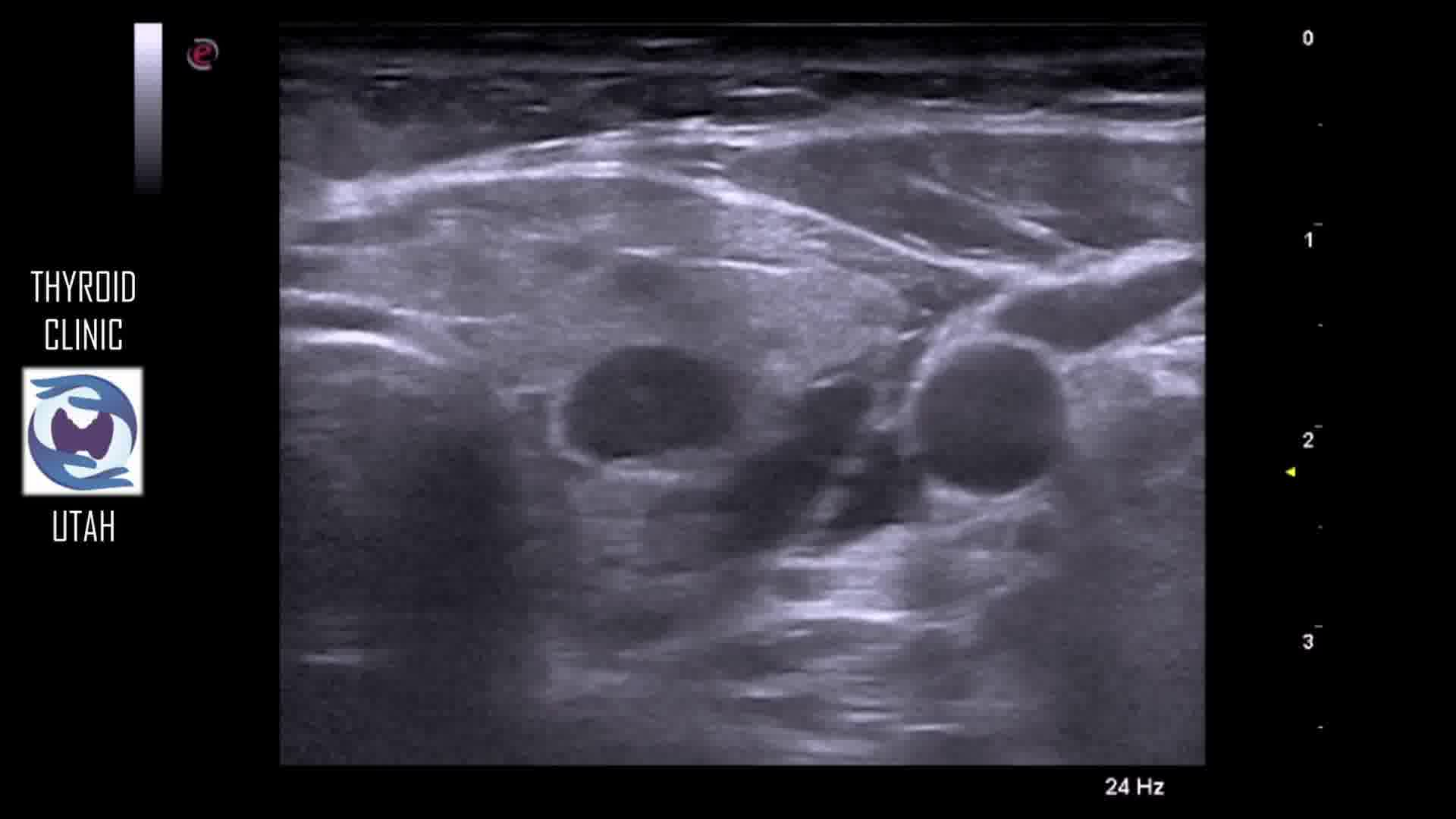
The patient is a 48-year-old woman with an intrathyroidal parathyroid adenoma localized on ultrasound in the right thyroid lobe inferior pole in the posterior medial aspect surrounded by a small rim of thyroid tissue and confirmed with FNA with PTH washout. The adenoma measured 0.8 × 0.6 × 0.5 cm (volume 0.12 cm3). Pretreatment laboratory values were calcium 10.8 mg/dL (8.4–10.4 mg/dL), PTH 133 pg/mL (22–94 pg/mL), 24-hour urine calcium 235 mg/24 hour, and Thyroid Stimulating Hormone (TSH) 0.49 µIU/mL. The patient was presented at a regional thyroid tumor board and also had consultation with a head and neck surgeon. There was consensus that a right hemithyroidectomy would be required to resect the parathyroid adenoma. The patient refused surgery and elected to have RFA for treatment as a potentially thyroid sparing treatment option.
Technique:
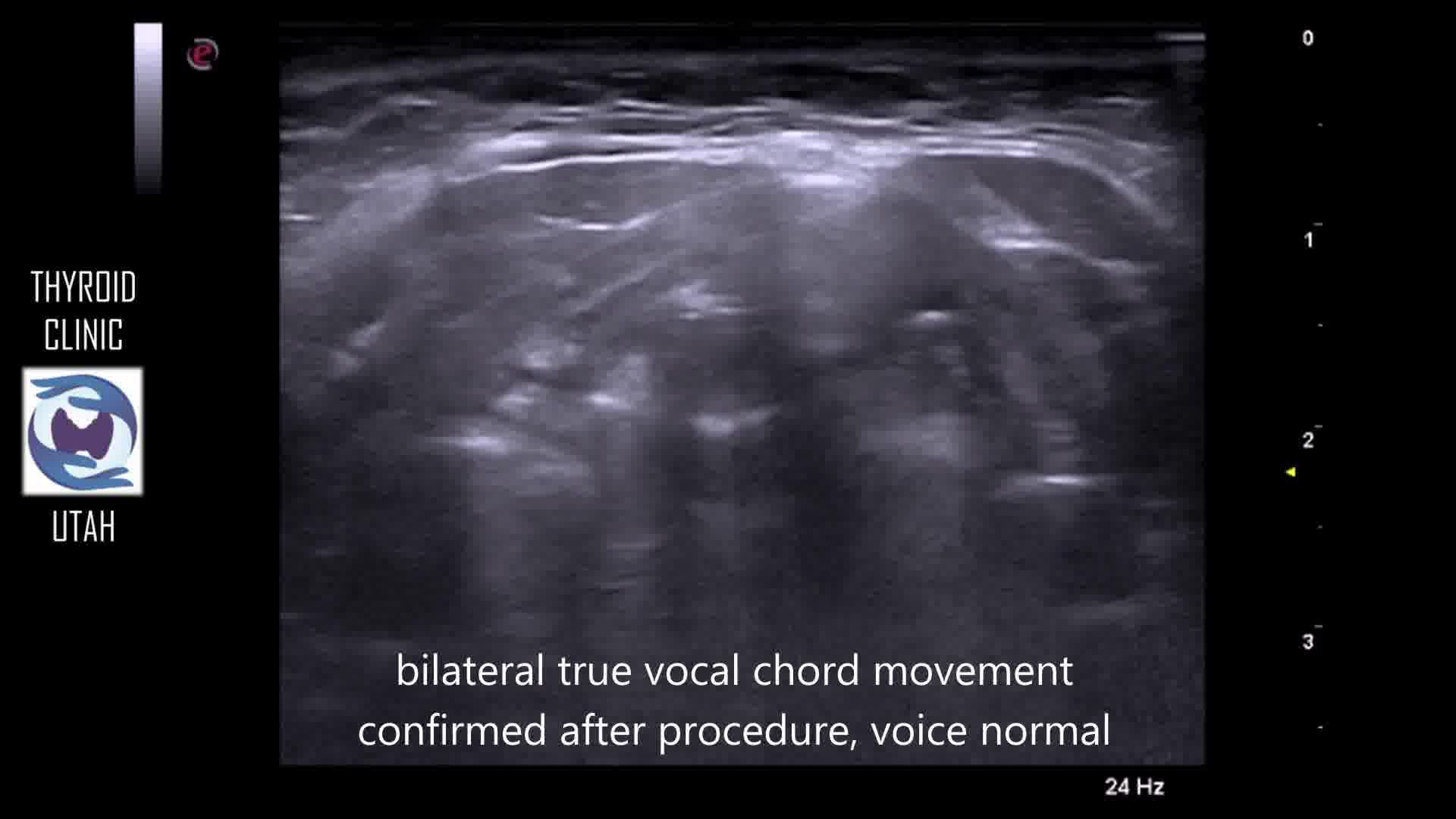
RFA was performed with an 18-gauge internally cooled electrode (Cambridge International, Burlington, MA) that was 12 cm in length with a 0.7-cm active tip and was powered by the CRF Generator (Cambridge International) at 35 W of power. Local anesthesia with lidocaine was used to provide adequate analgesia. Hydrodissection was performed to protect the surrounding normal tissue. A fixed ablation technique was used given the small lesion. The ablated area showed hyperechogenicity because of thermal ablation, and the electrode was then repositioned to continue the ablation in a different region until complete absence of vascularity was achieved; the total ablation time was 1 minute and 12 seconds.
Results:
Follow-up ultrasound imaging at 2 months showed a reduction in size of the targeted node to 0.7 × 0.4 × 0.4 cm (volume 0.08 cm3), showing a 53% volume reduction. Post-treatment laboratory values showed normalization of the calcium level to 9.2 mg/dL, PTH 80 pg/mL, and TSH 1.4 µIU/mL.
Conclusions:
RFA is a thyroid sparing treatment option for primary hyperparathyroidism caused by an intrathyroidal parathyroid adenoma, and perhaps preferred to surgery in this setting.
The authors have no relevant conflicts of interest
.
Runtime of video: 7 mins 12 secs