
Abstract
Abstract
Background:
Papillary thyroid cancer metastasizes to the neck in ~60% of patients, necessitating lateral cervical neck dissection in cases of clinically evident metastasis. 1 The nodal pattern of metastasis is to levels II, III, IV, and V, with incidences of 52%, 57%, 41%, and 21%, respectively. 2 Given the rate of metastasis to level V, it is recommended to clear level V lymph nodes when performing a lateral neck dissection for metastatic papillary thyroid cancer. 3 Two commonly applied approaches exist for dissection of level V depending on the volume of disease present. An anterior approach is used when there is limited disease in level V, and a posterior approach is employed with bulky or extensive disease. This video outlines the two approaches to lateral neck dissection for papillary thyroid cancer metastatic to the lateral neck.
Methods:
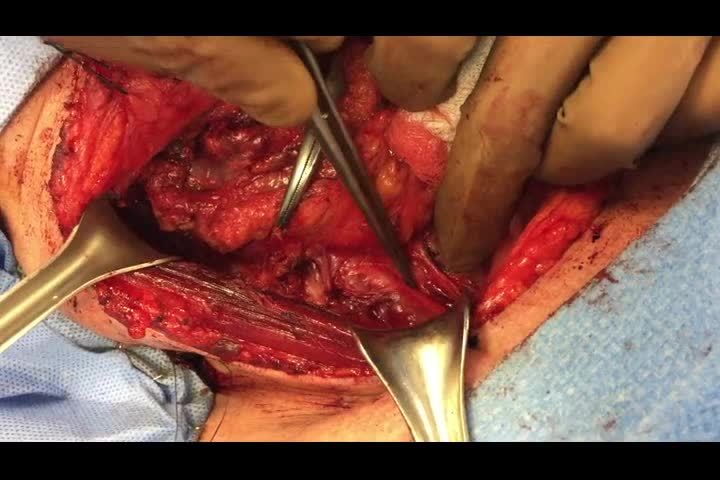
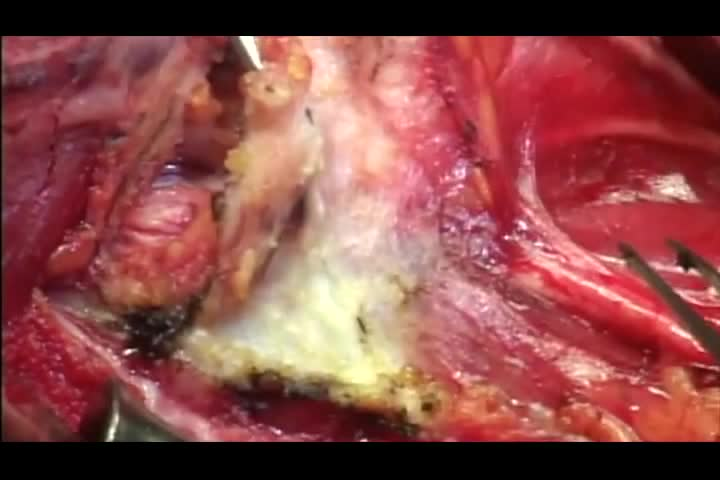
Video was created using iPhone 6 and edited in iMovie in patients undergoing right lateral neck dissection, levels II–V, for metastatic papillary thyroid cancer. An anterior approach is initially demonstrated, followed by a posterior approach in a separate patient. Written consent for video and photography was obtained for both patients.
Results:
Lateral neck dissection was effectively performed using both the anterior and posterior approaches to level V.
Discussion and Conclusions:
Clearance of level V lymph nodes is performed through either an anterior or posterior approach when performing lateral neck dissection for metastatic papillary thyroid cancer. It is recommended to employ the anterior approach when there is no clinically evident or limited metastasis in level V. The posterior approach is recommended when there is bulky or extensive disease.
No competing financial interests exist.
Runtime of video: 8 mins 51 secs
Presented at the 2017 World Congress on Thyroid Cancer held in Boston, MA.
Get full access to this article
View all access options for this article.