
Abstract
Abstract
Purpose:
The present study is the first randomized clinical trial designed to evaluate the intraocular pressure (IOP)-lowering effect of anecortave acetate (AA) administered at 3 doses (3, 15, or 30 mg) as an anterior juxtascleral depot (AJD) in patients experiencing elevated IOP due to corticosteroid therapy.
Methods:
This was a double-masked, randomized, placebo-controlled, multicenter, parallel group trial. Eligible patients had an IOP of at least 24 mmHg and an IOP increase of at least 10 mmHg relative to their IOP before treatment with steroids. A target IOP was established for each patient at baseline. Patients were randomized to 1 of the 4 treatment groups: vehicle, 3 mg AA, 15 mg AA, or 30 mg AA. All patients then received a 0.5 mL AJD of the assigned treatment. Patients returned for scheduled examination visits at weeks 1, 2, 4, 6, months 3, 4, 5, and 6. IOP was measured at each visit as well as best corrected visual acuity (logMAR), ocular motility, eyelid responsiveness, slit lamp examination, and assessment of any adverse events. In addition, at baseline and at exit, a dilated fundus examination was carried out and the lens was examined using LOCS II criteria.
Results:
Seventy patients were randomized to treatment. At week 4, eyes in the vehicle group showed a 3.4 mmHg (9.1%) decrease from baseline. Reductions for the 3 mg AA (3.1 mmHg, 10.7%) and the 30 mg AA groups (5.4 mmHg, 16.6%) were not significantly different than for vehicle control. However, IOP for the 15 mg AA group at week 4 was reduced 11.5 mmHg (31.3%) from baseline, which was statistically significant (P=0.0487). The mean time to treatment failure was 32.2, 38.9, 56.3, and 32.6 days for the vehicle, 3 mg AA, 15 mg AA, and 30 mg AA groups, respectively. Adverse events were assessed at each post-treatment visit. There were no serious adverse events that were determined to be related to the test article or its administration.
Conclusions:
AA can be of benefit to some patients requiring treatment with corticosteroids, but suffering from the side effect of elevated IOP.
Introduction
Anecortave acetate (AA) is a cortisene, a synthetic derivative of cortisol. Removal of the 11 β-OH group from cortisol's B ring and introduction of a C9–11 double bond renders AA devoid of glucocorticoid receptor agonist activity. 11 AA has 2 inherent pharmacological activities; it has antiangiogenic properties through inhibition of the angiogenic proteolytic cascade,11–13 and it has IOP-lowering activity.14–16
AA has been shown to lower IOP in steroid-induced ocular hypertensive patients in a case series of 8 eyes from 7 patients with medically uncontrolled IOP following intravitreal injections of triamcinolone acetonide. 14 AA has also been shown to lower IOP in steroid responsive sheep and to prevent IOP elevation in the same model system. 15 The present study is the first randomized clinical trial designed to evaluate the IOP-lowering effect of AA administered at 3 doses (3, 15, or 30 mg) as an anterior juxtascleral depot (AJD) in patients experiencing elevated IOP due to corticosteroid therapy.
Methods
This was a double-masked, randomized, placebo-controlled, multicenter, parallel group trial. The study was reviewed and approved by the Sterling Institutional Review Board and by local institutional review boards or ethics committees where appropriate. All participating patients provided written informed consent. The study was HIPAA compliant and was conducted under the tenets of the Declaration of Helsinki. The study protocol was registered on ClinicalTrials.gov (NCT00315640).
This was a multicenter study conducted at 18 sites throughout the United States, Europe, Mexico, and Brazil. Eligible patients were of either sex, and any race, 18 years of age or older, with an IOP of at least 24 mmHg and who had an IOP increase of at least 10 mmHg relative to their IOP before treatment with steroids.
Patients were excluded from the study for any of the following criteria: ocular trauma within the past 6 months in the study eye; the presence of a scleral buckle; a cup-to-disc ratio greater than 0.80 in either eye; any abnormality preventing reliable applanation tonometry; anticoagulant therapy other than antiplatelet therapy; evidence of scleral thinning; pregnancy or the intent to become pregnant during the study; breast feeding.
Patients under treatment with ocular hypotensive medications at the time of screening were allowed to enroll provided that they had at least 30 days stable dosing before enrollment for these medications, and that the treatment regimen was not changed during the study. Eligibility IOP requirements were the same whether or not a patient was receiving prestudy IOP-lowering therapy.
A target IOP was established by the investigators for each patient who provided informed consent and met inclusion/exclusion criteria at the screening/baseline visit. This target IOP was at the investigators' discretion and depended on the individual characteristics of each patient, including baseline IOP and health of the optic nerve. Following the setting of a target IOP, patients were randomized to 1 of the 4 treatment groups: vehicle, 3 mg AA, 15 mg AA, or 30 mg AA. All patients then received a 0.5 mL anterior sub-Tenon's injection of the assigned treatment. Before the injection, eyes were prepared as follows: instillation of proparacaine HCl (Alcaine®; Alcon Laboratories, Fort Worth, TX) followed by placing 5% povidone-iodine (Betadine®; Alcon Laboratories) in the cul-de-sac and closing the eye for at least 1 min. A wire lid speculum was inserted into the eye and the site of injection was selected between 4 o'clock and 8 o'clock and at least 5 mm posterior to the limbus in an area free of large conjunctival or episcleral vessels. Additional proparacaine was applied to the site of injection with a cotton swab or pledget for a minimum of 30 s. Injections were carried out using a 30-g needle and Fechtner forceps (Katena Products, Inc., Denville, NJ) to grasp the conjunctiva. A drop of topical antibiotic (e.g., moxifloxacin) was applied post-injection. Each injection was recorded with a digital video camera. The recordings were reviewed by the sponsor's medical monitor within 1 week to ensure that the AJD was given according to standard procedure.
Patients returned for scheduled examination visits at weeks 1, 2, 4, 6, months 3, 4, 5, and 6. IOP was measured at each visit as well as best corrected visual acuity (logMAR), ocular motility, eyelid responsiveness, slit lamp examination, and assessment of any adverse events. In addition, at baseline and at exit, a dilated fundus examination was carried out and the lens was examined using the LOCS II criteria.
Beginning at week 4, investigators could rule a patient a treatment failure and add appropriate rescue medication according to the following criteria: if the patient's IOP for the study eye exceeded the established target IOP and remained above the target IOP at a subsequent additional IOP check (scheduled at the investigators discretion, generally within a week). Patients ruled treatment failures remained in the study for the full 6 months; however, the last IOP measurement before the addition of rescue therapy was carried forward for analysis for subsequent visits. Missing data, either due to a missed visit or an early discontinuation for any reason (e.g., withdrawn consent, adverse event, treatment failure), was imputed using the method of last observation carried forward. In the case of a treatment failure, this means that the IOP carried forward for all subsequent visits was the failed IOP. This is a conservative procedure as it does not exaggerate the treatment effect of the drug at later study visits by only considering successes.
The primary statistical objective of the study was to demonstrate that AA (3, 15, and/or 30 mg) was superior to the placebo control with respect to IOP reduction. The primary efficacy end point was mean change in IOP from baseline at the week 4 visit. Hypothesis tests were performed using repeated measures analysis of variance. Multiplicity was adjusted using Hommel's method. Secondary efficacy parameters included the time to treatment failure and the percentage of patients declared treatment failures. Kaplan-Meier survival analysis was used to estimate times to treatment failure.
Planned enrollment was 60 patients. With 15 evaluable patients per group, there is at least 95% power to demonstrate a difference of ≥5 mmHg between any 2 groups. This sample size is based on a 2-sided t-test procedure with α=0.05 and an assumed standard deviation of 3.5 mmHg. With a standard deviation as high as 4.1 mmHg, there would still be approximately 90% power to achieve the planned primary objective.
Results
Seventy patients were randomized to treatment. All patients were evaluable for safety and for the intent-to-treat (ITT) data sets. Eleven patients were excluded from the per protocol (PP) data set (AA 3 mg, n=4; AA 15 mg, n=2; AA 30 mg, n=4; vehicle, n=1) because of protocol violations. These violations included less than 30 days stable dosing with prestudy IOP-lowering medications (n=7), history of trabeculectomy in the study eye (n=2), and nonqualifying IOP (n=2). Patient demographic data are tabulated in Table 1. Primary and secondary outcomes were similar for PP and ITT data sets. The majority of patients were male, Caucasian, under 65 years of age, and with brown irides. There were no significant differences in demographics between the treatment groups, although with respect to iris color, the vehicle group had a majority of patients with blue irides. Thirty percent (21 of 70) of the patients entering the study had prior vitrectomy surgery in the study eye; 3 in the 3 mg, 4 in the 15 mg, 7 in the vehicle and 30 mg groups. A sensitivity analysis was carried out excluding those patients with prior vitrectomy. There were no differences in conclusions based on these results and those from the larger ITT data set.
P value from χ2 or Fisher exact test.
SD, standard deviation.
Most patients (61 of 70) had been treated with triamcinolone acetonide before the study. These were primarily intravitreal injections (57 of 61) and were in most cases the patient's first injection with triamcinolone (51 of 61). Patients who had multiple prestudy triamcinolone injections were evenly distributed across the treatment groups (N=2 or 3 per group). The average dose of triamcinolone acetonide was similar for the 3 AA treatment groups (11.7, 10.6, and 11.4 mg for the 3, 15, and 30 mg groups respectively), and was about twice that for the vehicle group (average triamcinolone dose=5.5 mg). The interval between triamcinolone injection and administration of AA was also similar across the 3 AA treatment groups (84, 88, and 79 days for the 3, 15, and 30 mg groups, respectively), but again, was different for the vehicle group (average interval=33 days). An additional sensitivity analysis was carried out evaluating only those patients entering the study following intravitreal triamcinolone acetonide (IVTA) treatment. There were no differences in conclusions between the IVTA only dataset, or for ITT.
Primary inference for this study was based on the comparisons of mean change from baseline in IOP at week 4 for each of the AA active drug groups versus the vehicle group (Fig. 1). At week 4, eyes in the vehicle group showed a 3.4 mmHg (10%) decrease from baseline. Reductions for the 3 mg AA (3.1 mmHg, 10%) and the 30 mg AA groups (5.4 mmHg, 16%) were not significantly different than for vehicle control. However, IOP for the 15 mg AA group at week 4 was reduced 11.5 mmHg (31%) from baseline, which was statistically significant (P=0.0487) and over 8 mmHg greater than seen in the control group. The mean IOP changes from baseline and for percentage change in IOP, for each visit by treatment group are given in Table 2. Baseline IOP for the 4 treatments were similar (34.1, 31.1, 37.6, 32.9 mmHg for vehicle, 3, 15, 30 mg, respectively).
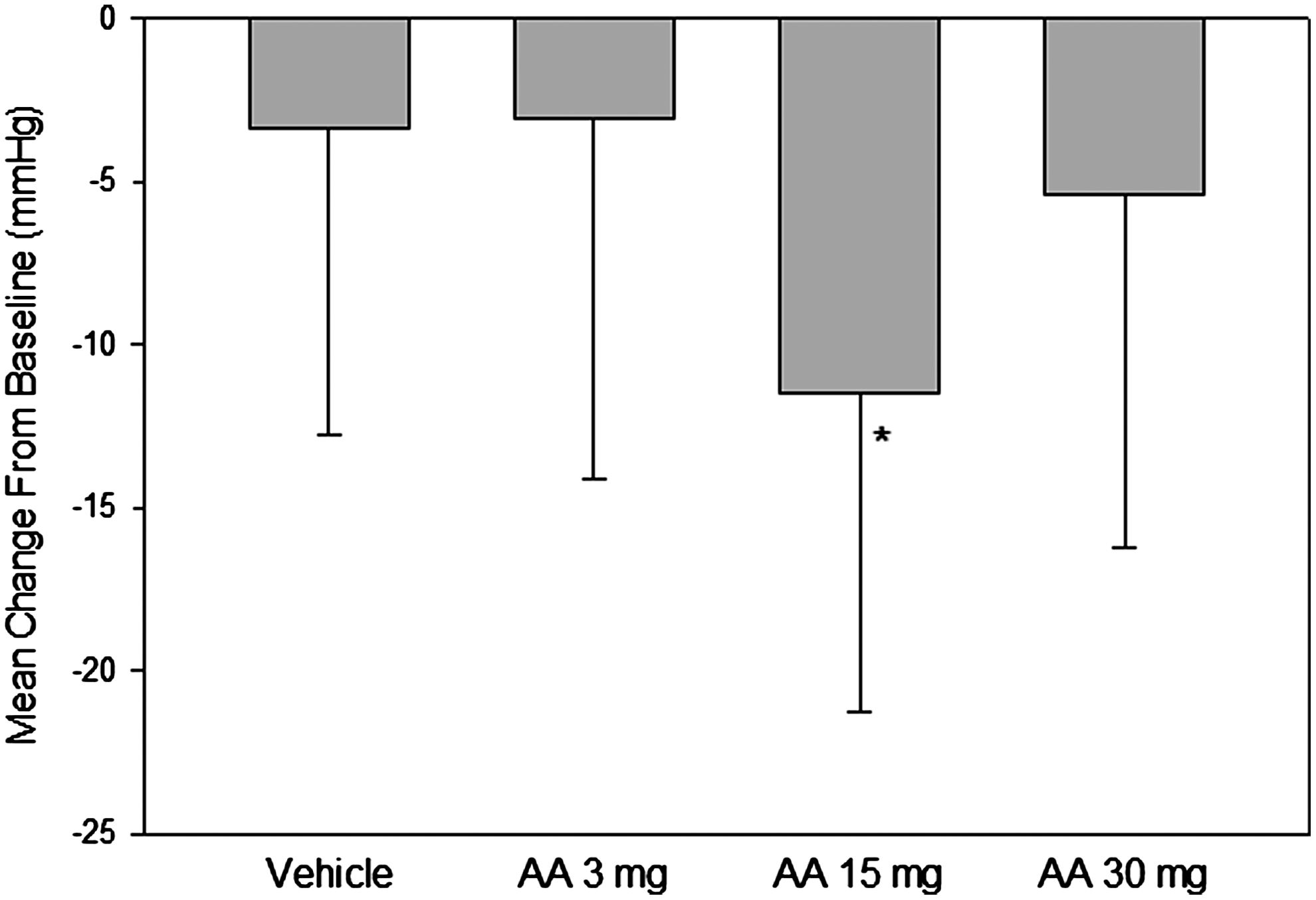
Mean IOP change from baseline at week 4. Error bars are 1 standard deviation. AA, anecortave acetate; IOP, intraocular pressure. *Significantly different from baseline, P=0.0487.
AA, anecortave acetate; % chg, percent change in IOP from baseline; IOP, intraocular pressure.
There was no significant difference in the frequency of treatment failure at any visit; however, there were interesting trends that are congruent with the IOP data. Survival curves indicated that the frequency of treatment failure was highest for the vehicle group at all time points. The 15 mg AA group had the lowest frequency of treatment failure at 5 of 7 time points. At 6 months (exit visit), the 15 mg group had 53% of patients requiring additional IOP-lowering medication, while the vehicle, 3 mg AA, and 30 mg AA groups were 77%, 67%, and 56%, respectively. These data are depicted as Kaplan-Meier plots in Fig. 2. For patients who were declared treatment failures, the mean time to failure was 32, 39, 56, and 33 days for the vehicle, 3 mg AA, 15 mg AA, and 30 mg AA groups, respectively.
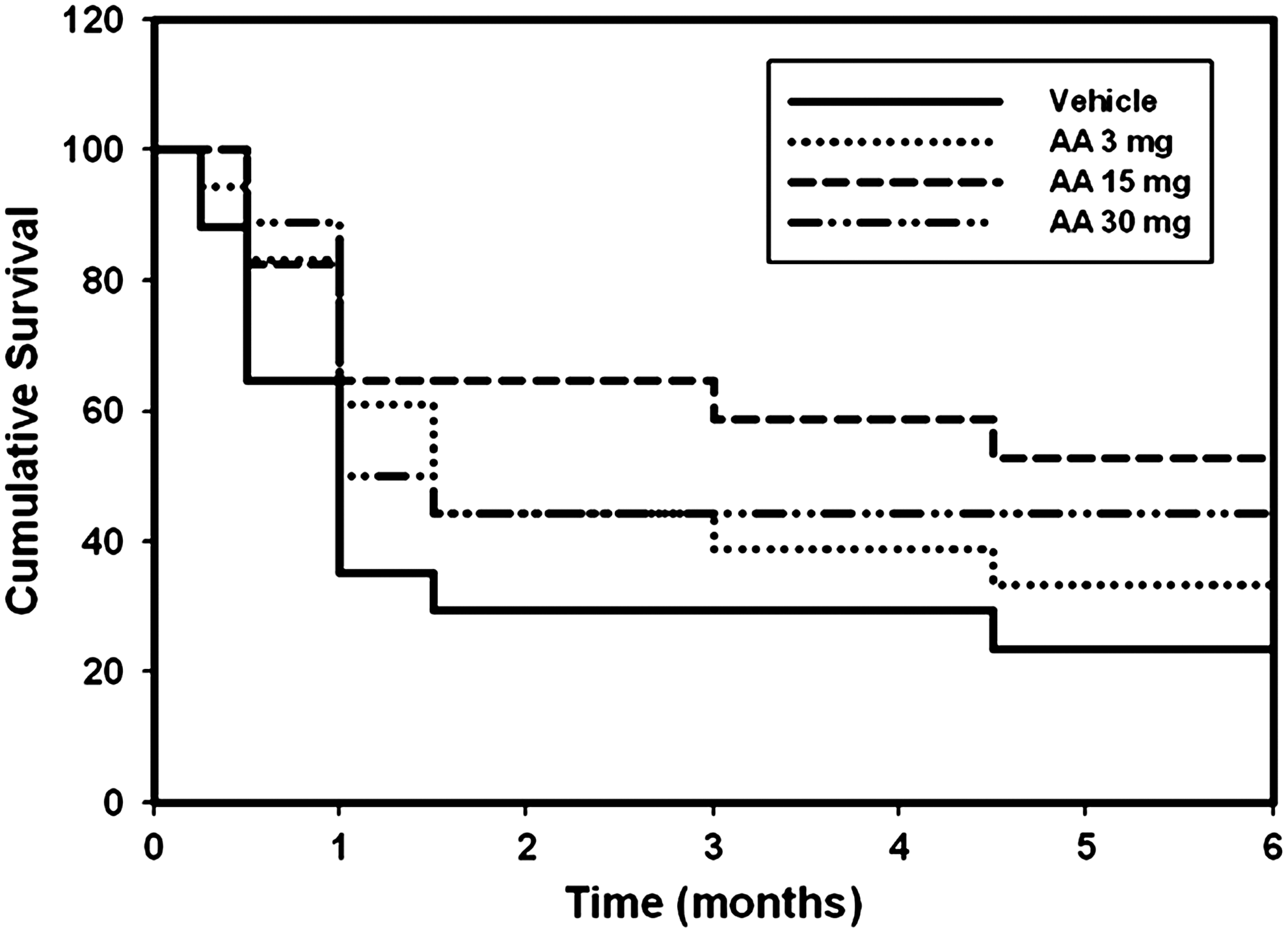
Kaplan-Meier plot showing time to treatment failure.
Enrollment in this study was not evenly distributed across the investigative sites. One site enrolled nearly one-third of the patients (N=23); 4 sites accounted for another 23 patients with the remaining 24 patients distributed across 13 sites. To evaluate the role that experience in administering the AJD might play in the efficacy of treatment, the patients were divided into 3 groups, high-enrolling site (N=1), mid-enrolling sites (N=4), and low-enrolling sites (N=13). Figure 3 plots the percentage of patients enrolled in each of these 3 groups who received active drug (the vehicle patients are excluded) who were not treatment failures at week 4, month 3, and month 6 for each of these groups. The lowest rate of success at all 3 time points was that for the low enrolling group. The highest enrolling site had the greatest success rate at 2 of 3 time points.
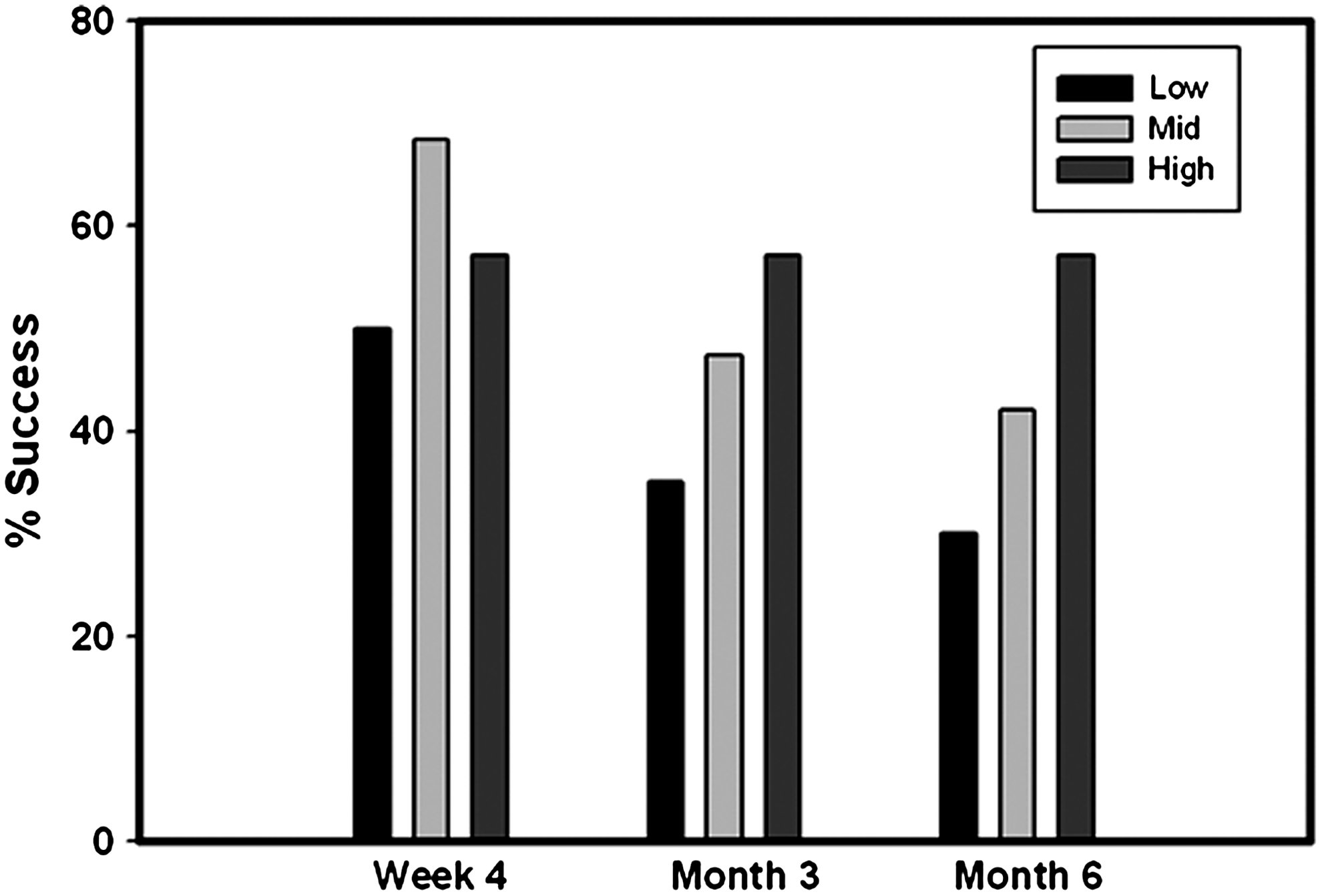
Percent treatment successes at week 4, and months 3 and 6 for low-, mid-, and high-enrolling sites. Treatment success for patients randomized to active treatment defined as IOP controlled without the use of adjunctive medications. Low, sites enrolling 1–4 patients (13 sites, N=24 patients); mid, sites enrolling 5–7 patients (13 sites, N=23 patients); high, 1 site that enrolled 23 patients.
Adverse events were assessed at each post-treatment visit. There were no serious adverse events that were determined to be related to the test article or its administration. One patient treated with AA 30 mg discontinued the study early due to a nonserious adverse event (macular edema), which was assessed as unrelated to the test article or the AJD procedure. The most frequent adverse events associated with either AA or the AJD procedure are listed in Table 3. Adverse drug reactions included keratitis and worsening of cataract. Procedural-related adverse events included conjunctival hemorrhage, eye pain, and hyperemia. No dose-related trend was observed for any adverse event, and the incidence of adverse drug reactions and those related to the AJD procedure were similar for the AA 3, 15, and 30 mg groups.
AE, adverse event; AJD, anterior juxtascleral depot.
Discussion
Corticosteroids are often necessary to provide effective treatment for serious systemic and ocular inflammatory conditions. Elevation of IOP is a known risk accompanying the use of these drugs. In a study of 305 eyes from 272 patients given IVTA for various retinal pathologies, Jonas et al. found that up to 40% of patients experienced an increase in their IOP above 21 mmHg. 17 Similar results have also been reported for a population of 147 Chinese patients 18 and for a group of 108 patients from the Southampton University Eye Unit in the United Kingdom. 19 Even more striking, pooled data from 3 large multicenter trials of the sustained release fluocinolone acetonide implant (Retisert; Bausch and Lomb, Rochester, NY) found that 71% of implanted eyes had an IOP increase of 10 mmHg or more from baseline. 20 Clearly, a means to suppress or counter the IOP elevation, while not interfering with the glucocorticoid receptor-mediated effects of these drugs (i.e., anti-inflammatory, angiostatic) would allow for a greater margin of safety with corticosteroid therapy.
AA is one of a class of steroid-derived compounds known to lower IOP, but devoid of conventional steroid hormone activitiy. 11 The precise molecular mechanism of action is not well understood, however, it has been shown that it does not bind the glucocorticoid receptor. 21
AA has been reported to have IOP-lowering efficacy for both steroid-induced elevated IOP, 14 and for elevated IOP associated with open-angle glaucoma. 16 These were small case series without a control group, and therefore, the true magnitude of the treatment effect is difficult to interpret. The IOP elevation produced by steroids eventually diminishes and the pressure will return to baseline as the steroid effect wears off. Thus, without a placebo control it is difficult to distinguish between the expected ebbing of the steroid response, and an actual IOP reduction produced by AA.
The present study employed a control group and 3 different doses of AA. The decrease in IOP with time seen in the vehicle group (refer to Table 2) was almost certainly due to a diminution of the steroid hypertensive effect with time. It should be noted that the average dose of triamcinolone acetonide for patients in the vehicle group was only about half that received by the patients in the 3 AA groups (5.5 mg vs. approximately 11 mg) and this could certainly have been a factor in the large placebo effect seen at month 6. However, the interval between triamcinolone and AA administration was also shortest for the vehicle group (33 days vs. approximately 80 days) making it less likely that the steroid effect had worn off relative to the 3 AA groups at month 1 (the primary end point). Prior history of vitrectomy in the study eye could have resulted in more rapid clearance of intravitreal triamcinolone, which could contribute to a decrease in IOP over time. Approximately one-third of the 30 mg AA group had a prior vitrectomy, while the 15 mg group had only half as many, making it unlikely that this was an important factor in the overall efficacy. Of the 3 active treatment groups, only the 15 mg AA group was statistically superior to vehicle. The 30 mg AA group showed numerically greater reductions from baseline than did vehicle, and perhaps with a larger sample size these differences would be statistically significant.
At least half of all subjects receiving any dose of AA were able to remain free of additional IOP-lowering medications at 1 month post-AA injection in contrast to only about one-third in the vehicle group, a trend indicating an IOP-lowering benefit for patients at all dose levels.
There were very few adverse events assessed as related to AA. Two of the three that were reported were for worsening of cataract. It is worth noting that a well-known side effect associated with corticosteroid treatment is the development of cataract. It is therefore very likely that the cause of cataract progression observed in these 2 patients was the original steroid insult, and not the AA. Furthermore, AA's lack of glucocorticoid activity casts additional doubt on its culpability.
A weakness of this study is the relatively small sample size relative to the amount of variability in the data. Initial power calculations were predicated on an assumed standard deviation in the IOP measurements of 3.5 mmHg as is commonly used for randomized clinical trials with glaucoma patients. 22 In fact, the standard deviation for the IOP measurements in this study was approximately 10 mmHg. There are probably multiple sources for this high variability. First, there is a natural time-course to the IOP response from treatment with corticosteroids. Because the patients for this study were generally identified after they had experienced an IOP increase, it was not always possible to standardize the time of AA administration relative to the initial IOP increase. Furthermore, this variability could be exacerbated by differences in the type, dose, route of administration, history of vitrectomy, and bolus versus chronic exposure for the corticosteroid treatment, although as noted in the results, the majority of patients had been treated with triamcinolone acetonide. Second, the successful administration of an AJD is dependent on the skill and experience of the investigator. This is a difficult variable to quantify a priori, however, all injections for this study were video recorded and reviewed by the sponsor. Feedback was given to the investigators for each injection. It was found to be generally true that the more experience (greater number of injections) an investigator had with the technique, the better the quality of the injection. This qualitative view is supported by the data shown in Fig. 3. There were more treatment successes at mid- and high-enrolling sites, than for low-enrolling sites. Third, individual differences in steroid responsiveness are well known and thought to have a genetic component.23–25 It is likely that response to AA is also dependent on an individual's genotype. We believe further study is warranted to explore this possibility.
It is interesting that the 15 mg AA middle dose provided better IOP-lowering efficacy, and more sustained IOP-control than the 30 mg AA high dose. One explanation could be that the 15 mg dose is pharmacologically optimal with diminished efficacy at higher doses. We do not believe this is likely. Robin et al. used a dose of 24 mg administered precisely as described here and found it to provide a mean IOP reduction of 14 mmHg at 1 month for steroid-induced ocular hypertension patients, and between 8 and 9 mmHg for up to 6 months in patients with open-angle glaucoma.14,16 Additionally, Candia et al. successfully prevented prednisolone-induced IOP elevation in steroid-responsive ovine eyes using a dose of 75 mg AA. 15 Our feeling is that the low performance of the 30 mg AA group relative to the 15 mg AA group is a random outcome likely due to the high variability observed in the data, and the relatively small sample size employed in this study. The 3 mg treatment group is statistically and numerically indistinguishable from vehicle in IOP-lowering efficacy at all time points (Table 2). If the 3 mg AA treatment could thus be considered a subclinical dose, and the 15 and 30 mg groups considered active, pooling of the data for the vehicle and 3 mg groups and for the 15 and 30 mg groups demonstrates a mean IOP reduction of 3.2 mmHg (vehicle+3 mg, N=35) versus 8.4 mmHg (15+30 mg, N=35; P=0.027, 1-tailed t-test). Although this is a post hoc analysis, the approximate 5 mmHg reduction relative to vehicle may be a more accurate estimate of the IOP-lowering benefit that could be expected in patients with steroid-induced IOP elevation.
We here provide data from a randomized controlled study demonstrating that AA can be of benefit to some patients requiring treatment with corticosteroids, but suffering from the common side effect of elevated IOP. Treatment with AA may provide long-lasting IOP-control for such patients from a single administration. Adverse events were found to be nonserious and easily tolerated. Development of long-acting IOP-lowering therapies like AA is clearly needed.
Footnotes
Author Disclosure Statement
Drs. Callanan and Robin are consultants of Alcon; Drs. Stalmans, Dirks, Moster, and Van Calster have no financial interest. Drs. Dickerson, and Bergamini were employees of Alcon during the conduct of this study. Dr. Landry and Ms. Scheib are employees of Alcon.