
Abstract
Objectives:
Over the last decades, there has been a significant increase in antimicrobial prescribing and consumption associated with the development of patients' adverse events and antimicrobial resistance (AMR) to the point of becoming a global priority. This study aims at evaluating antibiotic prescribing during COVID-19 pandemic from November 2019 to December 2020.
Materials and Methods:
A systematic review was conducted primarily through the NCBI database, using PRISMA guidelines to identify relevant literature for the period between November 1, 2019 and December 19, 2020, using the keywords: COVID-19 OR SARS-Cov-2 AND antibiotics restricted to the English language excluding nonclinical articles. Five hundred twenty-seven titles were identified; all articles fulfilling the study criteria were included, 133 through the NCBI, and 8 through Google Scholar with a combined total of 141 studies. The patient's spectrum included all ages from neonates to elderly with all associated comorbidities, including immune suppression.
Results:
Of 28,093 patients included in the combined studies, 58.7% received antibiotics (16,490/28,093), ranging from 1.3% to 100% coverage. Antibiotics coverage was less in children (57%) than in adults with comorbidities (75%). Broad-spectrum antibiotics were prescribed presumptively without pathogen identifications, which might contribute to adverse outcomes.
Conclusions:
During the COVID-19 pandemic, there has been a significant and wide range of antibiotic prescribing in patients affected by the disease, particularly in adults with underlying comorbidities, despite the paucity of evidence of associated bacterial infections. The current practice might increase patients' immediate and long-term risks of adverse events, susceptibility to secondary infections as well as aggravating AMR.
Introduction
The discovery of antibiotics in the middle of the 20th century was a significant breakthrough for humanity saving millions of lives and preventing significant morbidity and mortality associated with infectious diseases. 1 A decade after the historical discovery, a noticeable antimicrobial resistance (AMR) was observed escalating to an alarming scale over recent years. 2 It has been estimated that about 700,000 annual global mortality is attributed to AMR, which attracted the attention of world leaders and international organizations such as the World Health Organization (WHO) all advocating regional and global initiatives to contain the problem. 3 Antimicrobial Stewardship Programs (ASPs) have been implemented in many health care settings worldwide to curtail inappropriate and excessive antibiotic prescribing, particularly for broad-spectrum antibiotics. 4 At the end of 2019, the world witnessed a worrying herald of a global pandemic caused by a novel coronavirus coined SAR-CoV-2 leading to the clinical syndrome of COVID-19 disease. 5 Although the disease causes a respiratory illness primarily, it was noticed from the beginning it is associated with significant secondary presentations, including multisystem complications in need of critical care, particularly for server disease. Since there was no available effective management, antibiotics were frequently prescribed for various rationales with the potential of contributing to AMR. 6 Although COVID-19 principally is a viral infection not usually responding to antibiotics, it is capable of causing an acute respiratory disease indistinguishable from bacterial infections and creating an environment and complications favoring secondary bacterial infections. 7 For such reasons, health care professionals were confounded to prescribe antibiotics to treat potential bacterial infections or secondary complications. To comprehend the scale of the problem, a study conducted by the WHO demonstrated that 72% of COVID-19 patients received antibiotics. Nevertheless, only 8% had evidence of documented superimposed bacterial infections. 8
To add to the complexity of the situation, unverified research at the start of the pandemic advocated combined management with chloroquine/hydroxychloroquine together with the macrolide antibiotic azithromycin led to hasty inclusion in many COVID-19 management guidelines across the globe before establishing better-evaluated efficacy. 9 Even for patients who warrant treatment during the pandemic, Getahun et al. 8 indicated that antimicrobials were overprescribed for patients admitted to intensive care units (ICUs) in 88 countries where 70% of patients received antibiotics. However, only 54% of patients had suspected or proven bacterial infections. Because of the gravity of the situation, confusion of the optimal management approaches for the novel disease together with the stretching of physical limits and capabilities of health care ASPs; the COVID-19 pandemic created an environment for inappropriate and excessive antibiotic prescribing, which might worsen future AMR through selective pressures. The presented literature review is conducted to examine and highlight the spectrum of antimicrobial prescribing during the COVID-19 pandemic to raise awareness toward potential consequences.
Materials and Methods
A literature search was conducted using the PRISMA guidelines for systematic reviews. 172 The NCBI database was identified as a primary source of related literature because of clinical relevance between November 2019 and December 19, 2020. Adopted search keywords were COVID-19 OR Sars-Cov-2 AND antibiotics restricted to the English language. The search initially resulted in 527 identified titles eventually limited to 133 following applying restrictive criteria. An additional 8 articles were included following searching Google Scholar search engine, bringing the total number to 141 studies. As per the study protocol, only articles covering clinical settings were included, articles limited to basic science, solely microbiological characteristics, experiments, surveys, guidelines, and hypotheses. Those not providing details of antibiotic prescribing were excluded (n = 386) (Fig. 1). The information extracted from the included articles comprises types of antibiotics prescribed for COVID-19 patients and the number of those patients, bacterial coinfection, and relevant patient demographic data (age, gender, and country). In addition, if the COVID-19 patient is suffering from any other complications such as hypertension, cardiac disease, diabetes, pregnancy, cancer, and human immunodeficiency virus (HIV) were reported.
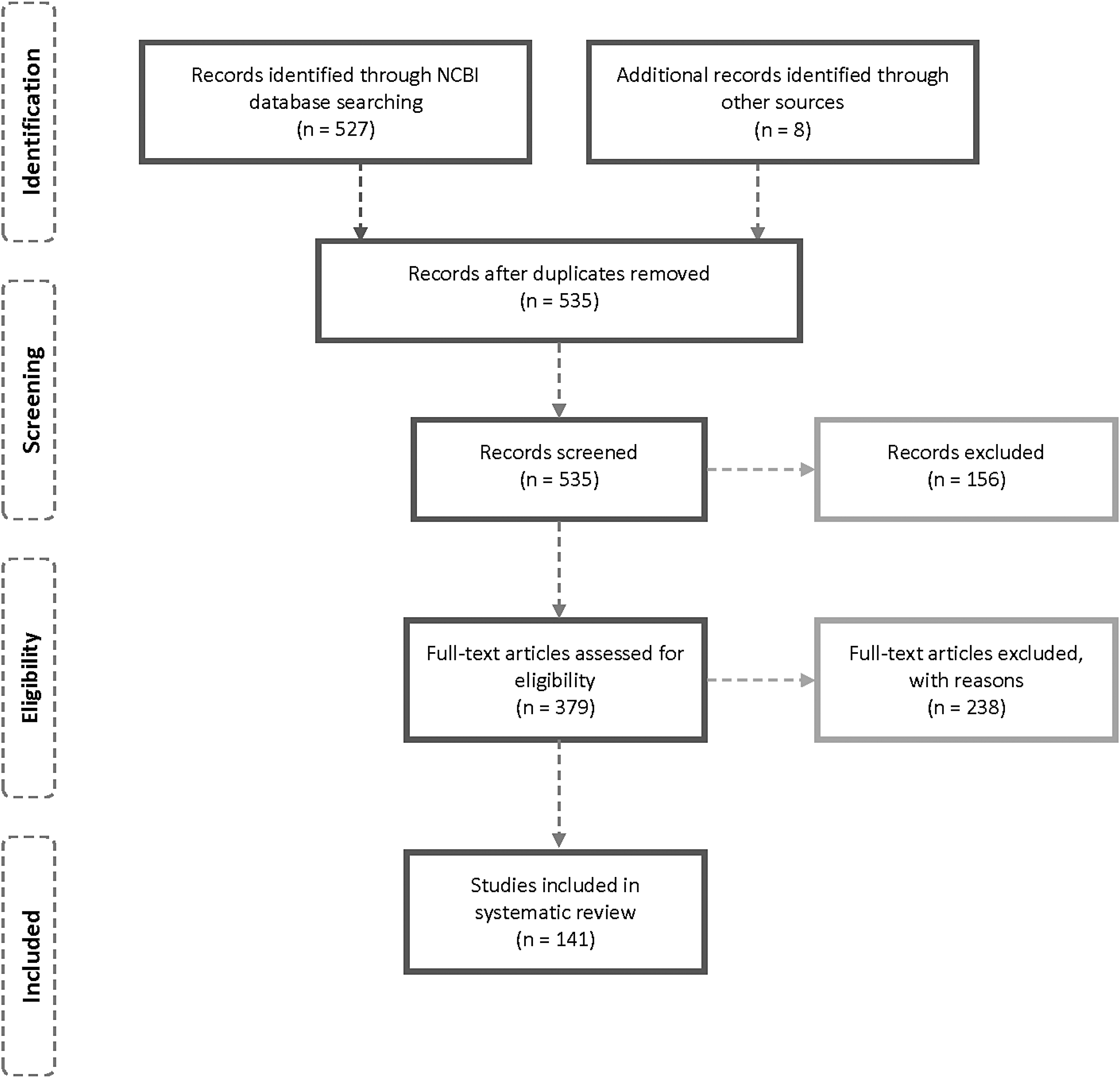
Schematic selection process of included studies.
Results
One hundred forty-one articles were included in this review from 28 different countries. The majority of them are from countries worst affected by the pandemic: China (n = 55), followed by the USA (n = 18), Italy (n = 10), UK (n = 5), Spain (n = 5), Brazil (n = 4), Iran (n = 4), and India (n = 3). Two articles were incorporated from Belgium, Germany, Japan, South Korea, Netherlands, and Saudi Arabia and one from Bhutan, Colombia, France, Ireland, Morocco, Niger, Oman, Philippines, Qatar, Singapore, Switzerland, Taiwan, and Uganda. Fourteen articles were included with no identified country (Table 1).
Showing Affected Countries, the Total Number of Patients, Number and Percentage of Patients Prescribed Antibiotics, Gender, Age, Prescribed Antibiotics, and Comorbidities
CKD, chronic kidney disease; CLD, chronic liver disease; COPD, chronic obstructive pulmonary disease; CVD, cardiovascular disease; DM, diabetes mellitus; HIV, human immunodeficiency virus; HT, hypertension.
The study population's demographic and clinical characteristics included all ages from neonates, children, and adults, including pregnant women and the elderly. Associated underlying conditions included hypertension, diabetes mellitus, heart, respiratory, renal, liver, thyroid, cerebrovascular, rheumatic diseases, and HIV and organ transplantation (heart, lung, kidney, liver, and bone marrow). Of 28,093 patients included in the combined studies, 58.7% received antibiotics (16,490/28,093). The percentage of patients prescribed antibiotics in each article differs, ranging from 1.3% to 100% coverage, with only 9.9% of the articles reporting less than 50% antibiotic covering (14/141). Most included articles did not present clear data on an antibiotic prescription for patients with other complications versus those without comorbidities. Comparing the articles that include the population who suffered from other diseases to those with no other complications, we found that antibiotic coverage did not differ significantly between patients with and without comorbidities (75.2%, 415/552), and 71% (8,449/11,886), respectively (Fig. 2).
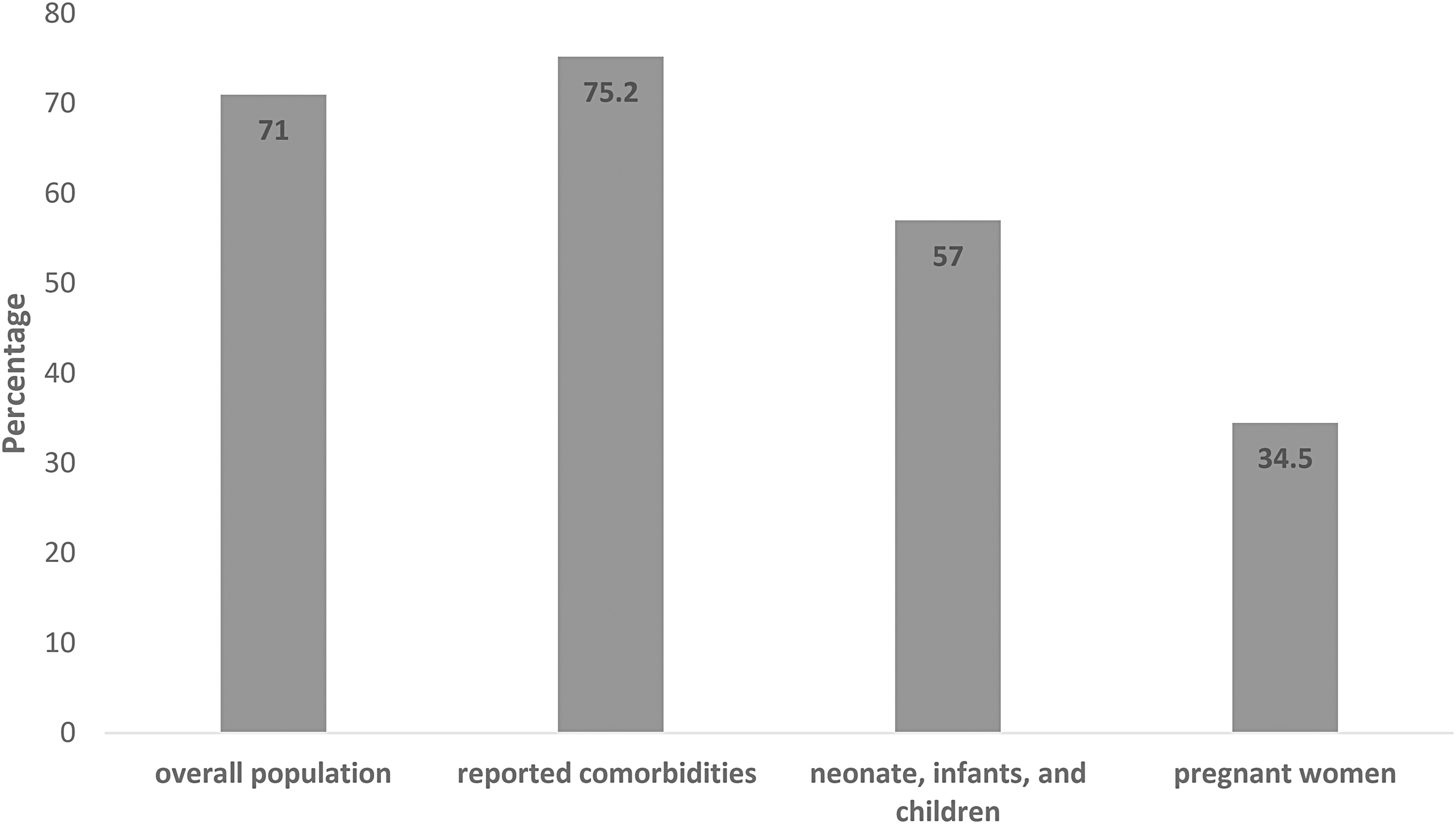
Comparison of percentage antibiotic prescription in studied population compared to patients with reported comorbidities, children, and pregnant women.
Antibiotics coverage was less in children, 57% (187/329) compared to adults, and it was least in pregnant women (34.5%, 29/84). Despite the high percentage of antibiotic prescribing, most articles did not report bacterial coinfection (75.36%), indicating that probably a significant amount of antibiotics were empirically and unnecessarily prescribed.
The spectrum of antimicrobial prescreening is broad since more than 40 different antimicrobials were used to manage patients with COVID-19 disease (Table 2).
Showing the Number of Articles Reporting Each Antibiotic
Inferring from the number of articles reporting the use of specific antibiotics, cephalosporins followed by azithromycin and moxifloxacin were the predominant oral antibiotics while piperacillin/tazobactam was the prevalent parenteral antibiotic. However, when subdividing cephalosporins into distinct classes based on their generation (first vs. second vs. third vs. fourth), azithromycin becomes the predominant antibiotic reported, which reflects its prominent role during the pandemic. Nevertheless, most studies highlighted that the majority of antibiotics were prescribed empirically as prophylaxis to prevent secondary bacterial infection, 70 to treat secondary bacterial infection such as pneumonia, 59 or as potential COVID-19 treatment agents. 53 Other described drugs reported include meropenem, levofloxacin, linezolid, vancomycin, amoxicillin/clavulanate, Teicoplanin, and carbapenem.
Discussion
The excessive and inappropriate prescribing of antibiotics is a significant challenge for health care across the globe. The escalating problem has been directly associated with detrimental patients' safety through the development of direct adverse events, indirect acquisition of secondary health care-associated infections, propagation of AMR, worsening infection control and prevention measures, as well as substantial cost implications.148,149 Of all infectious diseases, respiratory infections are the leading cause of inappropriate antibiotic prescribing and overuse. The majority of upper respiratory tract infections are caused by viruses, and only less than 10% are caused by bacteria 150 ; nevertheless, the WHO reported that in 2016, 71% of patients with UTRIs had been prescribed antibiotics. 151
The COVID-19 pandemic caught all health care settings across the globe by surprise; the novel SARS-CoV-2 virus caused an unprecedented universal health scare since there was little preceding knowledge about the disease and its implications, particularly potential secondary infections. Furthermore, the disease presents primarily as a respiratory illness mimicking bacterial infections hence confounding clinical assessment; conversely, critical patients need invasive procedures often associated with secondary health care-associated infections. To add the disease complexity, unverified early clinical reports and trials advocated using antibiotics to hinder disease progression and hasten viral clearance, despite the discouragement of such an approach by international guidelines. 8 Consequent to all these factors, antibiotic prescribing was noticeably frequent in patients with COVID-19 disease.
Our search encompassed about 28,000 patients from 28 different countries, to evaluate the problem systematically, the majority of which were severely affected by the pandemic, such as China, Iran, Italy, Spain, UK, and the USA, demonstrated widespread practice of prescribing antibiotics particularly in adults underlying clinical with conditions. The overall percentage of cases prescribed antimicrobial therapy is evident in 58.7% of cases being more common with premorbid or immune-compromised conditions (Fig. 1). Several authors reported treatment strategies for COVID-19 patients incorporating empirical antibiotic treatment.14,30,37,58,152 Such observations are in line with early pandemic epidemiological reports since it was apparent that more severe and critical disease is predominant in the elderly and those with underlying premorbid conditions such as diabetes, heart failure, and the immune-compromised. Conversely, severity markers included acute kidney and liver injuries, explaining antibiotic prescribing prevalence in such populations.
It is worth noticing; prescribed antibiotics are not necessarily to cover documented secondary bacterial infections since, in many studies, the presence of bacterial coinfection or secondary infection is much lower than the number of patients prescribed antimicrobial therapy. In their review, Lai et al. 153 reviewed 13 papers for the presence of bacterial coinfection or secondary infection, 5 of which reported 0% bacterial coinfection or secondary infection. In contrast, three reported a low percentage of 1%, 3.4%, and 4.8%, respectively. Similarly, a large-scale study from New York described 5,700 patients with only 3 secondary bacterial infections. 154 On the contrary, this in contrast with Italy's study, where 17.2% of patients had bacterial pneumonia and 37% suffered from secondary bacteremia. 155 Lansbury et al. covered 30 studies and 3,834 patients, demonstrating only 7% of the hospitalized patients infected with COVID-19 had a bacterial coinfection. 156 Understandably, the presence of bacterial coinfection was highest in ICU patients (14%) compared to patients in mixed wards (4%). A third review reported 8% of bacterial or fungal coinfection. 7
The reviewed evidence supports the discrepancy between inappropriate and excessive antibiotic prescribing in patients with COVID-19 disease and the presence of bacterial coinfections. Nevertheless, Chien-Yi Chang and Kok-Gan Chan argue that the low rate of coinfection could result from prescribing antibiotics on a large scale to avoid overwhelming health systems during the early pandemic. 157 Furthermore, some have argued that the lack of clear antimicrobial stewardship guidance for the frontline clinician at the early stages of the pandemic probably resulted in an inclination toward antimicrobial prescribing, especially in the early stages of the pandemic. In addition, Lansbury et al.'s 156 analysis shows that more than 90% of the patients in 10 out of 17 studies, in which patients were prescribed antibiotics, received the antimicrobial therapy empirically. It is also worth mentioning that in patients with moderate and severe symptoms, those who received antibiotics or corticosteroids had more extended hospital stays than those who did not. 17
It is worth noting that the high percentage of antibiotic prescribing in patients with no comorbidities (71%) could be confounded by not reporting them in some of the articles, which does not equate to their absence. It is quite possible that an undetermined percentage of patients in such studies suffer from comorbidities. The review also demonstrated lower antibiotic prescribing patterns in the pediatrics population; from 329 neonates, infants, and children included in the review, only 187 (57%) were prescribed antimicrobial therapy. This is a lower rate but might also be appropriate since coinfection is expected in the pediatric population since two studies reported 40% and 51.3% coinfection rates, respectively.158,159 This indicates that the pediatric population might have been better managed during the pandemic from the ASP point of view. Pregnant women were the least to be prescribed antimicrobial therapy, with only 34.5%, which might be due to fears of prescribing antimicrobials during pregnancy rather than its liberal use when compared to a similar cohort, however, we are not sure of the reason for this lower rate in antimicrobial prescription in pregnant women.
The macrolide antibiotic azithromycin was the predominant antimicrobial agents reported in the management of COVID-19 disease (Table 2). Most possible, it was used for its claimed anti-inflammatory effect. 160 Before the start of the pandemic, it was used mostly to treat community-acquired pneumonia as well as exacerbations of chronic obstructive pulmonary disease. 161 Azithromycin's role has been recognized by previous reports of efficacy against other RNA viruses such as Zika and Ebola virus disease162–164 and has been speared when suggested as an adjunct to hydroxychloroquine leading to rapid viral clearance in COVID-19 patients through unclear mechanisms. 9 This probably reflects the highlighted issue with the drug in the foremost pandemic history. 160 Although some limited reports support improved outcomes with adjunctive macrolides in the treatment of COVID-19 disease stemming from previous observations of moderate-to-severe acute respiratory distress syndrome, this has not been materialized in COVID-19 clinical trials. 165 Furthermore, both hydroxychloroquine/chloroquine and azithromycin have been associated with cardiotoxicity by prolonging the QT intervals (the time it takes for the ventricles of the heart to contract and relax), which might precipitate arrhythmias in susceptible patients, particularly those with cardiac diseases, the impact of which is yet to be thoroughly evaluated. 166 The widely used antibiotic azithromycin was gradually recognized as a rare cause of prolonged QT, severe arrhythmia, and increased risk of sudden death.167–170 Beović et al. 171 reported that broad-spectrum antibiotic use in patients with COVID-19 is widespread, according to his survey study administered across 82 hospitals in 23 countries. Importantly, different broad-spectrum antibiotics have been frequently prescribed, including piperacillin/tazobactam, meropenem, vancomycin, and teicoplanin, highlighting potential further development of current or future AMR. More than half of the respondents reported combined use of β-lactams and macrolides or fluoroquinolones, and the most commonly prescribed antibiotic in the COVID-19 ICU was piperacillin/tazobactam. 171 Worryingly, most broad-spectrum antibiotics have been prescribed empirically as prophylaxis to prevent secondary bacterial infection, 70 or to treat bacterial secondary infection and pneumonia, 59 or as part of COVID-19 treatment 53
Although the systematic search captured a significant number of studies in a short time frame, we acknowledge there are some accompanying limitations. Restricting inclusion to the English language probably omitted other thematic studies. The pandemic's dynamic nature and short time reporting scope probably caused reporting bias, which might be corrected over time. Nevertheless, our report outcomes are in line with other conducted cross-sectional studies such as the WHO studied report. 8
In summary, this systematic review demonstrated the widespread practice of antibiotic prescribing for COVID-19 patients during the pandemic with little supporting evidence of secondary bacterial infections. While the practice is more frequent in adult patients with comorbidities than in the younger population, this might reflect more advanced and severe diseases in this population. We encourage the appropriate and judicious use of antimicrobials, particularly broad-spectrum antibiotics, to avoid short- and long-term consequences. We anticipate if no appropriate actions have been taken throughout the pandemic through various elements of ASPs or tailored COVID-19 management guidelines, such practice might become an established culture with all its detrimental consequences.
Footnotes
Authors' Contributions
Conceptualization, N.O.E.; methodology, N.O.E., S.H.A., and H.A.; resources, S.H.A. and H.A.; writing—original draft preparation, S.H.A., H.A., A.J., and H.A.H.; writing—review and editing, N.O.E., H.A.H., H.M.Y., and A.A.A.
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the Biomedical Research Center, Qatar University.