
Abstract
Abstract
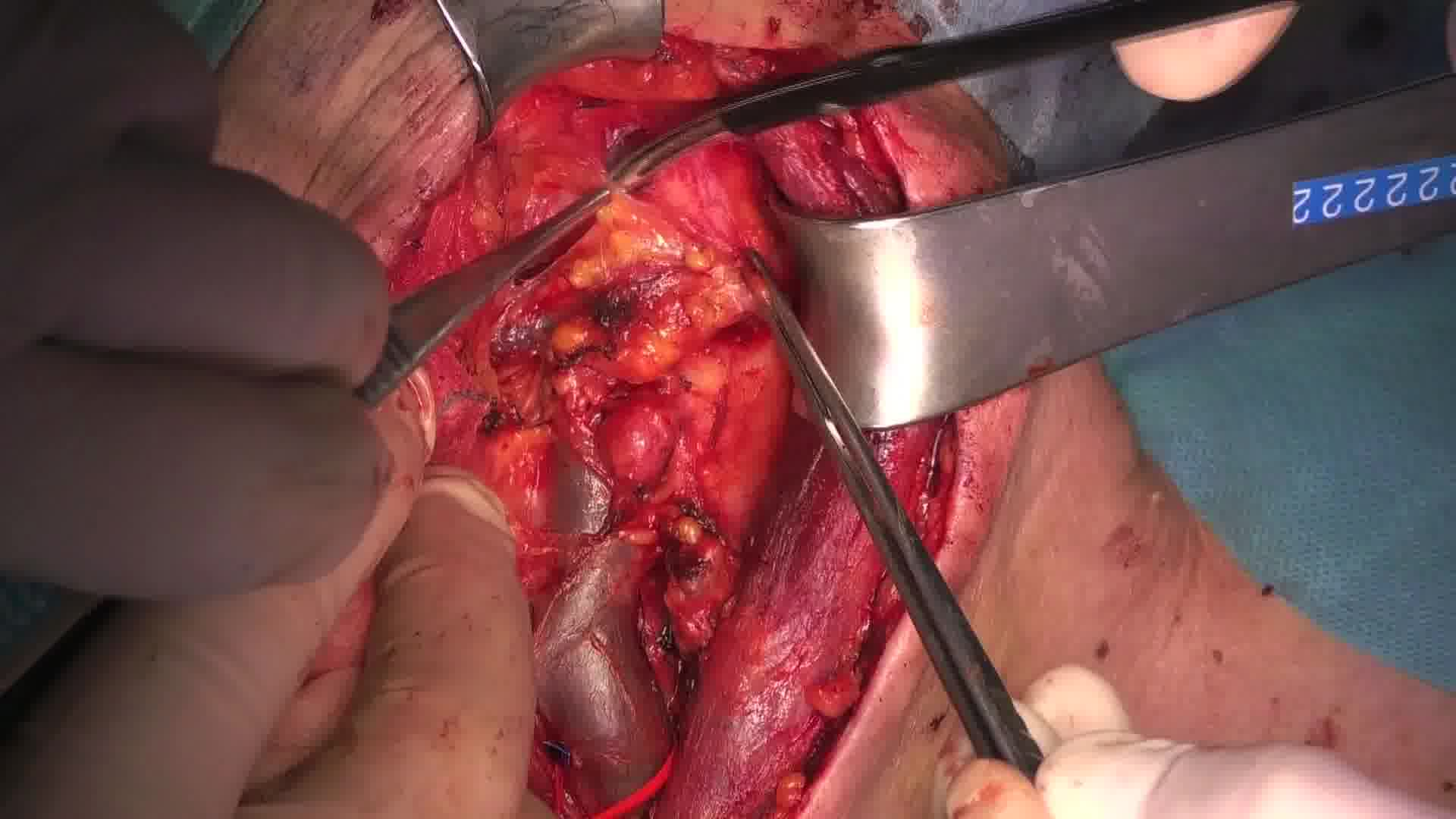
We present the case of a 50-year-old man with findings of enlarged level 3 nodes on the left side of the neck during the follow-up of a surgically resected papillary thyroid cancer. In anamnesis, he is obese (body mass index 37 kg/m2), with arterial hypertension, obstructive sleep apnea syndrome, and family history for thyroid cancer. When he was 47 years, he underwent a left lobectomy with isthmectomy with findings of adenoma and a papillary microcarcinoma. After 2 years, he underwent a totalization of the thyroidectomy for a growing nodule in the right thyroid lobe, negative for cancer. After a year, a follow-up neck ultrasonography showed enlarged left level 3 cervical nodes. Fine-needle aspiration cytology was positive for papillary cancer cells; therefore, a selective left neck dissection was planned. The L-shaped incision provides surgical control of the whole field, and it can guarantee surgical radicality both on cranial and on caudal cervical node levels. The selective neck dissection was targeted to levels 2a, 2b, 3, 4, and 5, sparing neck structure. Omohyoid muscle can be transected to better expose level 4 nodes, and it can be repaired at the end of the intervention. The only macroscopically involved lymph nodes were in level 3. There were no macroscopically pathologic lymph nodes in level 5b, therefore, in accordance with current guidelines we did not extend the resection to level 5a. Pathologic examination showed metastasis in 3 out of 26 lymph nodes. All the positive nodes were in level 3, the bigger node was ~3 cm in diameter. The postoperative course was uneventful, and he was discharged on second postoperative day. He started a suppressive therapy with levothyroxine. After 3 months he was given a dose of I-131 for persistent residual captation on a total-body positron emission tomography and computed tomography scan. After two years the oncological follow-up was negative for recurrence.
Authors' Contributions:
L.P., G.M., and F.C. performed surgery on the patient. L.P. and F.C. reviewed current evidence. L.P., F.C., and G.M. edited the video. P.D. reviewed the study and approved the final version to be submitted.
Acknowledgment:
The authors thank Claudio Martini for his valuable work in editing the video.
Consent:
Authors have received and archived patient consent for video recording/publication in advance of video recording of procedure.
Ethical Approval:
The study was approved by the ethics committee of the Ospedale Luigi Sacco—ASST Fatebenefratelli Sacco.
Data Availability Statement:
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
Runtime of video: 9 mins 32 secs

Get full access to this article
View all access options for this article.