
Abstract
Abstract
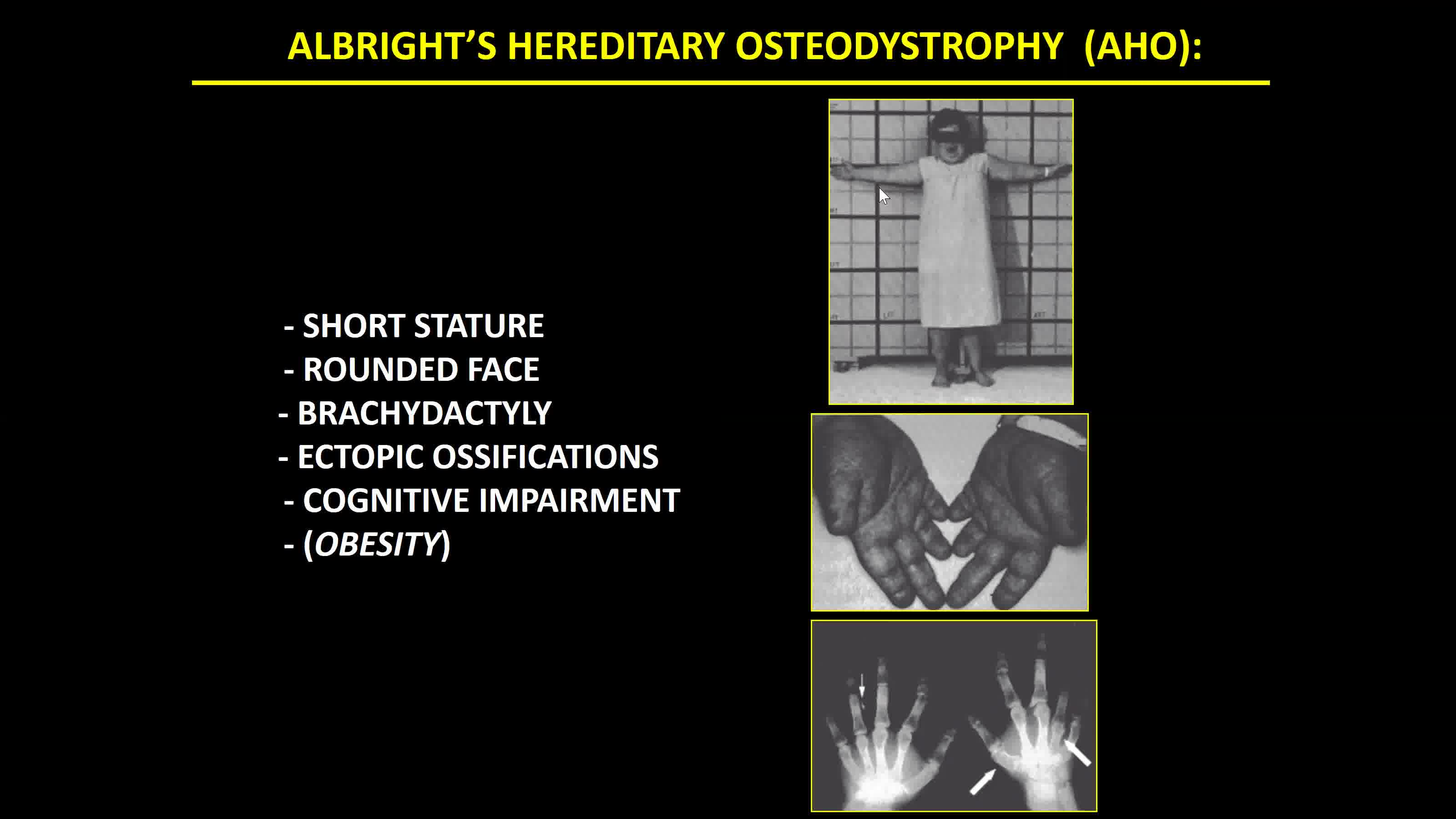
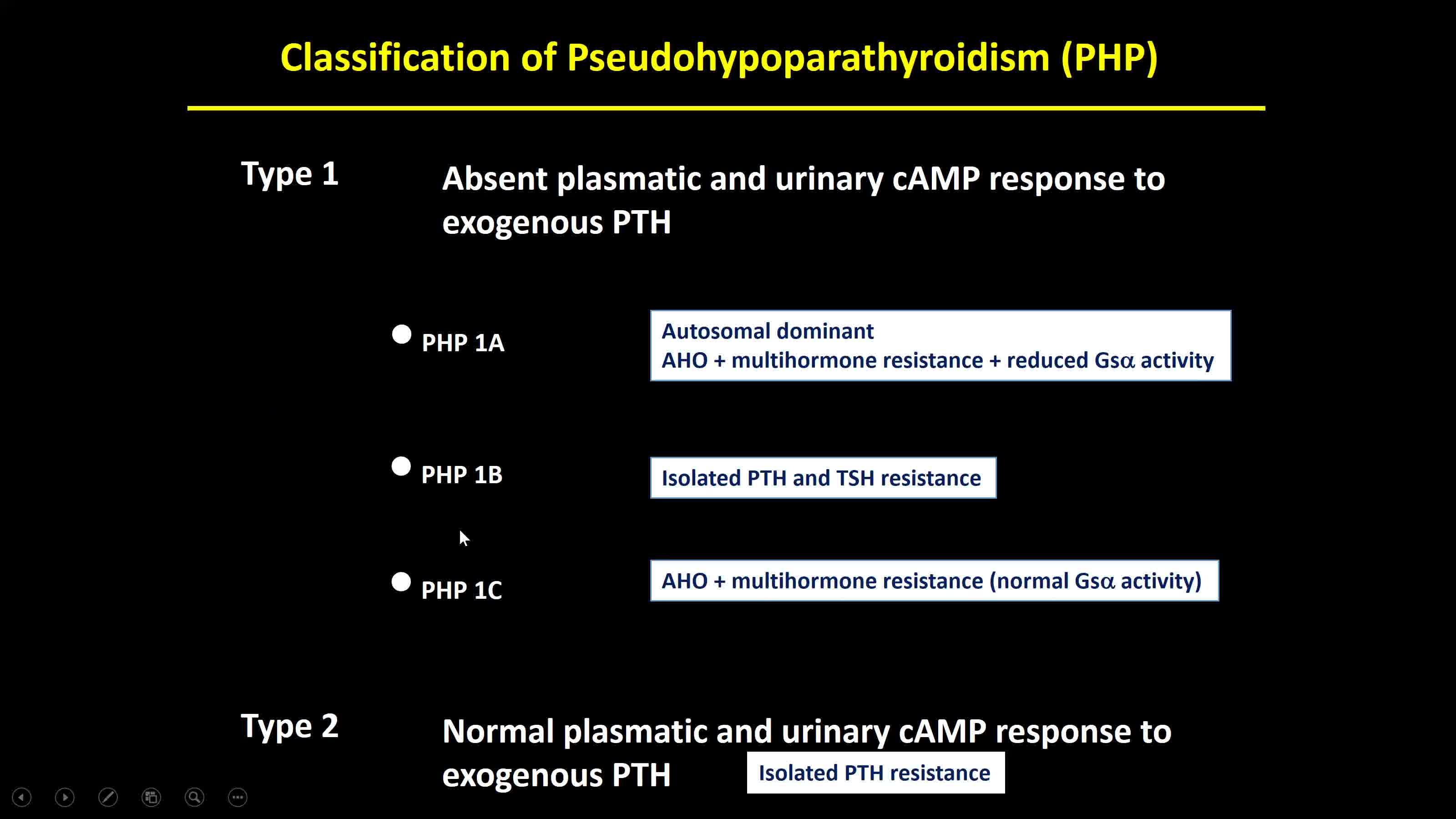
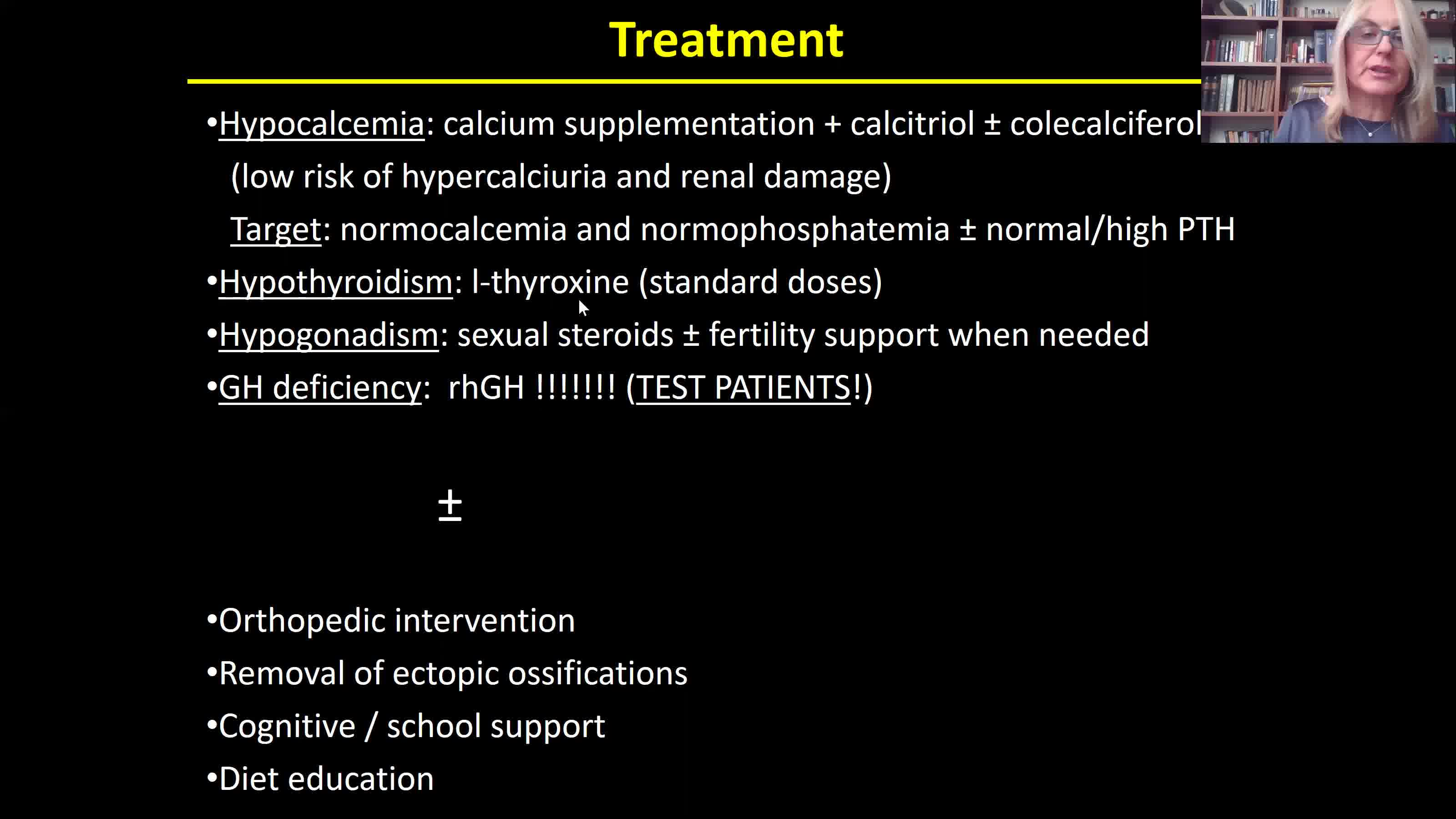
Different disorders derive from parathyroid hormone (PTH) deficiency (hypoparathyroidism), PTH excess (hyperparathyroidism), and PTH resistance (pseudohypoparathyroidism, PHP). Hypocalcemia increases PTH release and, after the exclusion of secondary hyperparathyroidism, elevated PTH levels should be investigated to identify patients with resistance to the action of this hormone. PHP was the first discovered syndrome due to hormone resistance. The growing knowledge on the PTH/PTHrp signaling pathway allowed to understand the existence of different related disorders in which PTH resistance is present and sometimes the major clinical manifestation and in which the underlying molecular defects affect members of the same signaling pathway in target cells. PHP and related disorders lead to a wide spectrum of abnormal physical characteristics, neurocognitive and endocrine abnormalities that share a common PTH/PTHrP signaling pathway. The clinical and molecular overlap of PHP and related disorders lead to difficulties in clinical and molecular diagnosis that prompt to the possibility of incorrect management of these patients. PHP (including all subtypes), pseudoPHP, acrodysostosis, and progressive osseous heteroplasia refer to heterogeneous disorders characterized by physical findings, differently associated in each subtype, including short bones, short stature, a stocky build, subcutaneous ectopic ossifications (features associated to Albright's Hereditary Osteodystrophy), as well as laboratory abnormalities such as hypocalcemia, hyperphosphatemia, and elevated PTH and TSH levels. Other features have been attributed to these disorders, such as intrauterine growth failure, early-onset obesity, hypogonadism, hypothyroidism, elevated calcitonin levels, growth hormone deficiency, and neurocognitive deficiency. The main subtypes of PHP and related disorders are caused by de novo or autosomal dominantly inherited inactivating genetic mutations, and/or epigenetic, sporadic, or genetic-based alterations within or upstream of GNAS, PRKAR1A, and PDE4D and PDE3A. The video gives an overview of this clinical spectrum and focuses on the clinical diagnosis, the molecular confirmation of the genetic or the epigenetic defect, up to the management of the most frequent manifestations.
No competing financial interests exist.
Runtime of video: 10 mins 52 secs
Get full access to this article
View all access options for this article.