
Abstract
Multidisciplinary team meetings (MDT-Ms) are utilized as a tool for clinical decision-making. Currently, these are in-person or remotely attended via screen-sharing of patients’ electronic health records, including clinical findings, numerical data, and two-dimensional and three-dimensional imaging. Immersive virtual reality (IVR) is an emerging technology that allows multiple care-providers to remotely interact with each other and with patient data in a metaverse—an immersive and collaborative digital environment. An MDT-M held in the metaverse could enhance surgical decision-making. To develop an IVR metaverse for MDT-M and to test its feasibility and efficacy to visualize data and make clinical decisions in the orthopedic trauma setting. Interviews of users attending existing orthopedic trauma MDT-Ms at a regional major trauma center identified strengths, weaknesses, opportunities, and threats for a novel metaverse platform. This was iteratively tested for feature development, and 24 simulated cases were curated from previous admissions. Pilot MDT-Ms were conducted, and user experience was measured using the NASA Task Load Index (NASA-TLX) and System Usability Scale. An IVR metaverse platform was developed to conduct MDT-Ms with multiple remote participants. Four MDT-Ms were successfully conducted with health care professionals (n = 13). Participants found that “data visualization” and “clinical decision-making” were effective in IVR: median 5 (interquartile range [IQR], 4–5) and 5 (IQR, 4–5), respectively. Ratings on “ease of communication” in the metaverse varied with a median of 3 (IQR, 2–4.5). Qualitative analysis highlighted the strength of IVR to interrogate 3D anatomy and injury patterns collaboratively and quickly. The NASA-TLX domain “task performance” was rated consistently highly, indicating the ability to use presented data to advance patient management. Health care professionals can feasibly conduct complex MDT-Ms using a novel metaverse platform on commercially available IVR headsets. Participants were able to collaboratively interrogate clinical data, facilitating enhanced discussion, decision-making, and perceived task performance. Future iterations will focus on improving the designation of roles to improve communication in the metaverse meeting.
Background
A multidisciplinary team (MDT) in health care is defined as a group of individuals across disciplines, who facilitate holistic decision-making related to patient care. 1 The MDT meeting (MDT-M) involves discussion of complex cases by health care professionals, with the aim of improving diagnosis and creating a detailed management plan specific to the individual clinical and psychosocial needs of the patient.2,3 Studies analyzing the perspectives of MDT members have found that scheduling conflicts owing to other responsibilities, poor cooperation within the team, and challenges in viewing multiple information sources at once are some of the factors that hinder effective MDT-Ms.4,5
The rise of hybrid virtual working during the COVID-19 pandemic has spurred a drive toward digitalization in health care.6,7 In immersive virtual reality (IVR), users utilize head-mounted displays to view a completely virtual environment. The ability of IVR to display accurate three-dimensional (3D) models of patient anatomy lends itself to use as a surgical planning tool. 8 IVR has enhanced teamwork in training of nurses and for planning neurosurgery.8,9 Interprofessional education via IVR can deliver a significant increase in collaborative attitudes. 10 In surgical training, IVR can enhance knowledge and technical skills of surgeons 11 and nurses. 12 Multiplayer IVR can enhance interdisciplinary, nontechnical skills, including communication, leadership, and decision-making. 13
Extended reality (XR) technology is a unifying immersive and collaborative digital environment, in which users can interact with each other and their surroundings in a life-like manner and outside of a defined timeline,6,14 for a specific experience, or to perform specific tasks. 14 XR technology designed for conducting MDT-Ms in health care could address challenges of existing in-person MDTs while enhancing collaboration and decision-making. 15
Orthopedic trauma MDT-Ms are typically attended by surgeons of varying subspecialties, nurses, physiotherapists, radiologists, microbiologists, and physicians. They rely on health care professionals evaluating clinical findings, laboratory results, and multimodal imaging to create individualized management plans.16–18 Imaging typically includes clinical photographs, plain radiographs, and multiplanar images from ultrasound, computed tomography (CT), and magnetic resonance imaging and 3D reconstructions. Management requires an understanding of patient factors, injury factors, local system factors, and cost-effectiveness. 19 There is a wide demographic of patients presenting with orthopedic trauma, including elderly patients with fragility fractures and typically younger patients with high-energy trauma to multiple regions of the body. This calls for patient-centered conservative and surgical management plans19,20 and timely decision-making to determine priority and urgency. 21 Orthopedic trauma surgery is thus an ideal situation for testing whether an XR technology can better facilitate patient-centered decision-making.
Our aim is to develop an IVR-based technology for a surgical MDT-M and to pilot its feasibility and efficacy to visualize data and make clinical decisions in the orthopedic trauma setting.
Methods
Study design
After institutional approval, this study was conducted in four stages: (1) qualitative evaluation of existing orthopedic trauma MDTs, (2) a scoping review of the literature and the commercial market for existing XR technology solutions, (3) development of an XR technology MDT-M, and (4) pilot testing with multiple health care professionals conducting an XR technology MDT-M using simulated orthopedic trauma and planned surgical cases.
Evaluation of existing orthopedic trauma MDT-Ms
Semi-structured interviews were conducted with health care professionals attending four consecutive orthopedic trauma MDT-Ms at a regional tertiary trauma center, collating their opinions on literature-identified barriers and facilitators of MDT-Ms. To develop a feature list for a minimum viable product XR platform, the MDT-Ms were evaluated to determine what patient data are required, what software is currently in use to present clinical data, the format of the MDT-M (whether entirely in-person, online, or hybrid), and location and role of attendees. A SWOT (strengths, weaknesses, opportunities, and threats) analysis was conducted with these data. Finally, the clinical pathway of 50 consecutive patients presenting to the orthopedic department was evaluated to create decision trees. This would allow for the MDT members to be asked standardized questions and systematically record their decisions for each patient, akin to a chatbot. 22
Scoping review of the literature and testing of commercially available XR technology products
A scoping review of relevant literature was performed by searching PubMed Medical Literature Analysis and Retrieval System Online and Cumulative Index to Nursing and Allied Health Literature from inception through August 2022. The keywords were “virtual reality,” “MDT” or “multidisciplinary team,” and “clinical decision.” This included all medical and surgical specialties. Results were screened for relevance to the study. The findings of remaining studies were evaluated for existing applications of IVR in MDT-Ms and the respective challenges and facilitators to their implementation.
Attendance at digital health technology conferences and exhibitions (Future Surgery, London, and Giant Health, London) between February and December 2022 identified existing XR technology solutions for medical education and training. This provided an understanding of health care innovations in MDT-Ms, previously identified challenges, and existing applications of IVR in this domain.
Commercially available software solutions were then evaluated for their suitability for conducting an MDT-M and closeness of fit to the minimum viable product feature list. The assumption was that it would be faster and more cost-effective to adapt an existing and widely available software than build one ab initio. Similar testing was carried out for hardware and devices, and the most appropriate hardware was selected based on a combination of suitability for study aims, practicality, and costs.
Developing and pilot testing an XR technology MDT-M
Development
Information Centric Engineering (ICE) principles were used to adapt an existing, commercially available IVR platform so that it could deliver an MDT-M suitable for multiple health care professionals collaborating to make decisions for patients with complex orthopedic trauma. ICE involves modeling, simulation, and exchange.23,24 Modeling, simulation, and exchange (of information) are the three core facets of ICE. Modeling involves the creation of functional and process models that describe the target simulator in an information-intensive document, including the resources and technologies required to deliver it. Simulation involves the design of 3D simulation models (in IVR) for processes at various levels of abstraction. The third facet, exchange, involves the collaborative exchange of information and data between cross-functional users so that ideas and models are communicated in real time to enable timely assessment, comparison, and validation of candidate plans. This can involve face-to-face interactions typically between subject matter experts (in this case, orthopedic surgeons) and software engineers, written communications, and cyber–physical interactions for collaborative development within virtual reality spaces. This latter approach enables team members who are geographically distributed to interact within a virtual space to develop IVR solutions in an agile way. “Agile software development” 25 refers to a collaborative approach between designers with different technical know-how, performed with the following principles in mind: (1) early and continuous delivery, (2) welcome of changing requirements, (3) short iterations and releases, (4) motivated individuals, (5) working software as a measure of progress, (6) technical excellence, (7) simplicity, and (8) self-organizing and reflective teams.
Data from the qualitative evaluation of existing orthopedic trauma MDT-Ms were used as the ground truth for adapting a virtual environment. Software programmers collaborated with orthopedic surgeons to iteratively evaluate mock patient datasets, including electronic health record (her) data, digital imaging and communications in medicine (DICOM) data, and management options to create an MDT-M XR technology with clinical relevance, technical feasibility, and face validity. The minimum viable product was developed and implemented through videoconferences and email correspondence. There were user tests, bug tracking, and iterative software releases. ICE and agile development resulted in a reduction in time to design and build the simulator environment, a reduction in the number of changes required between collaborative sessions, and a better understanding of the complexities of the simulation by all team members.
Medicalholodeck® platform
The virtual reality (VR) platform used to host the trial MDT in this study was Medicalholodeck, a software used for medical applications in VR. This existing software addressed several of the requirements of a VR MDT, as displayed in Figure 1. The base software consists of Medical Imaging XR, Dissection Master XR, and Anatomy Master XR. However, the commercially available solution did not allow for multiple datasets to be viewed simultaneously, did not allow for text files or photographs to be uploaded, and had basic multiplayer capability. Collaboration with Medicalholodeck led to the development of a bespoke, adapted platform with additional functionalities. The desired structure for the platform was conveyed as depicted in Figure 2a.
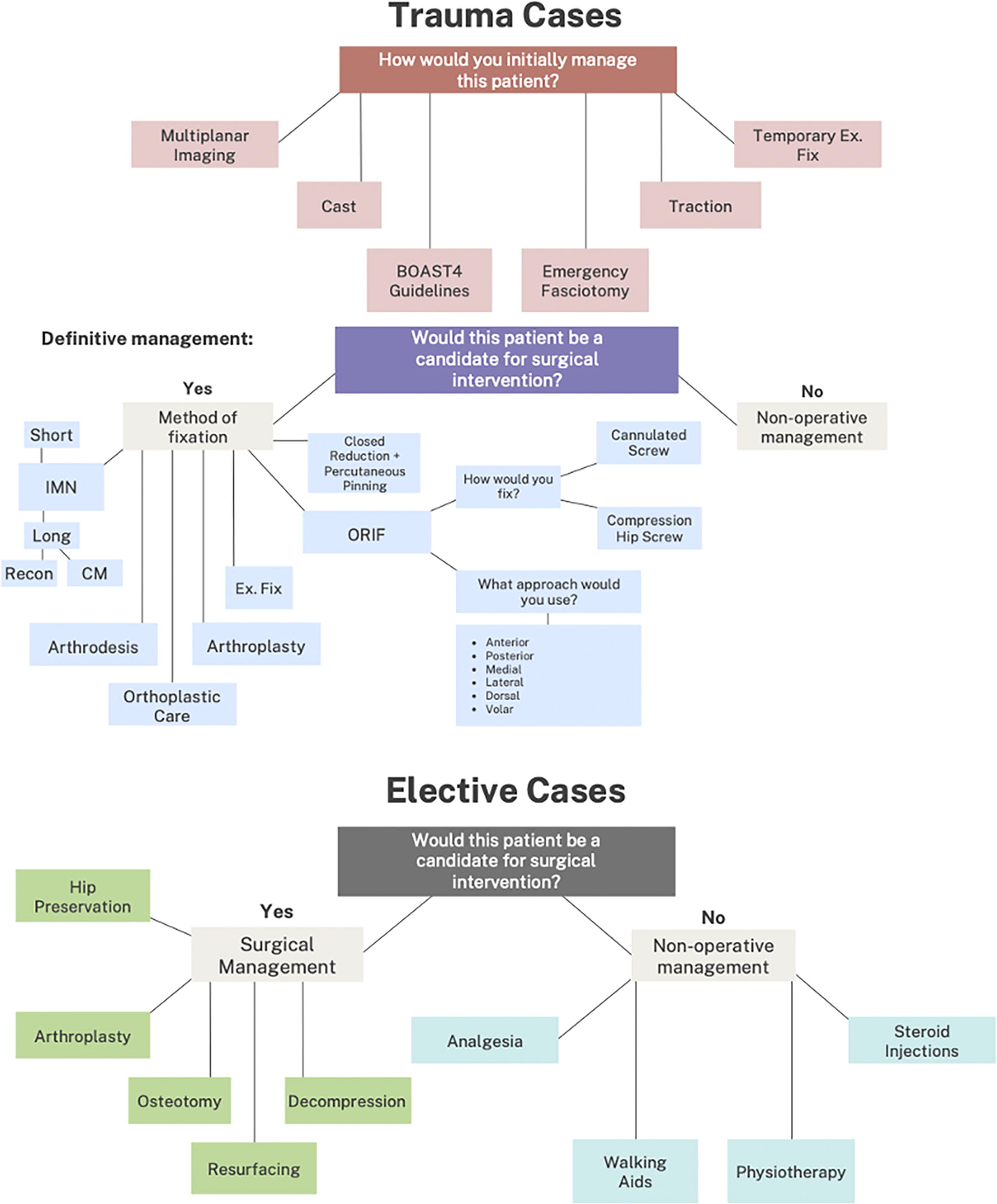
Clinical decision trees derived to facilitate structured discussion of patient cases and to record final management decisions. BOAST, British Orthopaedic Association Standards for Trauma; CM, cephalomedullary; Ex. Fix, external fixation; IMN, intramedullary nail; ORIF, Open Reduction and Internal Fixation.

Depictions of the IVR MDT-M platform and setup.
In this study, the Medical Imaging XR was used for viewing of the anonymized DICOM files in the simulated cases, as in Figures 2b and 2c. DICOMs were viewed in 3D format from the individual slices. Interaction with DICOMs included a slice function with the left hand, length measurement tool, angle measurement tool, drawing tool, and placement of arrow markers. Further functions included a zoom tool, movement of the DICOM, enlargement, and rotation in both x and y planes. The modality, contrast, and coloring of DICOMs were adjustable. DICOMs for each case were appropriately uploaded to laptops in advance and were uploaded to the platform via the “upload from drive” function.
Pilot testing
Participants and questionnaires
Consenting volunteer participants were recruited from existing memberships of two MDT-Ms, in orthopedic trauma, and hip and knee arthroplasty, based at Imperial College Healthcare NHS Trust. Participation required consent to participate in the pilot MDT and completion of questionnaires as given in Supplementary Data S1 and Supplementary Data S2. Exclusion criteria included a history of motion sickness, history of migraines, and history of epilepsy, because of the possibility of adverse effects to VR. 26
Outcome measures
The meeting questionnaire in Supplementary Data S1 evaluated participants’ familiarity and experience with orthopedic MDT-Ms and IVR software. Meeting questionnaires in Supplementary Data S2 evaluated participant experiences of the XR MDT-M. Validated questionnaires of the NASA Task Load Index (NASA-TLX) 27 and System Usability Scale (SUS) 28 were adapted to the given task and incorporated into the questionnaire given in Supplementary Data S2. The NASA-TLX allows subjective evaluation of the demand involved in task completion across the following six domains: mental demand, temporal demand, performance, effort, frustration, and physical demand. It has been widely validated and used in the analysis of tasks, both in surgical specialties and IVR.29,30 SUS is used for evaluation of software and was adapted in this study to specifically focus on the XR MDT. 28 Statements were rated from “Strongly Disagree” to “Strongly Agree” on a scale translating to a Likert scale (1–5).
The pilot tests of the XR technology MDT-M were evaluated using the following outcomes: number of cases discussed, average time taken for each case, and the proportion of cases in which the management plan was established. User experience outcomes evaluated users’ perceived opinions on the IVR MDT-M. These included perceptions on ease of use, case visualization, communication, task completion, and demand.
Simulated cases
Patient cases were compiled for discussion in the MDT trial. Anonymized DICOMs were identified from existing image banks at linked centers (Imperial College Healthcare NHS Trust and MSk Lab, Imperial College London), and mock cases were compiled around their presentation. Patients had consented for the use of their anonymized data for education and research. A total of 24 cases were prepared, of which 12 were trauma cases and 12 were elective cases. They included a diverse range of lower limb clinical cases and consisted of DICOMs, a summary of history and examination findings, and any relevant images. Cases were reviewed by two fellowship-trained orthopedic surgeons for clinical accuracy. A decision matrix was developed for recording decisions on initial and definitive management of both trauma and elective cases, as shown in Figure 1.
Results
Evaluation of existing orthopedic trauma MDT-Ms
A total of 25 orthopedic trauma meeting members completed semi-structured interviews. There were three attending surgeons, two attending anesthesiologists, eight orthopedic residents, eight junior doctors, two medical students, one trauma nurse, and one trauma coordinator. This delivered the following three outputs: (1) a SWOT analysis of existing MDT-Ms (Table 1), (2) a feature list for a minimum viable product to conduct an MDT-M (Table 2), and (3) clinical decision trees (Fig. 1).
SWOT Analysis of Existing Multidisciplinary Team Meetings in Orthopedics
EHR, electronic health record; MDT-M, multidisciplinary team meeting; SWOT, strengths, weaknesses, opportunities, and threats.
Features for a Minimum Viable Product to Conduct a Surgical Multidisciplinary Team Meeting
DICOM, digital imaging and communications in medicine; PDF, portable document format.
Advantages and Disadvantages of Software and Hardware Options
3D, three-dimensional; DICOM, digital imaging and communications in medicine; IVR, immersive virtual reality; MDT-M, multidisciplinary team meeting; MR, mixed reality.
Scoping review of the literature and testing of commercially available XR technology products
Scoping of the literature noted that 48 studies were found. Further screening limited this to 27 studies relevant to MDT applications of VR, of which 23 related to multidisciplinary surgical planning and 4 discussed multidisciplinary meetings. There were no instances of IVR MDT-Ms in surgical specialties. Key challenges were identified as image quality, access to IVR technology, and the security of platform utilized for discussion; facilitating factors included team interaction and the ability to accurately indicate lesions in a 3D space.
Outcomes
Investigated outcomes were separated into the following three categories: measures relating to feasibility, efficacy, and user experience. Feasibility was defined as the ability to complete an MDT clinical discussion of the given cases in IVR. This was measured by MDT completion and successful visualization of the simulated cases. Efficacy was evaluated as the quality of the clinical discussion.
Hardware
This study utilized five IVR headsets in total: three Oculus (Meta) Rift and two Oculus Quest headsets, all connected to high-speed internet. Headsets were selected based on institutional access and their advantages in the hardware analysis.
All headsets ran the adapted Medicalholodeck software version locally.
Pilot MDT
The pilot MDT consisted of cases presented in IVR by the MDT coordinator, composed of a patient case summary in .pdf format, CT scans and radiographs as DICOM files, and available clinical photographs in .jpeg format. CT scans were reconstructed into 3D visualization, and cases were discussed by participants with questions regarding patient compatibility with surgical intervention. Final management options were logged onto questionnaire version of the decision matrix in Figure 1.
Data processing
Data were exported into Microsoft Excel (version 16.61.1) and analyzed using GraphPad Prism (version 9.3.0), where they were presented graphically. Statistical analyses were conducted to test normality distribution of the data using Shapiro–Wilk test and quantile–quantile plots, yielding nonparametric data throughout. Mann–Whitney U test was used to compare the means between groups of nonparametric data. p-Values < 0.05 were considered as statistically significant in all analyses.
Results
Data were collected across six IVR MDT-M sessions. In total, there were 13 (n = 13) participants, as summarized in Table 4. Most participants were surgeons (n = 8), and most reported having prior experience of XR (n = 11). The reported MDT experience varied, with “Sometimes (e.g., Several times a month)” being the most stated. The most common uses for XR were stated as being for education, research, and recreational purposes, in the order of decreasing frequency. Online MDTs were reported as the most common mode of MDT-Ms.
Participant Characteristics of MDT Role and Experience
Table displaying participant (n = 13) characteristics in terms of MDT role and experience and XR experience and use. Sections with no participants are represented with —. MDT, multidisciplinary team; XR, extended reality.
Results of the System Usability Scale
Participants rated the given statements, and numerical values were given to the scores: Strongly Disagree (1), Somewhat Disagree (2), Neither Agree Nor Disagree (3), Somewhat Agree (4), Strongly Agree (5). Median, interpretation of median, and interquartile range values have been given. 2D, two-dimensional; 3D, three-dimensional; MDT, multidisciplinary team; VR, virtual reality.
Feasibility outcomes
Multiple MDT-Ms were successfully conducted in IVR, and simulated patient cases were successfully visualized. Connectivity issues were reported by multiple participants on a tethered Oculus Rift headset. Management decisions were logged by a coordinating member out of IVR.
Efficacy outcomes
A total of 16 cases were discussed, across 5 MDT sessions, with a mean time taken per case of 7.8 min (standard deviation = 6.1). All cases (16/16) resulted in management plans.
User experience
Participant scores on the NASA-TLX yielded overall workload scores and scores by dimension, as shown in Figures 3a and 3b, respectively. Overall workload had a median value of 27 (interquartile range [IQR], 16.0–28.5). By dimension, performance was the highest rated metric with a median of 8.0 (IQR, 4.0–8.0). Physical demand and frustration were rated the lowest and had median scores of 3.0 (IQR, 1.0–5.0) and 3.0 (IQR, 1.0–7.0), respectively.

Results of the NASA-TLX displayed by overall workload and individual dimensions.
Discussion
The principal finding of this study was that IVR was both feasible and effective as a method of delivering MDT-Ms. These early data revealed several potential advantages to this approach, most notably, ease of information delivery, and high-fidelity imaging manipulation. This appears to enhance the ability to make patient-centered decisions and plan future management while addressing several well-established barriers to effective MDT-Ms.
A unique capability of IVR incorporated into this study was the ability to reconstruct patient CT imaging in 3D. Studies have shown that the use of IVR in visualization of imaging allows for greater appreciation of the relation of anatomical structures, 8 and, in orthopedics, it has been linked with the reduction of operative time and alterations in management, resulting in fewer surgical procedures. 31 IVR visualization of 3D models may have greater utility than the alternative of printed models, as they incorporate soft tissues that may require consideration when deciding on suitability of a fixation method. 32
Findings of the pilot MDT displayed varied participant opinions relating to communication in IVR. The platform used in this pilot MDT is without set roles and hierarchy of IVR members, and all participants can interact with imaging, including simultaneously manipulating how 3D CT reconstructions are viewed. The absence of a clear role structure in the IVR MDT may have negatively impacted the quality of the clinical discussion. Conversely, recent literature has justified the need for a move away from a set hierarchy of roles in the medical profession.33,34 Despite the effect on the clinical discussion, the benefits of this feature in an IVR MDT may be increasing input from junior colleagues and medical students, 34 which are more likely to act as bystanders in MDT-Ms rather than active involvement. 35
The MDT-Ms in this study consisted of members of an existing orthopedic MDT to maintain relevance to true clinical practice. Cases were reviewed by two senior orthopedic surgeons with attention to clinical accuracy and points of discussion. The use of anonymized DICOMs from actual cases enabled further correlation to clinical practice and replicated surgical scenarios that would be seen in practice.
This project and its findings are not without limitations: owing to the nature of the pilot study, the small participant size limits the reliability and generalizability of the results. A greater range of health care specialties may allow improved generalizability of results to clinical practice. Further specialized teams exist in trauma and orthopedics, such as ortho-geriatrics or ortho-plastics MDTs, and there is a need to evaluate the aims of this study in these groups.36,37
In addition, investigating IVR MDTs in isolation may impede evaluation of efficacy and user experience, requiring the current gold standard of in-person and online MDTs for comparison. The utility of subjective metrics such as the NASA-TLX and SUS may affect result reliability. The NASA-TLX is a subjective marker of task workload, self-reported by participants, which limits the conclusions made from the results. This participant sample may also display recruitment bias in favor of individuals with positive opinions of XR technology, in contrast with the health care field where there is a reluctance to implement new technology, especially IVR.38,39 Finally, variations in case complexity must be addressed to ensure validity of results regarding MDT metrics, for example, the time taken per case. Tonelli et al. 40 demonstrated the use of various markers of patient complexity in evaluating the demand of a case, which may be applied to cases prior to MDT to allow similar scope of discussion throughout the MDT.
Further work
Our findings contribute to a novel but growing base of evidence supporting the use of IVR in MDT-Ms in clinical practice.41,42 Direct comparison with other MDT-M methods is needed to determine the best method of practice. A large-scale MDT trial is required, with a greater participant sample across multiple health care disciplines and comparison of IVR against in-person and online MDT-Ms. The reduced costs of IVR technology in recent years have increased accessibility while simultaneously improving capabilities, yet the uptake in health care fails to reflect this. 43 With high cost of technology being reported as a barrier to implementation of resources, this field would benefit from an up-to-date cost analysis of IVR MDTs. 38
Conclusion
MDT-Ms in IVR are an emerging feasible alternative to current MDT options with several potential advantages. They enable interrogation of multiple complex datasets in a virtual realistic environment, facilitating clinical discussion. The platform developed and tested in this project addressed key barriers of attendance and enabled 3D visualization and manipulation of radiological imaging, decision-making, and surgical planning. Further development is required to test this technology at scale, integrate it into routine workflows with real patients, and further interrogate cost-effectiveness of this promising new technology.
Footnotes
Acknowledgments
The authors would like to thank Christof von Waldkirch and the team at Medicalholodeck for their technical support in this study. An abstract of this article was published in British Journal of Surgery 20234, Volume 110, ![]() , proceedings of Association of Surgeons in Training annual meeting 2023, Liverpool, United Kingdom.
, proceedings of Association of Surgeons in Training annual meeting 2023, Liverpool, United Kingdom.
Authors’ Contributions
This article has been reviewed and approved by all authors.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The funding for this study was provided by the NIHR Imperial Biomedical Research Centre.
Ethical Approval
This study gained ethical approval by institutional review. Informed consent was gained from all participants prior to study participation.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.