
Abstract
Abstract
Introduction:
Ultrasound (US)-guided microwave ablation (MWA) is one of the effective thermal ablation (TA) techniques for the ablation of sympathetic benign thyroid nodules.
Materials and Methods:
The cystic portion of the nodule was aspirated and flushed before TA. MWA with 30 W was performed using moving-shot technique. The patient gave informed consent.
Case:
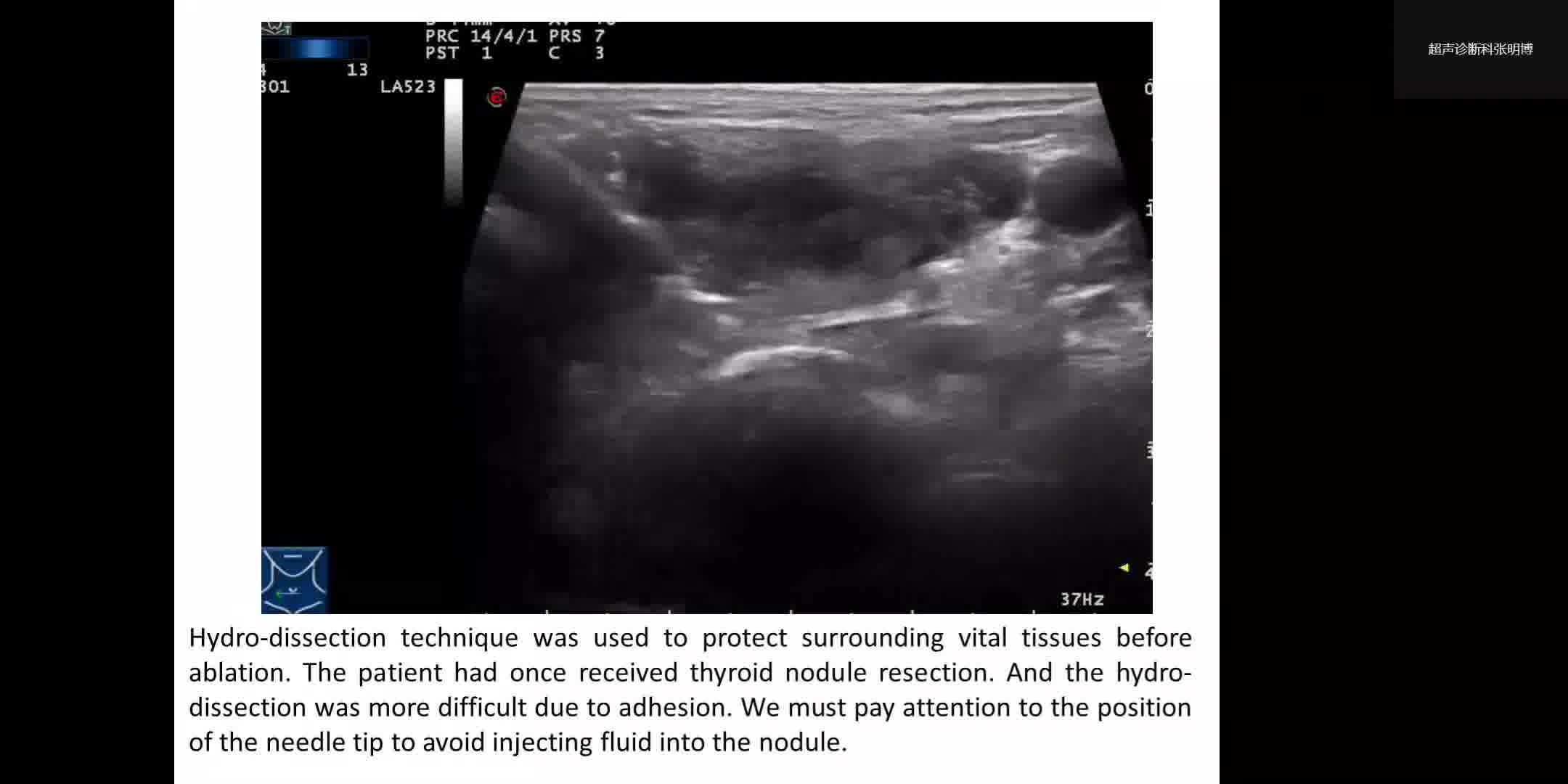
An 80-year-old woman complained of a right neck mass with neck pressure. The patient received partial thyroidectomy 20 years ago. At this time, the patient was symptomatic with dysphagia and neck pressure. Thyroid US revealed a cystic-solid nodule in right thyroid lobe, which was proved to be benign (Bethesda 2) by fine-needle aspiration cytology. It had the cystic composition of 90%, size of 5.1 × 4.3 × 5.4 cm, and volume 61.6 cc. After regular subcutaneous local anesthesia, a 16G papillary thyroid carcinoma was used to aspirate the cystic component, and 45 mL of stale bloody fluid with colloid was aspirated. Physiologic saline was used to flush the cystic repeatedly. Hydrodissection technique was used to protect surrounding vital tissues before ablation. Moving-shot technique was used to ablate the nodule. Contrast enhanced ultrasound confirmed complete ablation of the nodule.
Discussion:
This case illustrates the MWA technique in the treatment of cystic-solid benign thyroid nodules. Because of previous operation, the adhesion around the nodule made hydrodissection more difficult. Therefore, a small amount of fluid was injected at the beginning to see the tip of the needle and hydrodissection should be performed at both anterior and posterior space of the thyroid gland with larger amount of fluid. And attention should be paid to the position of the needle tip to avoid injecting fluid into the nodule. Although most of the fluid had been extracted from this nodule, there was still exudation and bleeding inside the nodule during ablation. The heat energy should not be applied to the fluid, but mainly to the wall of the cystic part, so the needle tip should be applied similar to an iron to ablate the wall of the capsule. Ethanol ablation (EA) is recommended as the first-line treatment for benign cystic thyroid nodules, instead of simple aspiration.1–3 However, TA has the advantage of predictable tissue destruction, and has replaced EA for the minimal invasive treatment for selected thyroid nodules.4,5 For this patient, the postoperative adhesions may increase the difficulty of surgical operation. In addition, the patient was 80 years old and TA is less invasive than surgical treatment and more reliable than EA to ensure the treatment completion to avoid recurrence. Studies have suggested that MWA can be a safe and effective treatment for patients with symptomatic benign thyroid nodules, as well as other TA techniques.6–10 In our hospital, the price for disposables of MWA is lower than the other TA technique. And it is the option at our disposal. Thus, we chose MWA for TA of this nodule.
Conclusion:
US-guided MWA can be an effective technique to treat large cystic-solid benign thyroid nodules and technical details should be noticed to ensure the effectiveness and safety.
No competing financial interests exist
.
Runtime of video: 5 mins 30 secs
Get full access to this article
View all access options for this article.