
Abstract
Introduction
For many individuals with chronic disease, optimal self-management is difficult to achieve. Consequently, there has been an increased interest in self-management programs, an important component of the Chronic Care Model. 1 One of the most widely implemented is the chronic disease self-management program (CDSMP), an in-person, peer-led health education program delivered in six weekly 2-h sessions by trained program leaders, developed and validated by the Stanford Patient Education Research Center. 2 Several randomized controlled trials have shown the CDSMP to be effective in increasing self-efficacy, which in turn has been related to improving health status and health behaviors. 3 –13
CDSMPs have an important role in rural and remote areas with limited access to and availability of healthcare and community-based services but have been rarely evaluated in this setting. 14,15 Delivery of the CDSMP via telehealth 16 would address three important barriers: the need for program leaders in every community; the need for leaders to travel long distances to communities, particularly remote areas without leaders; and the need for a sufficient number of participants to form a face-to-face group in each community. Prior research on the CDSMP has not evaluated a telehealth delivery model, nor have there been any published studies on a Canadian population.
We hypothesized that telehealth would enable a small number of trained program leaders (not from the same communities as participants) to link to self-management groups across several rural and remote communities in Canada. Two configurations of telehealth delivery—single site and multiple sites—were examined. At a single site, program leaders from one community (leader site) were linked via telehealth to participants from another community who formed a self-management group. In multiple sites, participants from several remote communities were linked to each other to form a self-management group and to a leader site via telehealth (Fig. 1). The main objectives of this study were to examine whether access to a telehealth self-management program in rural and remote communities for individuals with chronic diseases (telehealth CDSMP [tele-CDSMP]) improves self-efficacy, health behaviors, and health status and whether there are differences in outcomes between the two delivery models (single site and multiple site).
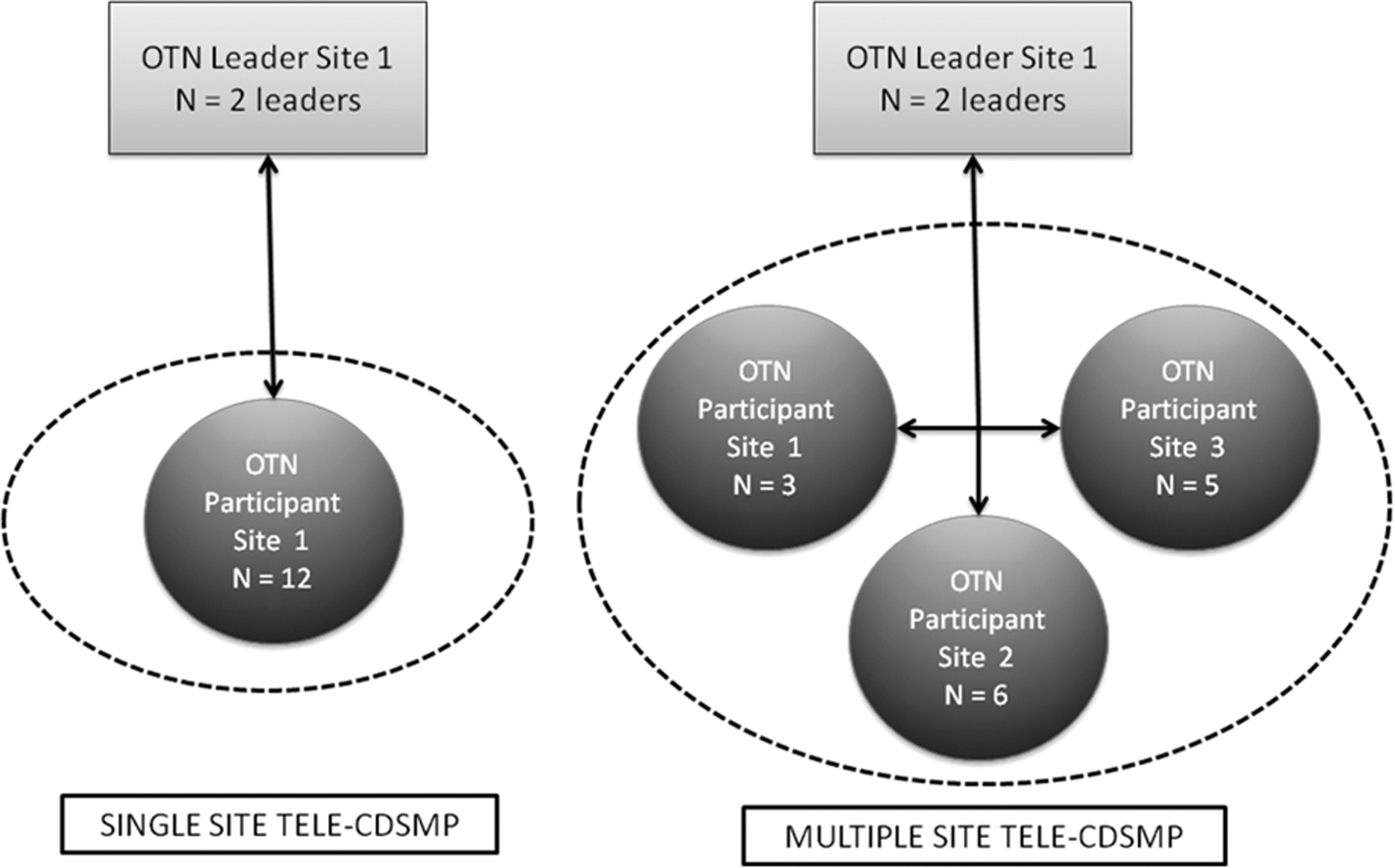
Example of single- and multi-site program delivery. CDSMP, chronic disease self-management program; OTN, Ontario Telemedicine Network.
Subjects and Methods
Study Design
A randomized controlled trial design was considered as an option with patients randomized to either single-site or multiple-site telehealth groups. However, it would not have been logistically possible to include patients in the trial who were from very remote and rural communities. The ideal group size for the chosen self-management intervention is 10–15 participants. 8 It is expected that in smaller communities there would not be sufficient numbers of individuals to make up a self-management program group because of population size. Therefore a trial would be limited to the larger communities and would not be generalizable to the communities that the intervention is expected to benefit. The more pragmatic two-group pre–post comparison design was chosen to examine delivering CDSMP in the context of the “real-world” setting in rural and remote communities using existing telehealth linkages. This study was approved by the Research Ethics Board at Women's College Hospital, Toronto, ON, Canada.
Setting
Ontario is the most populous province in Canada with approximately 13 million inhabitants and one of the largest in terms of geographic size. All communities in Northern Ontario who were part of the Ontario Telemedicine Network (OTN) 17 were eligible. Leader sites were designated as communities with population sizes >40,000, and participant sites were those with <20,000 inhabitants. Five leader and 13 participant sites were enrolled, with the latter ranging in population from approximately 1,400 to 18,000 inhabitants and 7 sites having populations of less than 5,000.
Leaders
Sixteen leaders were recruited (minimum of three per community) from disease-specific associations, hospitals, community groups (e.g., church groups, retired teachers associations), and OTN member sites. Consistent with CDSMP delivery, at least two of the three leaders per team had one of the chronic diseases targeted in this study, and the other was either a healthcare professional or other professional (e.g., teacher).
Participants
Participant recruitment was coordinated by the central study office. Internet searches were used to develop a community profile for each participant site, including contact information for each health and community-based organization. A research coordinator initiated community relationships by phoning individual organizations and sending brochures to raise their awareness about the program and ask them to promote the program to their clientele. A 1-800 number was provided to enable interested individuals to contact the study coordinators directly.
To be eligible for the CDSMP, participants had to have a self-reported physician diagnosis of chronic lung disease (asthma, chronic bronchitis, or chronic obstructive pulmonary disease/emphysema), heart disease (coronary artery disease or congestive heart failure), stroke, or chronic arthritis. Individuals with diabetes and hypertension were included if they also had one of the above diagnoses. Participants had to speak and read English and be able to attend a 2-h session, once a week for 6 weeks. Individuals younger than 45 years of age or who had received chemotherapy or radiation within the past year were excluded. Participants were allocated to either single-site or multi-site groups based on the number of interested participants in their community.
Description of Tele-CDSMP
The tele-CDSMP used the same training and content as the CDSMP (Table 1 gives the program description). 2 Leaders attended the standardized 4-day CDSMP training program delivered by two certified CDSMP Master Trainers, in addition to a 2-h training session on telehealth etiquette and use of equipment. Prior to running the courses, a booster telehealth training session was held to review procedures and to conduct a practice teaching session. The telehealth studios used in this study were already established in hospitals that were part of OTN and normally used for clinical consultations. Studio time was blocked for 2.5 h for 6 consecutive weeks on days and times with low use for clinical consultations. Each studio had a U-shaped table where participants sat, monitors, and cameras with videoconferencing capabilities. An OTN telehealth coordinator was present at each tele-CDSMP session to manage the technology, which is standard practice. No modifications were made to the content of the CDSMP, but preprinted handouts instead of flip charts and a seating plan rather than name tags were provided because of the monitors. As a patient education program, the tele-CDSMP is offered in the format of a guided workshop rather than a traditional lecture format, where program leaders and participants from different sites are in constant interaction, with ample room for sharing of experiences and teaching of practical skills to increase confidence and motivation to manage the challenges of living with chronic health conditions. In both the single- and the multi-site configurations, participants and leaders could communicate live with each other with both video and sound and therefore see and hear who in the group was speaking on their monitors. For the multi-site configuration, three nodes per leader group was the optimal configuration as an increased number of sites meant smaller-sized visuals on the monitor/screen for participants to see each another.
Overview of Telehealth Chronic Disease Self-Management Program Program Content
Outcome Measures
Three main outcomes were evaluated: self-efficacy, health behavior, and health status. To compare outcomes between the telehealth delivery models and already published evaluations of the CDSMP, the recommended measures developed and validated for the CDSMP were used. 2 Baseline data were collected within 2 weeks of the course start date, and data at 4 months were collected after the last session by telephone survey.
Self-Efficacy
This study used a six-item self-efficacy scale that was previously tested on 605 participants with chronic disease. 5 Participants rated their confidence on a scale of 1–10, with “1” being not at all confident to “10” being totally confident. The first four items were confidence in keeping fatigue, physical discomfort and pain, emotional distress, and other symptoms or health problems from interfering with activities. The fifth item was confidence in doing different tasks and activities needed to manage the condition, and the sixth was confidence in doing things other than taking medication to reduce how much your illness affects your everyday life. The summary score is a mean of the six item-level scores.
Health Behaviors and Health Status
Four health-related behaviors were measured: stretching and strengthening exercise, aerobic exercise, use of cognitive symptom management techniques, and use of techniques to improve communication with physicians. 2 There were seven health status measures: the Stanford disability scale, an adapted social role limitations and mental health index from the Medical Outcomes Studies, 18 and visual numeric scales for pain/physical discomfort, psychological well-being, energy/fatigue, health distress, and self-rated health status. 2 Age, sex, disease condition(s), marital status, employment status, income level, education level, and community name were collected at baseline for all participants.
Data Analyses
The analyses focused on evaluating changes in self-efficacy, health behaviors, and health status variables from baseline to 4 months after the tele-CDSMP for all participants using paired t tests if the assumption for normality was verified; otherwise the Wilcoxon signed-rank test for non-parametric distributions was used. Differences in baseline characteristics were examined using t tests for the continuous variables (age and total number of chronic conditions) and chi-squared analyses and Fisher's exact tests for the binary and categorical variables (sex, type of chronic condition, marital status, and education and income levels). To determine whether the two telehealth delivery models (single-site versus multi-site telehealth groups) differed with respect to changes in self-efficacy, health behaviors, and health status variables from baseline to 4 months, a series of analysis of covariance models while adjusting for age, sex, and education level, as well as the total number of chronic conditions reported by the participant, were conducted. Data were analyzed using SPSS version 19 software (SPSS, Inc., Chicago, IL). All tests were two-tailed, and we considered p values of <0.05 to be statistically significant.
Results
Program Attendance
Two hundred thirteen participants were enrolled in 19 tele-CDSMP courses between September 2007 and June 2008. One hundred four were enrolled in a single-site tele-CDSMP course, and 109 were enrolled in a multi-site tele-CDSMP course. In total, 71 (31.5%) participants attended all sessions, 158 (70.2%) attended four or more sessions, and 20 (8.9%) dropped out of the program. Of the enrolled participants, 186 (87%) completed the 4-month follow-up telephone questionnaires.
Participant Characteristics
Demographic information of all enrolled participants is provided in Table 2. Participants were mostly female (74.2%), of European descent (89.7%), and between the ages of 45 and 88 years (median age, 67 years). About half of respondents were married (50.2%), with an average household income within the range of $20,000–40,000. The median level of education achieved was the completion of high school. Participants reported an average of 2.6±1.2 chronic conditions. The multi-site tele-CDSMP groups had significantly more female participants than the single-site groups (p<0.001).
Demographic Information and Distribution of Chronic Diseases Among Enrolled Program Participants
Comparison of Baseline and 4-Month Outcomes
Participating in the tele-CDSMP was associated with significant improvements in self-efficacy and each of the health behaviors, including stretching and strengthening exercises, aerobic exercise, cognitive symptom management, and communication with physicians (Table 3). For health status, statistically significant improvements in social role function, psychological well-being, energy, and self-reported health and a significant decline in health distress 4 months after completing the tele-CDSMP were observed, with no significant changes in pain or disability.
Program Outcomes for Participants at Baseline and at 4-Month Follow-Up and Change Scores
The P value corresponds to the significance level for the paired t tests and Wilcoxon signed-rank tests performed on all variables between baseline and 4 months.
Comparisons between Single- and Multi-Site Tele-CDSMP Groups
There were no statistically significant differences in the change scores for self-efficacy, health behaviors, and health status variables between participants in the single-site tele-CDSMP and the multi-site tele-CDSMP groups from baseline to 4-month follow-up, after adjusting for covariates (Table 4). Greater changes in self-rated health for those in the multi-site tele-CDSMP groups than for those in the single-site tele-CDSMP groups (p=0.05) were noted.
Mean Change in Self-Efficacy, Health Behaviors, and Health Status Scores from Baseline to 4 Months for Participants Enrolled in the Single- Versus Multiple-Site Telehealth Chronic Disease Self-Management Program
The P value corresponds to the significance level for the analysis of covariance models estimated for all change scores (difference between variables at 4 months and baseline), with age, sex, education level, and total number of chronic conditions as covariates.
SD, standard deviation.
Discussion
The findings of this study indicate that using telehealth to deliver the Stanford CDSMP to participants in rural and remote areas improves their self-efficacy in managing their condition, promotes positive health behaviors, and increases health status 4 months after participating in the program. More important is that we also found no differences in outcomes between the single- and the multi-site groups with the exception of self-rated health, which improved more in the multi-site groups. Our findings suggest that this model could be used to connect several virtual groups to the same lay leader.
Fourteen studies, conducted in various countries (six in the United States, three in the United Kingdom, and one each in China, Hong Kong, Japan, Australia, and The Netherlands) have evaluated the CDSMP compared with a control group using self-efficacy as an outcome. 3,4,7,9 –13,19 –24 Only three studies evaluated variants of the in-person CDSMP, the Internet version and its update, the Expert Patients Programme (EPP) online, 8,19 and Homing in on Health (HIOH), 13 which is delivered one-on-one in homes or by telephone for 6 weeks. The purpose of HIOH was to make the CDSMP available to those unable to participate in group settings, those with functional limitations, transportation problems, and/or discomfort with groups.
Similar to the current study, 11 of the 14 in-person studies evaluating the CDSMP had 70% or more women participating. The distribution of diseases varied across the studies, but the majority had some combination of participants with arthritis, heart disease, lung disease, and diabetes and similar age distributions. The attendance rate (74%) in our study was similar to that seen in other studies where the majority of participants attended at least half the sessions. We did find a significant effect of the tele-CDSMP on illness management self-efficacy after the intervention with a change score comparable to that in other CDSMP studies, suggesting successful implementation of the intervention. Of the nine studies evaluating self-efficacy, 3,7,10,11,13,21 –23,25 all but one found a statistically significant improvement following participation in the CDSMP. Eleven 3,4,7,9 –11,13,19,23,24,26 of the 14 studies reported on exercise behavior, and in all but one study, aerobic exercise behavior significantly increased. The findings for the other health behaviors (cognitive symptom management and communication with healthcare providers) and health status measures have been mixed. Possible explanations for the differences in findings or inconsistent effects across studies include variability in the characteristics of the populations studied, program implementation, or chance effects due multiple outcomes testing. Effects also differ among the CDSMP variants, the EPP online, and the HIOH. For the EPP online 19 and the HIOH one-on-one home visits, 13,27 improvements were similar to those seen with the in-person program, whereas no significant effects were observed for the HIOH delivered by telephone. A possible explanation may be that face-to-face peer interaction, like that of the tele-CDSMP, may produce a more powerful therapeutic alliance than is possible by telephone. This does not explain the positive effects for the online program, which had no face-to-face interaction. It should be noted that the EPP online recruited those with an interest in online learning and allowed for virtual support through an e-mail buddy system and bulletin board discussion groups, which may explain why they did not need face-to-face interaction. 8,28
Although this is one of the few studies of the CDSMP in a rural setting, 15 it had several limitations. First, it was not a randomized trial, and this was intentional, given the study setting. The purpose was to increase access to small communities that would not have the capacity to conduct the standard CDSMP. Multi-site communities did not have the capacity to be randomized to single-site delivery. Second, the possibility cannot be ruled out that those who did not benefit from the course were more likely than those who benefitted to have dropped out. Thus, the results apply most strongly to those willing to participate in a program and complete questionnaires after participation. Another limitation is that the outcomes were measured at 4 months and not longer term to establish sustainability.
In conclusion, the tele-CDSMP adds to the research on CDSMP variants and is one of the first studies on a Canadian population. It is also one of the first studies reported in the literature to deliver the CDSMP via telehealth. The findings indicate that using telehealth to deliver the Stanford CDSMP to participants in rural and remote areas in Canada results in significant improvements in self-efficacy, health behaviors, and health status that are comparable to the traditional in-person program. With the exception of self-rated health, which improved more in the multi-site groups, no differences were found in outcomes between the single- and the multi-site groups, suggesting that a virtual group connected to the same lay leader is equally effective. Unlike the Internet-based intervention, it is not limited to those who can read. Like the EPP online, the tele-CDSMP should not be viewed as a replacement for the traditional CDSMP but rather as an additional means of reaching populations with limited access to community-based programs.
Footnotes
Acknowledgments
We would like to acknowledge the funding support provided by the Canadian Institutes of Health Research (funding reference number MOP 81099) and our partnership with the Ontario Telemedicine Network and its member sites. S.B.J. is the Toronto Rehabilitation Institute Chair at the University of Toronto. N.M.S. was supported in part by a Canadian Institutes of Health Research postdoctoral fellowship and in part by a Heart and Stroke Foundation of Ontario Clinician Scientist Award to conduct this research. G.H. is the F.M. Hill Chair in Academic Women's Medicine, Women's College Hospital, University of Toronto. W.L. is a Canada Research Chair in Statistics at the University of Toronto. P.K. is a Canadian Institutes of Health Research New Investigator.
Disclosure Statement
No competing financial interests exist.