
Abstract
Background:
Telemedicine involves medical practice and information and communications technology. It has been proven to be very effective for remote health care, especially in areas with poor provision of health facilities. However, implementation of these technologies is often hampered by various issues. Among these, ethical and legal concerns are some of the more complex and diverse ones. In this study, an analysis of scientific literature was carried out to identify the ethical and legal challenges of telemedicine.
Materials and Methods:
English literature, published between 2010 and 2019, was searched on PubMed, Scopus, and Web of Science by using keywords, including “Telemedicine,” “Ethics,” “Malpractice,” “Telemedicine and Ethics,” “Telemedicine and Informed consent,” and “telemedicine and malpractice.” Different types of articles were analyzed, including research articles, review articles, and qualitative studies. The abstracts were evaluated according to the selection criteria, using the Newcastle–Ottawa Scale criteria, and the final analysis led to the inclusion of 22 articles.
Discussion:
From the aforementioned sample, we analyzed elements that may be indicative of the efficacy of telemedicine in an adequate time frame. Ethical aspects such as informed consent, protection data, confidentiality, physician's malpractice, and liability and telemedicine regulations were considered.
Conclusions:
Our objective was to highlight the current status and identify what still needs to be implemented in telemedicine with respect to ethical and legal standards. Gaps emerged between current legislation, legislators, service providers, different medical services, and most importantly patient interaction with his/her data and the use of that data.
Introduction
Telemedicine has been shown to be especially useful in underserved communities where there is a shortage or absence of adequate clinical care, such as in remote areas. For the first time, in developed and developing countries alike, proven, reliable and cost-effective telemedicine and telehealth services are available at scale. 1 Thus, thanks to robust enabling technology infrastructure, the great promise of telemedicine has finally arrived. Rather than move the patient to the clinical specialist, it is now commonplace to harness the power of technology to transmit the knowledge of the specialist right to the patient in need. 2 Therefore, this progressive change in health care can open up new doors in legal, ethical, and regulatory issues and have a great impact on decision policy making by health authorities. 3 In this context, artificial intelligence (AI) plays an important role to enhance standards of care. 4 The authors want to specify that in this article, the term telehealth is in relation to those articles focusing on telemedicine. Operationally, telemedicine covers two broad areas. The first is the virtual interaction between patient and doctor and treatment prescribed and the second is the flow of information.
For example, misdiagnosis can occur in both face-to-face and virtual interactions. However, the former has a detailed mechanism from patient complaints to investigation and compliance standards. The growth of telemedicine is rapid and could lead to future cost savings. 5 However, the risk of misdiagnosis is greater and the legal statutory clauses are not standardized or universal. This often leads to varying standards and coverage offered by service providers, including the dangers of a decrease in quality of handling ethical and legal concerns to be ahead of the competition. 5,6
The cost of telemedicine services is practically the same as that of services performed in face-to-face interactions. There is no assurance of pay equality among in-person health care and telemedicine providers. On the other hand, liability and potential issues such as negligence and malpractice will also have an impact on telemedicine. 5 –7
Telemedicine provides several benefits such as improving access and quick patient engagement at a cheaper cost, but ethical and legal challenges need to be taken into account while implementing telemedicine programs. 8 For example, some countries have described prerequisites for getting an educated permission, especially for telemedicine, to make sure patients follow the privacy risks and essential techniques of telemedicine. These regulations in telemedicine training policies of patients might vary from verbal policy explanation to written consent. 8,9 Overcoming legal issues in telemedicine can be a long and complicated process; however, they are not impossible to understand. To make progress, it is first important to know the current status.
Materials and Methods
Searching Strategy
The research reported here was carried out on the scientific literature between February 2010 and March 2019 in the online databases of PubMed, Scopus, and Web of Science (WoS). The search in the databases was carried out using the following keywords: “telemedicine,” “Ethics,” and “Malpractice” either in free form—with the following search strings: “telemedicine and Ethics,” “Telemedicine and Informed consent,” and “telemedicine and malpractice”—or by combining the words between them. In the latter case, we used the “AND” Boolean operator and reported the following search strings in PubMed, Scopus, and WoS: “Telemedicine and medical ethics ‘AND’ Telemedicine is a risk factor for medical malpractice and liability.”
The authors operated the preliminary assessment independently by reading the abstracts and drafting a list of the articles that they considered eligible. Then, the aforementioned lists were compared for discrepancies, and when one was individuated, the different ideas were discussed to reach a consensus. Once the authors decided which articles were worthy to be included in the review, they read all the articles to gather data useful for the purpose of the research effort. The information evaluation was conducted independently and opinions compared to formulate a consensus.
The review includes research articles published in the last 9 years (2010–2019) and in all sectors where telemedicine is most active. The following sectors emerged: teleneurology, teleradiology, telemedicine for nursing, telemedicine for mental health, geriatric telemedicine, teleoculistic, and medical ethics. Prior studies were considered unusable for the purposes of the review because the first practical applications of telemedicine were found to be documented starting from 2010.
Selection Criteria
The research initially provided 210 results, characterized by publications potentially relevant to the objectives of this study. Specifically, 110 works were found in PubMed, 80 in Scopus, and 20 in WoS. The types of study objects of interest were the following: original articles, analytical studies, and literature reviews. The inclusion criteria that guided the selection of the works were (1) type of study: analytical studies, original articles, and literature reviews published in the last 9 years (2010–2019 in January only), publications in English with full text available; and (2) articles that had an interest population of remote patients to be treated with telemedicine in each of the different medical specialties. The exclusion criteria were (1) studies with different characteristics compared with the inclusion criteria and (2) studies that took into consideration only technical and engineering aspects of medical devices used in telemedicine.
Following the examination of the abstract studies taken into consideration, further 150 articles that were not pertinent to the objectives of this study were eliminated for the following reasons: 65 articles were concerned with technical and engineering aspects of medical devices; 55 articles evaluated only the efficiency of the devices used for application of telemedicine; and 30 articles focused on the degree of patient satisfaction in using telemedicine solutions. Twenty-four articles, relevant to the objectives of this review, were identified. Of these, following the reading of the full-text version, two were excluded because they analyzed the relationship between patient and technology and therefore did not fall within the previously specified inclusion criteria.
Quality Evolution
Newcastle–Ottawa Scale 10 was employed for quality check of selected studies. The overall quality was determined as very poor (score 0–3), moderate (4–6), and excellent (7–9). The mentioned score was based on filters such as case selection, comparability, and outcomes with related analysis. Moreover, various parameters were considered to define scores for each article. Figure 1 illustrates the preferred reporting items for systematic reviews and meta-analyses (PRISMA) flowchart.
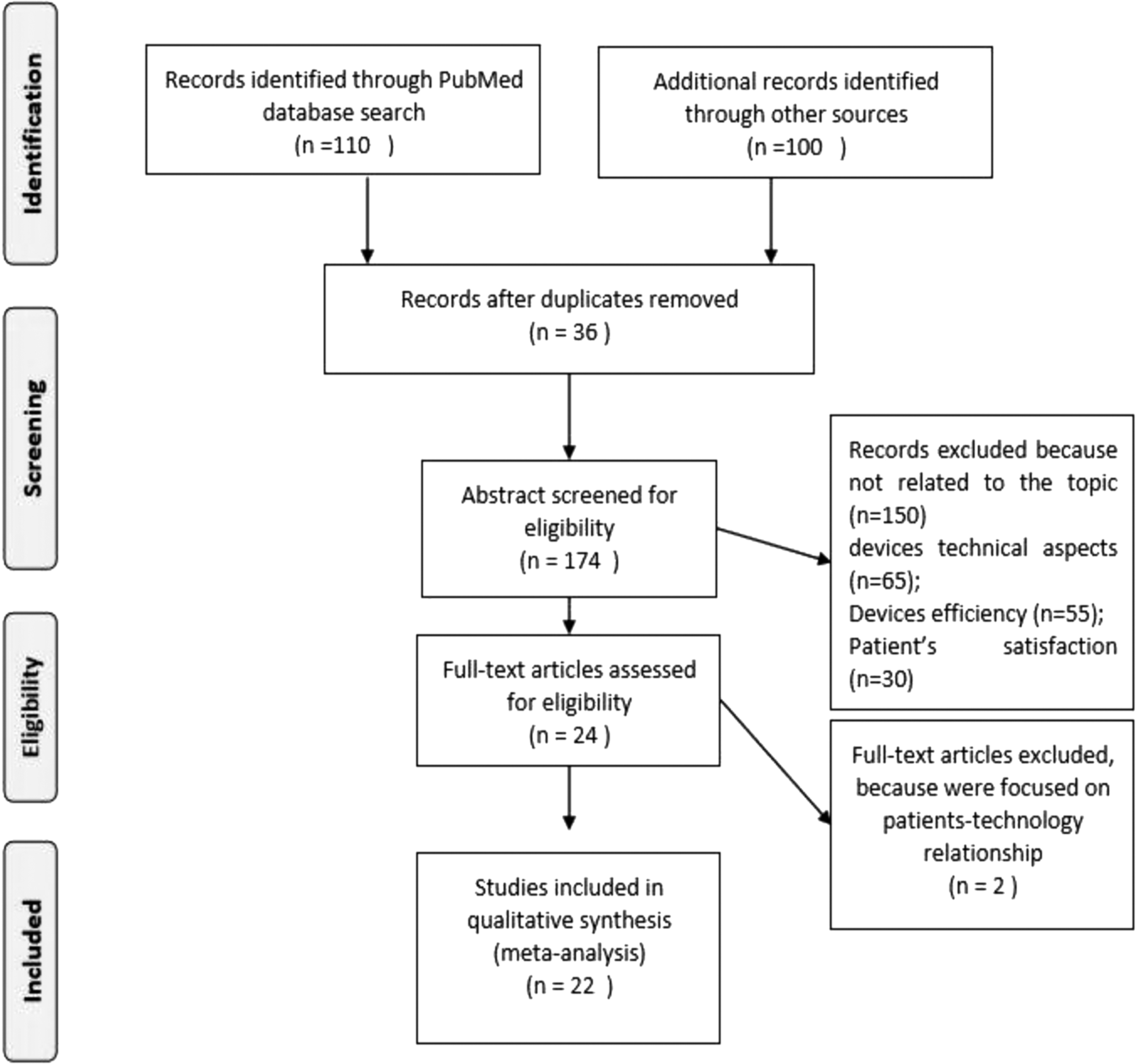
Preferred reporting items for systematic reviews and meta-analyses (PRISMA) flowchart.
Summary of Article Pool
The literature search identified 22 relevant articles within the area of telemedicine as the main interest. The studies were organized into several general categories based on the type of medical specialty.
Of the 22 articles, 2 dealt with telemedicine for nursing, 2 with teleradiology, 4 with telehealth for mental health services, 1 with telemedicine and assistance to sailors at sea, 1 with teleneurology, 1 with geriatric telemedicine, 1 with telemedicine, 1 with teleophthalmology, and 1 with telemedicine and alternative medicines. Eight articles were mainly concerned with the legal and ethical aspects of telemedicine.
It is evident that from the selected papers, multidisciplinary methods are highly recommended in telemedicine and telehealth research. The authors have medical, legal, engineering, and philosophical backgrounds. Table 1 list the studies about ethical and legal challenges while dealing with telemedicine practice, with the studies sorted according to year of publication.
Studies About Ethics and Legal Challenges Dealing with Telemedicine Practice
The studies are sorted according to year of publication.
APNs, advanced practice nurses; HIPs, health informatics professionals.
Results
Telemedicine involves the widespread use of an electronic format for maintaining medical records and documenting diagnoses, prescriptions, and details of follow-up appointments. Today, an electronic medical record can hold more intimate details of an individual than any single document. This magnifies the issues related to patient privacy. Federal laws across states and countries do not uniformly address patient record privacy, therefore legal protections for health information are limited to the states. 11 The added concern of jurisdiction and ownership of data gets further complicated in the use of telemedicine across borders.
Current measures often ignore ethical issues linked to professional conduct and relationships, protection of patient autonomy, patient safety, cultural diversity, and the human value system. 12
Informed Consent
Strong evidence stressing the need for informed consent was documented during the review of the studies. All articles mentioned ethical aspects and/or informed consent. Given the scope of the studies, this was expected. Research that focused more on the hardware of telemedicine did not adequately cover these aspects. 13 –15
On the other hand, the work of medical specialties such as telesurgery and those of a juridical and philosophical nature that consider ethical aspects in a significant way are above all. 16 –20
Thirteen articles expressly talk about informed consent to health services. Kluge 19 refers in his work to the informed consent inserted in the electronic file and places the patient's consent, in contrast to the medical paternalism still present in some societies (Japan and China). His reflection on the fact that the patient must have access to his data is interesting and that telemedicine cannot be just implementation of the technological imperative. Many authors speak of the explicit informed consent in transmitting health images. 17,21,22 The ethical cues in Newton's work 23 are interesting, which speak of social justice in accessing telemedical treatments, the risk that the doctor becomes a “medical-automan,” and remembering that there is always the patient besides the images transmitted.
Comer et al., in their work on parent–child integration in disruptive behavior disorders, provide an informed consent of the whole family. 24 The study by Kotsopoulou et al. is one of the few that expresses that the form of consent could be both written and oral under certain circumstances. 17 Kramer et al. on the other hand, in their article on risk management and malpractice, speak about consent, saying that it must be specific. 25 Ricci et al. state that in special conditions such as medical assistance at sea, respect for ethical principles and informed consent of the patient must be present even in such difficult conditions. 26 Balestra hypothesizes the possibility of requesting informed consent for every telemedical transmission unless it is an emergency situation. 27
Botrugno, in his strictly legal work, focuses on the importance of the explanation that must be clear and unambiguous to obtain consent from the patient. 28 The difference in the purpose of each study impacted the structure, content, and format of the informed consent. The lack of uniformity leads to multiple consents with different approaches exposing the vulnerability and validity in telemedicine services.
Protection of Data and Confidentiality
Protection of data and confidentiality always existed for medical information. However, General Data Protection Regulation (GDPR) has further classified and defined data points for easier understanding of and managing personal data. For maximum protection of data, many authors consider necessary uniform guidelines, similar to the GDPR in force in the European Union. 19,25,28,29
The provider in all articles has a strong responsibility for the use of devices, which must be safe, noninvasive (not to make the patient feel spied 21 upon), and easy to handle. Instead, the doctor must pay utmost attention when transmitting the patient's data to others (e.g., second opinion) and in the data storage. 27 There are many hypotheses for maximum data protection; Legido-Quigley et al. 13 hypothesize the anonymity of online data, other authors the identification by a photo, 15 and others that the transmission should be only with encrypted language.
Maximum protection must be ensured when transmitting data of minors and entire groups of subjects (families). 24 However, the study of Newman et al. 30 mentioned that primordial Australian psychiatric patients preferred to wait longer to have a face-to-face meeting with a health expert rather than having a video conference. One of the articles talks about Big Data, referring to data in the electronic medical record. 31 The strictly juridical aspects concern the violation of secrecy and privacy, resulting in a criminal, civil, and deontological crime. 26
Botrugno asserts that no system is absolutely safe and mentions the peculiarity of genetic data. 28 Only this author speaks of the right to oblivion and cancellation of the data. Most articles mention data protection and privacy, and everyone agrees that the information is sensitive and must be protected. Due to the lack of a universal format, the extent of data protection varies, exposing the structure for misuse.
Physician's Malpractice and Liability
The articles that were extensively reviewed talk about the fundamental rights of the patient and issues concerning medical malpractice. The more the works deal with clinical health specialties (telenursing, teleradiology, telemental, and teleneurology), 13,15,22,25,27,32 the greater is the concern expressed. However, almost all articles fell short of providing insight into the potential outcome in the case of the above. In most cases, the section was summarized by referring it as being purely ethical in nature and not being elaborated in detail. 16,18,20,28,30,31
The discussion on malpractice can be classified into two segments: (1) telemedicine introduces a new form of malpractice 25,32,33 or (2) there is no difference with the normal malpractice with the patient being present. 15,18 Interpretation is left to the imagination of the end user.
Some articles proposed interesting concepts such as training of doctors to avoid “telenegligence.” 21,32 Kluge also proposes a breakdown of doctor–patient responsibility 16 : “Medical interventions are provided, how should they be taken advantage of if you make mistakes in taking readings or if they are bad values, or if they accidentally interfere in the automated measurements or in their transmission?” In addition, Parimbelli et al. 34 expand on the figures involved, talking about all the stakeholders—patients, physicians and nurses, system developers, hardware vendors, and hospital administrators. Many studies indicate (as a solution to the damage) that an extended insurance coverage 14,22,23 or a civil responsibility 22,26 should be derived from the telemedicine implementation in order to protect the careers of health care providers. However, in the balance between risks and benefits, the benefits of teleconsultation 15 seem much greater than the risk of being sued.
Laws and Regulations for Telemedicine
Given the diverse approaches to the various ethical and legal aspects of telehealth, it was much expected that there would be only limited studies talking about laws and regulations. Within those that mentioned it, most seemed to lack constructive information and only further expressed the need for unified legislation. Two major strands can be distinguished: North American works deal mainly with laws governing telemedicine activity between one State and another and the problem of licenses for the exercise of telemedicine. 15,23,25,27,32 The European works instead report the European Directives, their application, and their harmonization. 13,22,28,34 The work of Chiang et al. 14 provided poor knowledge on Taiwan's constitutional laws: “There is no protection from specific regulations and laws; therefore, sometimes, medical practice easily leads to medical disputes, and it is difficult to clarify the attribution of responsibilities.”
In this article, we defined remote regions as areas with limited access to good health care in developing nations or those affected by conflict and refugee populations. The above most often depend on support from nonprofits and basic government initiatives.
However, one of the limiting factors is the sensitivity to local culture as more often care is provided by medical professionals from different geographic and cultural backgrounds. The above raises an important aspect of sensitizing telemedicine professionals and its users on cultural issues. A comparison can be drawn with the airport security at international airports where a lot of efforts have been made to train officers on the ethnic and cultural diversity and appearances of various populations. In health care, it is more profound and complex and would require a sustained effort from all stakeholders. 35
Statistics show that telemedicine if adopted collectively can bring about greater care for individuals, cost savings in the long run, and more importantly a more organized and sustained manner for public health. This despite that health care for all is a long-drawn debate in countries practicing, proposing, or opposing it. 36
However, we believe that with growing adoption of AI in health care, we would be able to expand the scope and results while optimizing the costs of telemedicine.
Conclusions
Telemedicine for patients has been shown to be feasible and well accepted in areas of medical consultation, nursing, teleradiology, psychotherapy, and teleneurology. Some advantages documented in the articles are not only the reduction of distances between the doctor and patient, especially in rural and difficult to reach areas, but also the possibility of having support, be it medical specialist, nursing, or psychological. To increase the adoption of telemedicine globally, standardization of laws for telemedicine is essential.
A critical concern is data privacy. Although the guarantees are high, in the future, maximum protection of patient's data must be ensured. This guarantee must be provided first and foremost not only by those who supply the device but also by all health professionals. The maintenance, use, and replacement of devices (which age in a short time) are objects of concern strongly found in all the analyzed articles.
Another important aspect is the training and professionalism of those who carry out the telemedical activity. Preparation remains the responsibility of universities, training institutions, and individual scientific societies so that they can provide, as soon as possible, integrated health training with telemedicine aspects. This would greatly help the performance of health professional services.
It seems necessary not to underestimate the issue of the absence of legislation. Many works show that the legislation on telemedicine activity is lacking if not completely absent in many cases. The regulatory uncertainty entails further difficulty that adds to the curative activity of telemedicine itself. Many articles refer, for Europe, to the community directives that help in development of telemedicine activities. In the future, it would be desirable to carry out a systematic review in this area to see if greater sensitivity will be shown by legislators around the world.
There are two issues that seem to have entered fully into the telemedical activity and been dealt with due consideration: ethical arguments and costs.
The ethical aspects of telemedicine are sufficiently analyzed in many works, and it seems comforting that all the authors have strongly insisted on protection of patient information, on informed consent, and on the fact that behind the screen there is, however, a suffering person, not making the patient just a number to take care of. Several articles examined the high costs of telemedicine implementation due to automation, security, and legality, etc.
In conclusion, with this work, we want to highlight the importance of telemedicine activity in all its health, curative, relief, and consultation areas. Although aspects that are not well developed or with obvious shortcomings still exist, we can safely say that the use of telemedicine overcomes every organizational and practical deficit that may exist. The purpose of the analysis of the literature is preventive; in fact, if the highlighted aspects are not corrected, we could envisage a boomerang effect of telemedicine. From a great system of utility for health activity, it would become a source of professional responsibility, with the risk of increasing claims for damages and malpractice that would not help such a useful and vital activity for the patient.
Footnotes
Acknowledgment
The authors thank Professor Fabio Esposito for providing language help and having reviewed the English grammar.
Author Contributions
G.N. made a substantial contribution to conception and design of the study; he has analyzed and revised the data; he prepared the draft of the manuscript and revised it critically; and he has given final approval of the version to be published. R.K. made a substantial contribution to conception and design of the study; he has analyzed and revised the data; he prepared the draft of manuscript and revised it critically; and he has given final approval of the version to be published. S.B. carried out the acquisition of data or analysis of data and he has given final approval of the version to be published. G.P. carried out the acquisition of data or analysis of data and he has given final approval of the version to be published. G.B. carried out the acquisition of data or analysis of data and he has given final approval of the version to be published. A.S. made a substantial contribution to conception and design of the study; he has performed the analysis and interpretation of medical data; and he has given final approval of the version to be published. A.F. made a substantial contribution to conception and design of the study; he has performed the analysis and interpretation of medical data; and he has given final approval of the version to be published. G.R. made a substantial contribution to conception and design of the study; she has performed the analysis and interpretation of ethical and legal aspects; and she has given final approval of the version to be published.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.