
Abstract
Introduction:
The prevalence of telehealth has witnessed a significant increase in various medical domains, especially in endocrinology. Telehealth brings about considerable advantages for both patients and health care professionals. However, despite these positive aspects, the growing prominence of telehealth is accompanied by certain challenges. This systematic review aims to assess the role of telehealth in endocrinology, including its applications, effectiveness, challenges, and implications for patient care.
Methods:
This study involved a thorough search using comprehensive techniques across databases such as PubMed/Medline, Embase, and Scopus. The studies were selected for a tailored adaptation of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) to enhance the clarity of our systematic review’s reporting.
Results:
This systematic review explores global telemedicine applications in endocrinology. Addressing various endocrine conditions, interventions utilize technology tools such as smartphones and applications, offering multifaceted utility from education and data gathering to screening and treatment. Notably, these interventions demonstrate adaptability during the COVID-19 pandemic. Positive outcomes include enhanced patient education, disease self-management, reduced complications, and improved glycemic control. However, drawbacks include the need for technical proficiency, perceived lower care quality, and potential privacy risks. These nuanced findings contribute to the discourse on telemedicine efficacy and limitations.
Conclusion:
In conclusion, telehealth holds significant potential in transforming endocrine care. While there are challenges to its implementation, the benefits it offers underscore its value as a health care delivery model.
Introduction
Recently, the application of new technologies in disease management has increased.1–4 Telehealth involves utilizing digital communication technologies to deliver health care services remotely. 5 It extends beyond patient care, also serving as a platform for disseminating information and providing education in the health care domain. 6 Endocrinology is a particularly well-suited field for telehealth because its focus is on data monitoring, chronic condition management, and lifestyle counseling, and the assessment of diverse endocrine conditions is mainly reliant on laboratory analyses, or imaging outcomes, rather than physical examination findings.7,8 Following the initial phases of the COVID-19 pandemic, during which telehealth saw a surge in popularity among patients, endocrinology stood out as one of the subspecialties experiencing a notable rise in telehealth visits.9,10 Given that diabetes ranks among the most prevalent endocrine disorders, imposing a considerable burden on patients, telehealth has emerged as a widely utilized tool in this realm.11,12 Its application is particularly prominent in diabetes care, notably in blood sugar control, diabetes management, and screening for diabetes.13,14 The increasing cost of health care and the need for enhanced treatment options are prompting more hospitals to explore the advantages of telemedicine. 15 Telehealth mitigates the workload for doctors and contributes to increased job satisfaction. 16 These facilitate the smooth sharing of information, ensuring the appointments occur on time. Telehealth offers advantages for patients by higher completion rates of visits and a reduction in the travel burden for patients, including reminders for medications and appointments. 5
Telehealth faces challenges related to factors such as ethnicity, age, language barriers, and limited access to technology.17,18 Hence, the drawbacks of telehealth, including cost implications, restricted accessibility to reliable internet connections and technology devices, privacy concerns as individuals may worry about the security of their personal health information, and reduced opportunities for physical interactions which potentially impact the quality of the patient–provider relationship, should be duly considered. 19
In this systematic review, the authors aimed to comprehensively evaluate the role of telehealth in the field of endocrinology, examining its applications, effectiveness, challenges, and implications for patient care.
Methods
To explore the landscape of telehealth in endocrinology, we chose a systematic approach. This involved a thorough search using comprehensive techniques across databases such as PubMed/Medline, Embase, and Scopus. The studies were selected for a tailored adaptation of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) to enhance the clarity of our systematic review’s reporting.
Search strategy
In collaboration with a research librarian, we carefully devised a search strategy targeting PubMed/Medline, Embase, and Scopus databases. Our key search terms were “telemedicine,” “diabetes,” and “endocrinology” Using various search functions, such as thesauruses, Boolean operators, truncation, and advanced searches, we conducted this thorough search on June 23, 2024. There were no restrictions on publication date or country of origin; however, our searches focused on studies of adults published in English (Appendix 1). Additionally, we expanded our search by reviewing the reference lists of the identified articles to find more probable relevant publications.
Study selection
The references were imported into Rayyan, an online systematic review tool, following their download into Endnote. Initially, two independent authors reviewed titles and abstracts based on inclusion criteria, with any inclusion-related questions referred to a third author for resolution. The third author independently examined a subset (5%) of study titles and abstracts for eligibility to ensure consistent adherence to inclusion criteria. All studies deemed for inclusion by at least one investigator underwent a full-text review. Studies marked for exclusion at the title and abstract level by one investigator were screened by a second investigator. If both agreed on exclusion, the study was excluded. The full-text review involved two independent reviewers, and conflicts were resolved through discussion.
Study eligibility criteria, including population, intervention, comparator, outcome, timing, setting elements, and additional criteria such as study design, language, and publication type, were organized. Four inclusion criteria guided literature selection: (1) the study had to be original; (2) the exposure included empirical data on adherence to data logging processes using advanced technology for adults with endocrinology components; (3) the outcome focused on the impact of telehealth in endocrinology; (4) risk estimates with 95% confidence intervals. Ultimately, among the publications, we identified a total of 40 studies deemed applicable. Excluded were conference abstracts, unpublished studies (dissertations and theses), editorials, opinions, and discussion papers.
Definition of terms
We identified key elements to abstract from eligible literature to gather essential evidence on conducting telehealth visits across various clinic settings. Building on this foundation, we examined the relationship between clinical visits and telehealth modalities (e.g., telephone, video, and in-person) outcomes. Our telehealth interventions aligned with a well-defined telehealth concept, encompassing crucial contextual factors such as delivery mode (telephone, video, and in-person), dose (duration and frequency of contact), and the clinical context of care provision. Moreover, we specified that telehealth-delivered care should pertain to clinical activities conducted by the prescribing clinician, such as evaluation, diagnosis, or medication prescription. It excluded interventions such as self-management education or other support provided adjunctively by a clinical team member other than the prescribing clinician (e.g., nurse care manager), as these have been previously evaluated.
Quality and risk of bias assessment
To optimize the quality, this review study benefits from the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist. To minimize any probable bias risk, we utilized the Newcastle-Ottawa Scale (NOS) risk assessment tool (Table 1). Worthy to mention that a total score of nine in three categories is calculated in this numerical bias assessment tool. These three categories include selection, comparability, and exposure/outcome. Numerical values of four, two, and three are attributed to these categories respectively.
Newcastle-Ottawa Scale Bias Risk Assessment of the Study
Data extraction and synthesis
We presented a comprehensive summary of the primary literature, extracting relevant data from eligible studies. Summary tables delineate key characteristics, including study design, patient demographics, and details of the intervention and comparator. Due to conceptual heterogeneity in the structure, purpose, and delivery of telehealth visits, we opted not to conduct a meta-analysis. Instead, we provided a narrative description, emphasizing the identification of patterns in the efficacy and safety of interventions across conditions and outcome categories. Continuous outcomes were synthesized using the mean patient-level difference (follow-up minus baseline) when reported on the same scale. For studies without direct reporting of mean and standard deviation (SD) of patient differences, we calculated the difference in means between follow-up and baseline. If only baseline SD were reported, we assumed the same SD at follow-up. Without other information, a conservative 0.5 correlation between follow-up and baseline measures was assumed.
Results
Overview of included articles
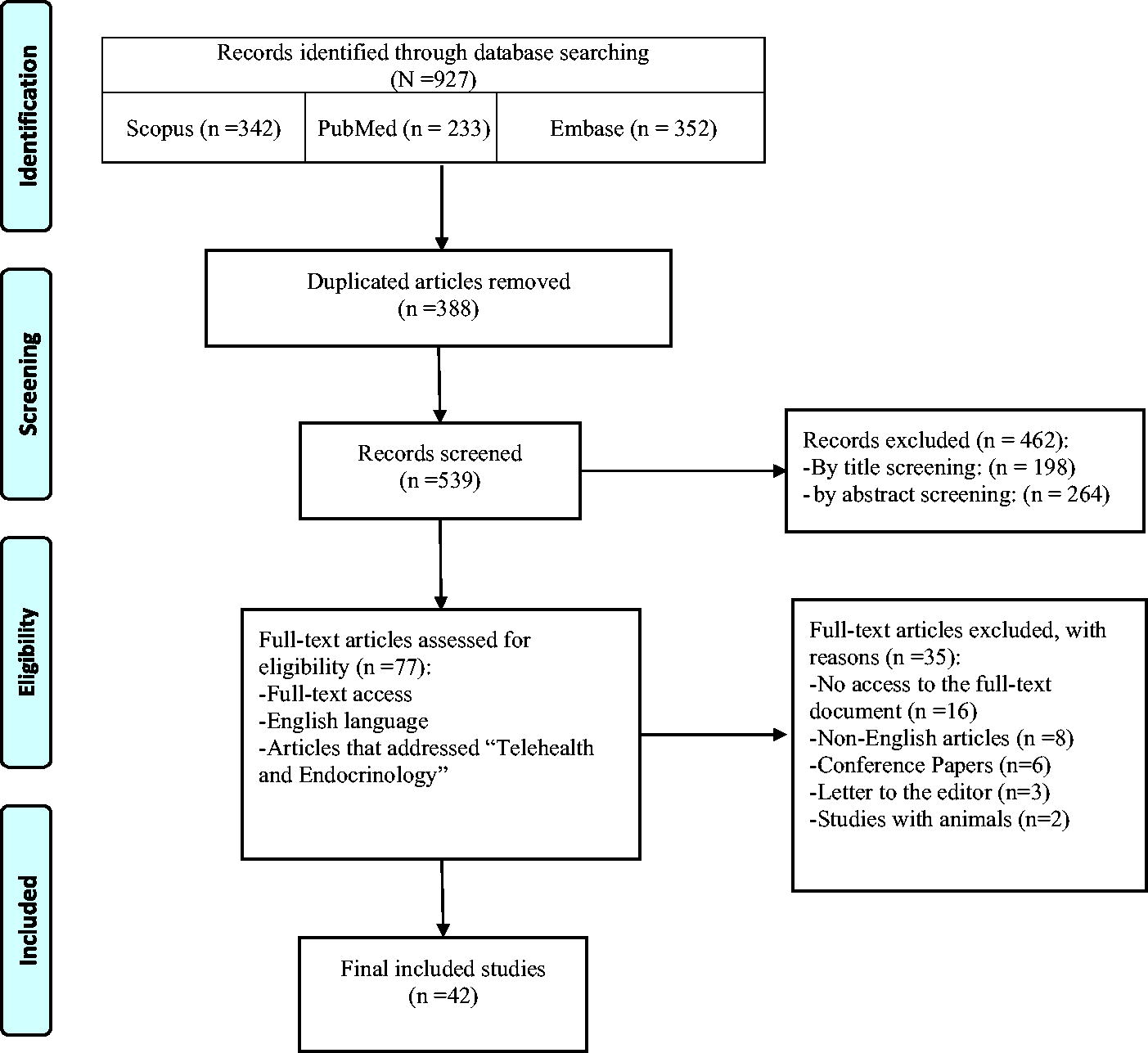
This systematic review comprehensively examines global telemedicine applications in endocrinology, covering studies conducted between 2004 20 and 2024,21,22 with more than half of the articles being published post-2018. We included 42 articles for full-text review (Fig. 1). As shown in Table 1, according to the NOS risk assessment tool, out of 42 included articles, 5 articles were of good quality (≥6), 13 articles were of fair quality (5≥, >2), and none of the articles were of poor quality (2≥).
Telehealth and endocrinology: A systematic review.
The research, involving over 25,000 participants, spans diverse countries, with notable contributions from the United States of America,23–34 Pakistan,35–37 Turkey,38,39 India,40,41 Korea,20,42 Australia,43,44 Saudi Arabia,45,46 China, 21 and Iran.22,47 We reviewed incorporating varied study types, such as randomized controlled trials,32,35,36,38,41,44,48–52 observational studies such as cohorts,20,23,24,29–31,45,53–55 case-controls, 56 and cross-sectional studies.25,26,33,46,47,57,58 The mean age of participants varied from less than one year 54 to 68 years, 53 demonstrating the wide applicability of telemedicine across various age demographics. In terms of gender distribution, most studies included both male and female participants. However, a study focusing on telehealth visits for patients dealing with reproductive endocrinology and infertility issues was an exception, as it exclusively featured female participants 25 (Table 2).
Details of the Included Articles
RCT, Randomized Controlled Trial.
Telemedicine interventions and target groups
The majority of the studies primarily focus on patients as the target group for telemedicine interventions. However, one study targets endocrinologists and compares their performance in virtual visits versus in-person visits. 26 Telemedicine interventions have been applied to a wide array of endocrine conditions. The majority of these interventions were targeted toward Type 1 and Type 2 diabetes mellitus.17,20,23,34,35,39,41,44,45,47,48,51,52,60 Other areas of focus included pediatric endocrinology,33,38,54,61 obesity, 55 reproductive and fertility complications, 25 and thyroid disorders.24,57 Additionally, telemedicine was utilized for screening conditions, such as diabetic retinopathy.27,30,46 The interventions employed a variety of technology tools. Smartphones17,29,32,36,42,45,47,60 and mobile applications41,45,49,50,52,56,61 were frequently used, along with traditional communication methods such as phone calls23,35,40,51,57,58 and emails.23,38,51,57,61 Other tools included SMS,20,37,39,40,53 video/audio visits,26,33,43,44,48,49,55 social messengers such as WhatsApp,39,58 and web-based24,59 platforms. In certain cases, specialized equipment such as teleophthalmological cameras and devices were also utilized.27,30,46 Telemedicine interventions demonstrated a multifaceted utility, serving various purposes. These ranged from education29,32,34–38,40,52 and data gathering17,24–26,36,39,42,47,54,61 to screening27,30,46 and treatment.20,23,32,38,43–45,48,49,51,53,55–60 Notably, these interventions provided enhanced support for chronic conditions, particularly during viral pandemics (Table 3).
Description of the Findings Reported in Included Studies
CFP, color fundus Photography; CGM, continuous glucose monitoring; DM, diabetes mellitus; DR, diabetic retinopathy; ED, emergency department; FFA, fundus fluorescein angiography; FTF, face-to-face; HDL, high-density lipoprotein; IP, in-person; MBG, mean blood glucose; NMFP, nonmydriatic fundus photography; OCT, optical coherence tomography; PCOS, polycystic ovary syndrome; PCPs, primary care providers; PE, physical examination; REI, reproductive endocrinology and infertility; SBP, systolic blood pressure; SMBG, self-monitoring of blood glucose; SMS, short message service; TH, telehealth; TIR, time in range; UWF, ultra-widefield fundus; VDC, virtual diabetes clinic; WHO, world health organization.
Outcomes of the interventions
Our review elucidates the primary objectives of telemedicine interventions in managing chronic endocrine conditions. These interventions effectively address issues such as access barriers,24,25,43,49,54,58 timely monitoring,20,38,44,50,57,59,60 and glycemic control in diabetes29,31,39,42,45,48,50,59 Most important, they also enhance patient education and self-management of their disease, provide lifestyle advice,23,32,34–37,41,47,51,52,55,56,61 and contribute to the reduction of costly complications.27,35,40,51 Notably, these interventions have proven particularly beneficial during the COVID-19 pandemic, demonstrating the adaptability and resilience of telemedicine in times of viral outbreaks.17,38,57
The positive outcomes of telemedicine interventions were manifold and significant. These interventions led to high levels of patient satisfaction,24,25,45 reduced HbA1c levels,20,23,48–50,52,56,58 improved self-care behaviors,32,35,38,41,44,47,50,52,55 and decreased glucose variability.42,51,60,61 Also, some studies showed it lowered the complications and hospitalizations in patients.23,53 Telemedicine was particularly effective during the COVID-19 pandemic, reducing infection risk38,45 and facilitating health care access.25,29,43,45,57 For instance, one study reported a significant decrease in HbA1c levels from 8.3% at the start to 7.8% at the end of the study (
Discussion
The recent decades have witnessed significant technological advancements, the implications of which are increasingly being realized in the medical sector. The incorporation of these advancements into medical practice has transformed caregiving, introducing a new paradigm in patient care. Telehealth applications, in particular, have found extensive use in various medical fields, including endocrinology, serving as a platform for remote patient monitoring, consultation, disease management, and medication adjustment. As of 2019, 76% of U.S. hospitals had adopted some form of telehealth modalities. 62
The onset of the COVID-19 pandemic presented unprecedented challenges in health care delivery, necessitating the adoption of innovative solutions to optimize and ensure care delivery. This led to an accelerated integration, utilization, and development of telehealth, which can address traditional caregiving difficulties and problems. 63 Numerous studies have highlighted the effectiveness of telehealth solely or in conjunction with traditional health care, particularly during the COVID-19 pandemic, while also acknowledging its limitations.64–66
Telehealth has found applications in a wide range of medical fields, including cardiovascular diseases, pulmonary diseases, dermatology, nephrology, psychiatry/psychology, neurology, multidisciplinary care, 67 cancer treatment, 68 and pediatric care. 69 Endocrinologists had adopted telehealth as a standard care modality even before it became mainstream in other medical fields and before the COVID-19 pandemic. 70 This can be attributed to the chronic nature of endocrine disorders, which primarily involve patient history taking, laboratory, and imaging results, rather than physical examination. Moreover, endocrine diseases necessitate long-term follow-ups, which can be conveniently facilitated through telehealth.
Telehealth offers several benefits, such as improved access to health care services, especially for patients in remote areas with a shortage of health care professionals 7 and elderly people. 71 It enhances patient satisfaction by saving time and eliminating unnecessary travel, thereby reducing associated costs. Telehealth also mitigates the risk of infections acquired from health care facilities. 72 The user-friendly nature of telehealth can lead to greater satisfaction, 45 acceptability, and feasibility, 73 resulting in higher attendance than in-person visits and a higher visit completion rate.19 Furthermore, telehealth has the potential to improve health outcomes by enabling timely intervention and promoting patient engagement in self-care and adherence to therapy. 74 It also serves as an effective medium for delivering health education, 75 physical activity, and diet monitoring. 76
However, the implementation of telehealth in endocrinology is not devoid of challenges. Successful execution of telehealth requires resources and extensive infrastructures allocated to health care systems by administrations and governments. 65 This increases technology-related costs 77 which may not be feasible, especially in low- and middle-income countries. Technical issues, such as poor internet connectivity 78 and lack of hardware equipment such as smartphones, wearables, and laptops, can impede care delivery. 65 Additionally, the absence of physical interaction may limit the clinician’s ability to conduct comprehensive assessments.26 There are also concerns about the quality of care delivered via telehealth, with some patients and providers preferring traditional in-person visits due to technology illiteracy 79 or the inability to reach treatment goals. 66 Moreover, with the advancement of electronic health records and large databases, patient data privacy has become a contentious issue, necessitating the adoption of regulatory parameters. Insurance reimbursement considerations can also pose a barrier to the effective implementation of telehealth. 77
In the realm of telehealth and endocrinology, our systematic review presents a novel approach by encompassing all endocrine conditions, rather than focusing solely on specific diseases. This comprehensive scope allows for a more holistic understanding of the implications of telehealth in endocrinology, thereby filling a significant gap in the existing literature. Our findings largely align with previous research, underscoring the benefits of telehealth such as increased accessibility, cost-effectiveness, and patient satisfaction. However, we also acknowledge the limitations, including technological barriers, data security concerns, and the potential for reduced interpersonal interaction. Our review suggests that the advantages of telehealth in endocrinology significantly outweigh the drawbacks, reinforcing its potential as a transformative tool in health care delivery.
Despite these challenges, the future of telehealth in endocrinology appears promising. With advancements in technology and growing acceptance among patients and providers, telehealth is poised to become an integral part of endocrine care. Further research is warranted to develop more robust evidence to establish guidelines for its use and to explore its potential in managing endocrine disorders in hard-to-reach populations. From a policy perspective, it is imperative to create a conducive environment for the adoption of telehealth. This includes addressing regulatory issues, reimbursement policies, and ensuring the privacy and security of patient information.
Limitations
In this study, we studied the available recent resources on telehealth applications in endocrinology. Considering the broadened telehealth field, many studies did not differentiate between the different technologies used, and we had to perform a very careful screening to include more relevant studies. Also, some of the included studies did not clearly address the pros and cons of telehealth technologies for endocrinology.
Conclusions
In conclusions, telehealth holds significant potential in transforming endocrine care. While there are challenges to its implementation, the benefits it offers underscore its value as a health care delivery model. In the right context, such as appropriate diseases that can benefit from telehealth implementation and suitable infrastructures, it can be beneficial. In the coming years, with deeper integration of electronic medical records with telehealth systems and technological advancements such as high-speed connections such as 5G internet, which comes at lower costs, telehealth is projected to mature and surpass in-person encounters in terms of attendance. As we continue to navigate the digital health landscape, it is crucial to leverage telehealth solutions to enhance the quality of care in endocrinology.
Footnotes
Acknowledgment
The present study was conducted in collaboration with Khalkhal University of Medical Sciences, and Tehran University of Medical Sciences.
Authors’ Contributions
The conception and design of the study: E.M., S.S. Acquisition of data: S.D., P.M. Drafting the article: E.M., S.D., P.M., F.A., S.Y., S.A., F.A., A.P., A.M., A.P., S.A. Revising it critically for important intellectual content: S.S., E.M. Final approval of the version to be submitted: S.S., E.M.
Availability of Data and Material
The authors stated that all information provided in this article could be shared.
Author Disclosure Statement
The authors declare that there is no conflict of interest regarding the publication of this article.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.