
Abstract
Background and Objectives:
To pilot Project Extension for Community Healthcare Outcomes (ECHO) as a tool to expand access to stroke prevention education to more interprofessional health care professionals (HCPs) and leaders of local organizations. They may then provide primary stroke prevention to the vulnerable populations they serve, who may not have access to primary care providers or routine primary stroke prevention knowledge.
Methods:
Corewell Health neurologists provided an educational program through tele-education using the ECHO platform with five hour-long didactic sessions. Education about primary stroke prevention in women, African Americans, and Latinx communities was provided to community organizations throughout West Michigan and HCPs serving these populations. Participant surveys were used to assess the efficacy of the sessions. Survey results were prospectively obtained then analyzed before and after the program.
Results:
A total of 32/80 (40.0%) participants completed the pre- and post-program surveys. The pre-program survey (PREPS) had 10 knowledge-based multiple-choice questions and one Likert-scale experience-based question. The post-program survey (POSTPS) had the same pre-program questions with the addition of four Likert-scale experience-based questions. Statistical significance was approached with there being 6.0 ± 1.2 correct answers on the PREPS and 6.5 ± 1.0 correct answers on the POSTPS, p = 0.05 (confidence interval −1.00–0.00). 6 (18.8%) participants before the program versus 13 (40.6%) after the program strongly agreed that they are very confident in counseling someone on risk-factor modification for preventing a first-ever stroke. Twenty-eight (87.5%) participants agreed or strongly agreed that they would be interested in participating in the program again.
Conclusions:
We effectively piloted a primary stroke prevention education program about groups who are particularly at-risk for having a stroke. The ECHO platform has the high potential to be used in preventative pedagogy to address cerebrovascular inequities.
Introduction
Stroke is the fifth leading cause of death in the United States, with an overall prevalence of 2.6% in people over 20 years of age.1,2 Women have a higher lifetime risk of stroke, are less likely to get acute interventions such as thrombolytics, and have poorer functional outcomes after a stroke versus men. 3 The Latinx community has a higher cumulative incidence for ischemic stroke at younger ages, and Hispanic men are projected to have the highest increase in strokes by 2030. 4 African Americans are 50% more likely to have a stroke than Caucasians and 60% more likely to die from a stroke. 5 Such disparities result from higher occurrences of modifiable risk factors including obesity, smoking, alcohol use, sedentary lifestyle, hypertension, hyperlipidemia, and diabetes. 6
Members of these minority populations are less likely to seek formal medical care due to several potential barriers such as reduced access to primary care and neurologists, differing language, distrust resulting from gender and racial inequities within health care, and lack of health insurance or prohibitive financial circumstances.7–9 Providing medical education to community organizations and health care professionals (HCPs) that cater to minority populations enables them to disseminate vital information regarding risk modification in the primary prevention of strokes. A tool for providing this education is Project Extension for Community Healthcare Outcomes (ECHO), which is a hub-and-spoke telemedicine platform for sharing specialty medical knowledge with community providers and populations that may not otherwise have access to such expertise.
Project ECHO, originally introduced in 2003 to address disparities in hepatitis C care in the rural areas of New Mexico, has since been expanded and implemented worldwide, impacting hundreds of millions of patients. 10 The project has been used to mitigate educational disparities between primary care and hospital teams, most notably used today in diabetes management, chronic pain, osteoporosis, and cancer. 10 An area of particular interest has become neurological care, with recent case studies demonstrating the potential for the project’s utilization in stroke education. 11 The demand for neurology care greatly outweighs the supply of neurologists, with this disparity expected to widen. 12 A call for greater cross-training of primary care providers in acute neurology care is cited as a potential avenue to improve patient care while acknowledging the constraints with supply of the neurology workforce. 12 Project ECHO can facilitate this cross-training; however, it has previously not been used in addressing inequities in cerebrovascular care.
ECHO’s knowledge networks can also be applied to health outcomes research and the delivery of services to underserved communities.13–15 We hypothesized that ECHO can effectively educate community organizations to address primary stroke prevention in vulnerable populations upstream of clinic visits with medical providers. This may bridge gaps in health disparities including reduced access to medical care, language barriers, lack of health insurance, and racial distrust. Our objective is to implement ECHO as a tool to expand access to stroke prevention education to more interprofessional HCPs and leaders of local organizations so they may provide primary stroke prevention to the vulnerable populations they serve.
Methods
This study was funded by an internal foundation grant through Corewell Health. Corewell Health providers led two rounds of five virtual didactic sessions through the ECHO platform. CME and CEU credits were provided for participation and ensured utilization of evidence-based medicine as well as adherence to best-practice guidelines. HCP participants were recruited internally between October 2020 and January 2021 through the regional hospital system of Corewell Health and externally through the help of community organizations throughout West Michigan including the Grand Rapids African American Health Institute, Hispanic Center of Western Michigan, and local health clinics that cater to women, African Americans, and the Latinx community. Twenty-five regional organizations were asked to participate, of which 14 participated. HCPs included were social workers, care managers, counselors, nurses, nurse practitioners, occupational and physician therapists, and physicians. After inquiring with the Corewell Health Institutional Review Board, this study was determined to be exempt from IRB and ethics committee review.
The logistics of providing ECHO sessions using computers capable of audio, video, and microphone telenetworking, as well as session mediation was coordinated by MNI Great Lakes ECHO LLC (Grand Blanc, MI). The curriculum was comprised of interventions for lifestyle modifications that have shown to impact stroke prevention, which are smoking cessation, reduced alcohol intake, healthy diet, and adequate exercise.6,15 Specific didactic sessions are shown in Table 1 and were conducted between January 2021 to December 2022. Each session was an hour long with case-based teaching and included an interactive format between educators and participants. In addition to educator expertise, 2014 and 2013 AHA stroke prevention guidelines and 2013 AHA/ACC guidelines to reduce cardiovascular risk provided the framework for educational content.6,16
ECHO Didactic Sessions for Primary Stroke Prevention
ECHO, Extension for Community Healthcare Outcomes.
Results
Outcomes
Data were gathered prospectively. The outcome we assessed was at a participant level as we measured the efficacy of the program, evaluated surveys based on course content proficiency and the experience of program participants. Each pre-program survey (PREPS) survey had 11 total questions: 10 multiple-choice questions regarding educational content as it pertains to risk factor modification to prevent strokes and 1 question with a Likert-scale answer on a scale from 1 to 5, 1 being strongly disagree to 5 being strongly agree. Each post-program survey (POSTPS) had 15 total questions: 10 of the same multiple-choice questions on the PREPS, the same Likert-scale question from the PREPS, and four additional experience-based Likert-scale questions (Supplementary Table S1). These experience-based questions encompassed participant confidence in counseling on educational content, meeting program expectations, satisfaction with ECHO format and resources provided, and future interest in the program (Supplementary Table S1).
Data collection and analysis
Demographic data of providers and participants were collected. Surveys were performed online using Survey Monkey and Red Cap. Qualitative data were described as nominal (binary, yes or no fashion) or ordinal variables (ranked, 1 to 5). Numerical data were described as mean ± standard deviation for continuous variables. The number of correct answers was tallied for each PREPS and POSTPS. The mean correct answers were compared between PREPS and POSTPS using a paired samples t-test. A t-test was performed for univariate analyses to assess associations among variables. Statistical testing was done at the two-tailed α level of 0.05, and a 95% confidence interval was reported.
Results
A total of 32/80 (40.0%) participants including HCPs completed the PREPS and POSTPS. Demographic data of participants are shown in Table 2. Most participants were women (87.5%), Caucasian (81.2%), and were nurses or physicians (68.8%). In assessing our primary outcome, statistical significance was approached with there being 6.0 ± 1.2 correct answers on the PREPS and 6.5 ± 1.0 correct answers on the POSTPS, p = 0.05 (CI −1.00–0.00). Results are shown in Figure 1.

Percentage of Correct Answers on PREPS Versus POSTPS. PREPS, Pre-Program Survey; POSTPS, Post-Program Survey.
Demographics for Participants That Completed Surveys
Data are presented as n (%).
Six (18.8%) participants before the program versus 13 (40.6%) participants after the program strongly agreed that they are very confident in counseling someone on risk-factor modification for preventing a first-ever stroke. Thirty out of 32 (93.8%) participants agreed or strongly agreed the program met their expectations on learning about primary stroke prevention. Twenty-six out of 31 (83.9%) participants agreed or strongly agreed the program format was excellent, 30/31 (96.8%) that the resources provided throughout the program were useful, and 28/32 (87.5%) participants agreed or strongly agreed that they would be interested in participating in the program again. No one disagreed with having a positive experience, but one person strongly disagreed for their answers to all the experience-based questions (3.1%). The detailed breakdown is shown in Figure 2.
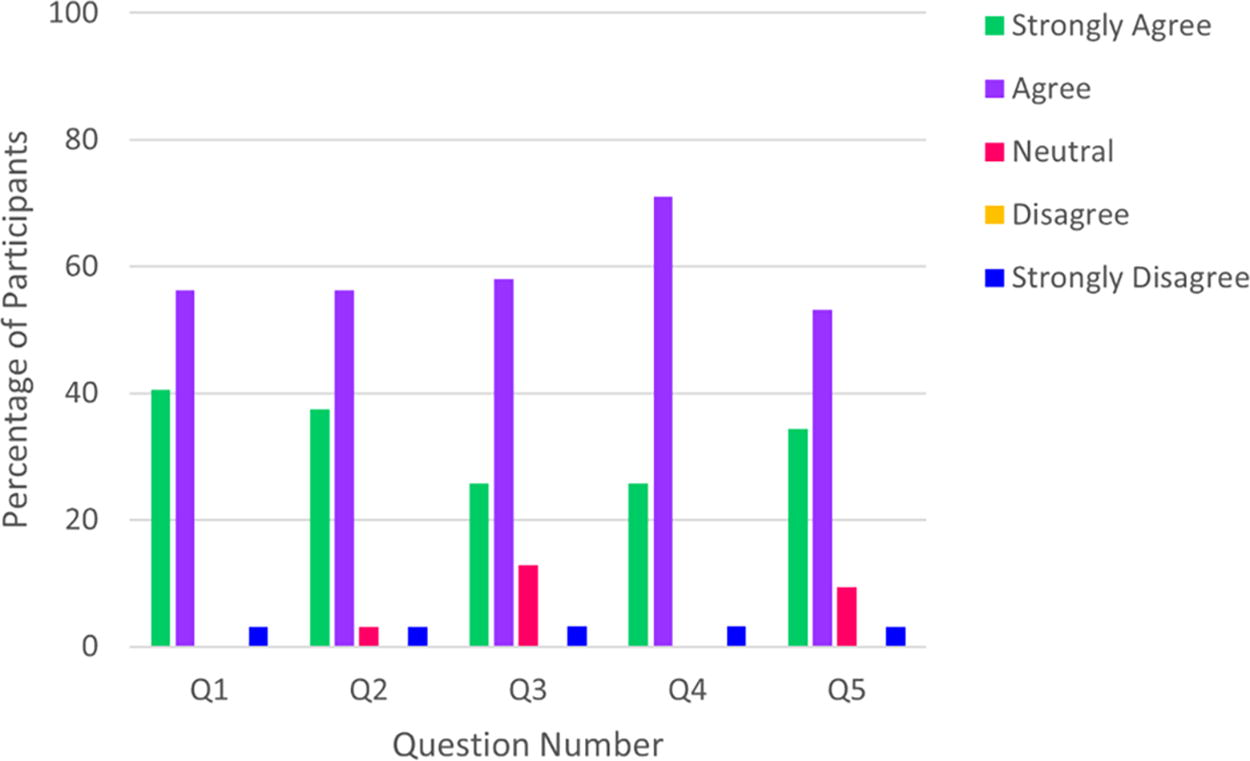
Qualitative Feedback on Program Experience (n = 31 for Questions 2 and 3, n = 32 for Questions 1 and 4).
Discussion
We were able to provide effective education through a pilot program using the ECHO platform to community HCPs and providers about primary stroke prevention in high-risk groups of women, African Americans, and the Latinx community. Though ideally, all 80 participants would have filled out the PREPS and POSTPS, of the 32 participants who did fill them out, more of them had correct answers to content-based questions after the program (p = 0.05) and agreed or strongly agreed that they are very confident in counseling someone on risk factor modification for preventing a stroke after the program (96.9%), that the session format was excellent (83.9%), that the resources provided were useful (96.8%), and that they would be interested in participating in the program again (87.5%). These high rates of positive feedback are in line with results of other studies that have used the ECHO platform.17–19
To our knowledge, this is the first study to use the ECHO platform for the purpose of preventative care in neurology and cerebrovascular diseases. ECHO has been widely used in a wide range of medical specialties, including in neurology to a far more limited extent.19–21 There are many neurological subspecialties that have yet to use ECHO, including in the realm of cerebrovascular diseases. Our findings indicate the benefits of the program and open the door to the use of the platform and the pedagogical framework we have created to potentially be used for other areas of preventative neurology, in and outside of the subspecialty of cerebrovascular diseases.
This pilot study also shows the potential for using ECHO to expand access to care, particularly for vulnerable and minority populations such as women, African Americans, and members of the Latinx community. The success of ECHO in expanding expertise and knowledge of specialty and subspecialty best-practices has been shown in the literature.22–27 In combination with national provider staffing shortages, the many barriers to accessing preventative care that vulnerable and minority populations encounter are addressed by this program in providing subspecialty expertise to a wide range of HCPs who traditionally do not possess such expertise including social workers, care managers, counselors, nurses, nurse practitioners, occupational and physician therapists, and physicians throughout the community. 28 In our study, HCPs were affiliated with community organizations that serve the high-risk populations the education was about, as well as local and regional hospitals and clinics throughout West Michigan. And HCPs who were able to get CME and CEU credits gained credit-hours in accordance with the number of sessions they were able to participate in.
In the future, we hope to be able to include a larger geographic area and increase the number of participants and HCPs, as well as assess direct patient-level outcomes as to whether our intervention lowers their stroke risk and prevents strokes. One participant strongly disagreed with all experience-based statements; it is unclear as to why they had this feedback as they did not add any details to the reasoning for their answers. There is also opportunity for improvement in the educational content based on qualitative feedback from participants as well as the quality of the questions asked in the PREPS and POSTPS. We plan to provide further ECHO sessions on this topic and will make improvements to the content, structure, and surveys in accordance with feedback, which will hopefully make even more of a positive impact for participants. We also aim to directly educate community members at the center of this study and assess the efficacy of the program at the patient level rather than just the HCP level.
Limitations
There were limitations to our study. The low n-size of participants who filled out the surveys underpower the findings of our study. Also, this study was a feasibility and developmental pilot and our first step in using ECHO. Therefore, our initial aim was to expand access to subspecialty expertise regarding primary stoke prevention to a wide range of interprofessional HCPs so that they may disseminate this knowledge to members of minority and vulnerable populations who are at high-risk for having strokes. However, our ultimate goal is to provide education directly to the members of these high-risk groups. We were limited by funding and the number of our local and regional connections to have a wide and deep enough reach to engage women, African Americans, and members of the Latinx community to have the ability to assess a direct impact on patient care. With subsequent iterations, we hope to gain more funding so we can assess patient-level feedback and outcomes, as well as include a broader range of participants in terms of specialty and geographics. Lastly, the majority of the participants in our study were female (87.5%); we are unclear as to why this is other than that perhaps the constitution of the organizations that we educated are more female than male. All participants were asked to take the surveys, and we did not focus on any particular demographic of participants.
Conclusion
We effectively piloted a primary stroke prevention education program using Project ECHO about groups who are particularly vulnerable to strokes. The ECHO platform has great potential to be used in preventative pedagogy to address cerebrovascular inequities. Our next step is to include members of high-risk populations as patients and to assess their outcomes before and after implementation of the ECHO program.
Footnotes
Acknowledgments
MNI Great Lakes ECHO LLC for helping coordinate the logistics of using the Project ECHO platform. Freddie Hildreth II, MPH, for help with statistical analysis.
Authors’ Contributions
T.C. authored, conceptualized, analyzed and acquired data, drafted, and revised the article. She had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Reports no disclosures. K.B.-S. authored, drafted, and revised the article. Reports no disclosures. A.A. authored, conceptualized, drafted, and revised the article. Reports no disclosures.
Data Availability Statement (DAS),Data Sharing,Reproducibility,and Data Repositories
All survey data are publicly available upon individual request.
Author Disclosure Statement
No relevant disclosures.
Funding Information
No funding was received for this article.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.