
Abstract
Woolcott, Orison O., and Richard N. Bergman. Mortality attributed to COVID-19 in high-altitude populations. High Alt Med Biol. 21:409–416, 2020.
Background:
Since partial oxygen pressure decreases as altitude increases, environmental hypoxia could worsen Coronavirus Disease 2019 (COVID-19) patient's hypoxemia. We compared COVID-19 mortality at different altitudes.
Methods:
Retrospective analysis of population-level data on COVID-19 deaths was conducted in the United States (1,016 counties) and Mexico (567 municipalities). Mixed-model Poisson regression analysis of the association between altitude and COVID-19 mortality was conducted using individual-level data from 40,168 Mexican subjects with COVID-19, adjusting for multiple covariates.
Results:
Between January 20 and April 13, 2020, mortality rates were higher in U.S. counties located at ≥2,000 m elevation versus those located <1,500 m (12.3 vs. 3.2 per 100,000; p < 0.001). In Mexico, between March 13 and May 13, 2020, mortality rates were higher in municipalities located at ≥2,000 m versus those located <1,500 m (5.3 vs. 3.9 per 100,000; p < 0.001). Among Mexican subjects younger than 65 years, the risk of death was 36% higher in those living at ≥2,000 m versus those living at <1,500 m (adjusted incidence rate ratio [IRR]: 1.36; confidence interval [95% CI], 1.05–1.78; p = 0.022). Among Mexican men, the risk of death was 31% higher at ≥2,000 m versus that at <1,500 m (adjusted IRR: 1.31; 95% CI, 1.03–1.66; p = 0.025). No association between altitude and COVID-19 mortality was found among Mexican women or among Mexican subjects 65 years of age and older.
Conclusions:
Altitude is associated with COVID-19 mortality in men younger than 65 years.
Introduction
As of May 13, 2020, 4.17 million people around the world have been tested positive for SARS-CoV-2, the virus that causes Coronavirus Disease 2019 (COVID-19). Nearly 288,000 deaths have been attributed to COVID-19 (WHO, 2020). Severe hypoxemia is a common complication in critically ill patients infected with SARS-CoV-2 (Chen et al., 2020). Since partial oxygen pressure decreases as altitude increases, it is possible that environmental hypoxia could worsen COVID-19 patient's hypoxemia.
Recently, it has been reported that there is a lower absolute number of COVID-19 cases at higher altitudes in Bolivia and Tibet (Arias-Reyes et al., 2020). However, the interpretation of the previous findings is very difficult because data were not reported as rates (e.g., number of cases per 100,000 population) and comparison was performed in a reduced number of cities. Whether COVID-19 mortality rate is different at low and high altitude remains unknown.
The first aim of this study was to compare the mortality rates attributed to COVID-19 in low- and high-altitude populations nationwide in the United States and Mexico. The second aim was to determine the association between altitude and COVID-19 mortality adjusting for risk factors related to COVID-19 and potential confounders.
Methods
This study consisted of two main analyses: (1) a retrospective analysis of data at the population level on all reported COVID-19 cases and deaths attributed to COVID-19 in counties or county equivalents of mainland United States and in municipalities of Mexico and (2) a retrospective analysis of data at the individual level on all confirmed cases of COVID-19 in Mexico. This second analysis was performed to specifically determine the association between altitude and COVID-19 outcomes (pneumonia, requirement for endotracheal intubation, and mortality) adjusting for risk factors related to COVID-19 and potential confounders.
This study did not require approval or exemption from the Cedars-Sinai Medical Center Institutional Review Board as it involved the analysis of publicly available deidentified data only.
Data sources
United States
County-level data on COVID-19 cases and deaths between January 20 and April 13, 2020, were obtained from Newsbreak.com (News-Break Coronavirus Realtime Updates, 2020), an online tracking source of COVID-19 outbreak in the United States that uses data from each state official health division. For verification, we compared the total number of cases and deaths across counties reported by Newsbreak.com and those reported by official sources from Colorado, the state with the larger number of counties located at high altitude in the United States, and New York City, the region with the largest number of cases in the country. At the time of data collection, the cumulative number of COVID-19 cases (7,552 in the state of Colorado and 13,740 in New York City) and deaths (306 in the state of Colorado and 756 in New York City) reported by Newsbreak.com were identical to those reported by the Colorado Department of Public Health and Environment (covid19.colorado.gov) and the New York City Department of Health and Mental Hygiene.
Mexico
Individual-level data on confirmed cases of COVID-19 between January 8 and May 13, 2020, were obtained from the COVID-19 database available from the Secretary of Health of the Government of Mexico. The total cumulative number of COVID-19 cases and deaths attributed to COVID-19 for each municipality were calculated from individual data.
Population estimates were obtained from the latest censuses or latest official projections. For each administrative division (county, county equivalent, and municipality), population density was calculated using the latest projected or census population.
COVID-19 cases and deaths attributed to COVID-19
Population-level analysis—United States
A total of 3,108 U.S. counties or county equivalents were initially eligible. Those with missing information on cases or deaths were excluded from analysis (n = 882). Counties with zero deaths reported were also excluded (n = 1,210). We used this approach to minimize possible underreport of deaths and have a fair comparison of COVID-19 mortality rates across counties. Importantly, 1,207 out of 1,210 counties with zero deaths had <200 COVID-19 cases. Thus, the number of fatalities in theory could be as low as 0.5 (and, therefore, not yet detected), given that COVID-19 fatality rate appears to range between 0.25% and 3.0% globally (Wilson et al., 2020). Final analysis included 1,016 counties.
Population-level analysis—Mexico
A total of 1,159 municipalities of Mexico were initially eligible. Mexican municipalities with zero deaths reported were excluded (n = 592). All 592 municipalities with zero deaths had <48 cases of COVID-19. Final analysis included 567 municipalities.
Individual-level analysis—Mexico
A total of 40,186 confirmed cases of COVID-19 were initially eligible. Cases with missing information on residence location (state or municipality, regardless the patient's migration status), pneumonia, requirement of endotracheal intubation, and intensive care unit (n = 18) were excluded. Final analysis included 40,168 cases.
Geographical elevation
For the purpose of this study, high altitude was defined as a geographical elevation ≥1,500 m (Woolcott et al., 2015). Altitude was grouped into three categories: 0–1,499, 1,500–1,999, and ≥2,000 m. Average elevation for each U.S. county and county equivalent was obtained from Zipcodes.com and validated using Google Earth (based on geographic coordinate system). Average elevation for each municipality of Mexico was obtained from the Instituto Nacional para el Federalismo y el Desarrollo Municipal or using Google Earth for missing data.
Statistical analyses
Data are presented as medians and interquartile ranges (IQR) unless otherwise indicated. Cases and deaths are presented as rates per 100,000 population. Kruskal–Wallis test (followed by post hoc analysis with Dunn's test with Bonferroni adjustment when appropriate) was used to compare variables across altitude categories. Wilcoxon rank-sum test was used to compare variables between survivors and nonsurvivors. Chi-squared test was used to compare proportions. In the Mexican population, multilevel mixed-effects Poisson regression analysis was used to estimate the relative risk of death attributed to COVID-19 (here calculated as the incidence rate ratio [IRR], with confidence intervals [95% CIs]) while accounting for nested data (states and municipalities) (Woolcott et al., 2016). The relative risk of death attributed to COVID-19 was adjusted for age, gender, medical history of diabetes, chronic obstructive pulmonary disease (COPD), cardiovascular disease, hypertension, obesity, and chronic kidney disease, and population density of residence location. We also evaluated the relative risk of pneumonia and requirement for endotracheal intubation as indicators of the severity of COVID-19. Since old age and male gender are risk factors linked to COVID-19 mortality (Li et al., 2020; Vincent and Taccone, 2020), we tested for a possible interaction between age and altitude and between gender and altitude on the regression models for mortality, pneumonia, and endotracheal intubation. A p-value <0.05 was considered statistically significant. All analyses were performed using Stata 14 (StataCorp LP, TX).
Results
Characteristics of the counties of the United States and municipalities of Mexico are provided in Tables 1 and 2, respectively.
Characteristics of U.S. Counties by Altitude
Projected population for 2019 by the U.S. Census Bureau.
Estimates were obtained from the total cumulative number of COVID-19 cases and the total cumulative number of deaths attributed to COVID-19 between January 20 and April 13, 2020, in counties or county equivalents of mainland United States.
IQR, interquartile range.
Characteristics of Municipalities of Mexico by Altitude
Data from latest projected population or latest censuses.
Estimates were obtained from the total cumulative number of COVID-19 cases and the total cumulative number of deaths attributed to COVID-19 between March 13 and May 13, 2020.
Population-level analysis—United States
The total cumulative number of COVID-19 cases was significantly higher in U.S. counties with a mean elevation ≥2,000 m than in those <1,500 m (176.3 vs. 67.2 per 100,000; p = 0.023) (Fig. 1A). COVID-19 mortality rates were also higher in counties at ≥2,000 m than in those <1,500 m (12.3 vs. 3.2 per 100,000; p < 0.001) (Fig. 1B). Since exclusion of counties with zero deaths could lead to biased estimates, we performed a sensitivity analysis including counties with zero and nonzero deaths (n = 2,637). The total cumulative number of COVID-19 cases was significantly higher in counties with a mean elevation ≥2,000 m than in those <1,500 m (49.9 vs. 36.8 per 100,000 population; p = 0.010). However, the median of COVID-19 mortality rates was zero in all altitude categories (p = 1.00) due to a higher number of counties with zero deaths than counties with nonzero deaths in all altitude categories (data not shown).
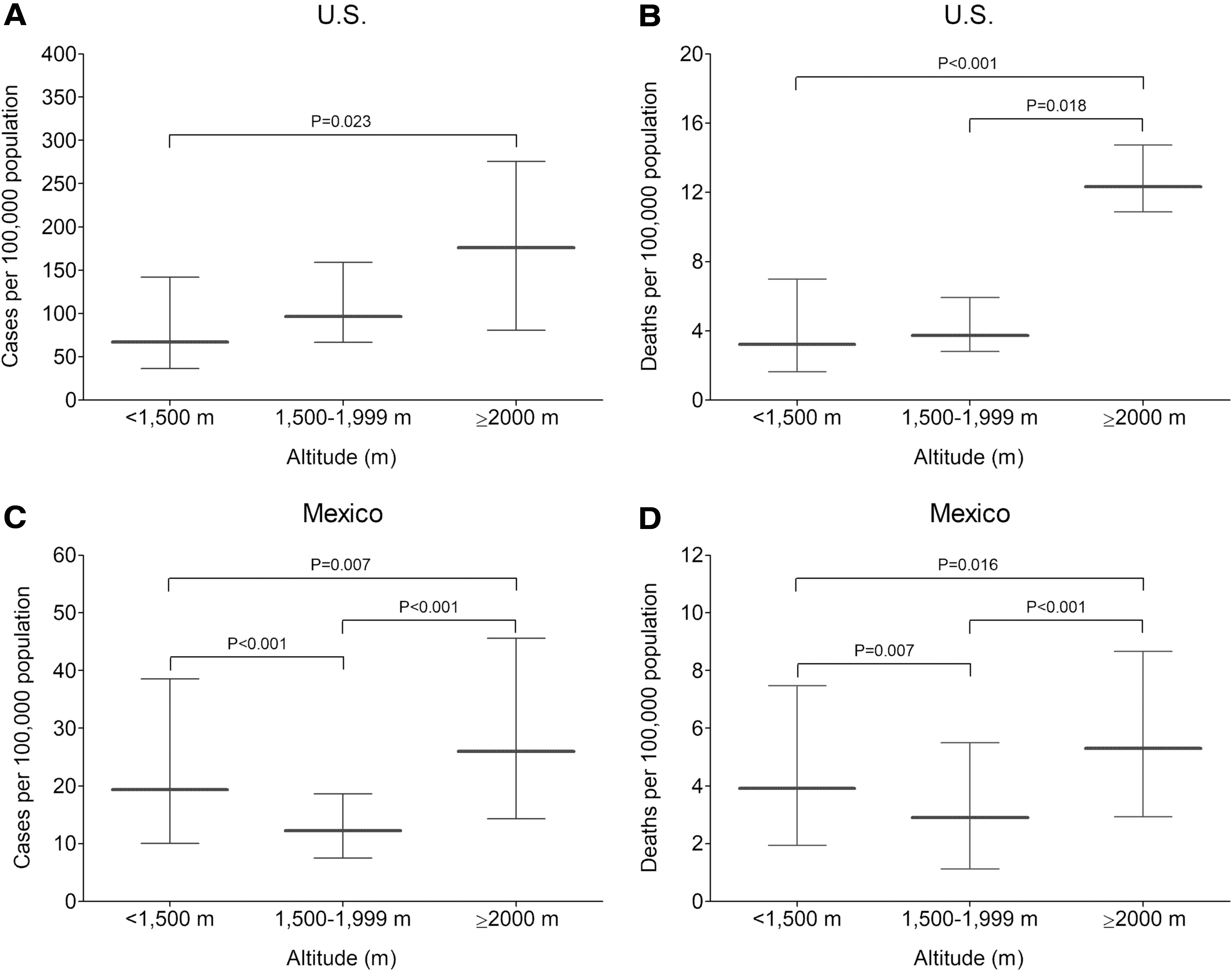
Total cumulative number of cases of COVID-19 and mortality rate attributed to COVID-19 in populations located at different altitudes.
Population-level analysis—Mexico
The total cumulative number of COVID-19 cases was significantly higher in Mexican municipalities with a mean elevation ≥2,000 m than in those <1,500 m (26.0 vs. 19.4 per 100,000; p = 0.007) (Fig. 1C). The mortality rates were also higher in municipalities located at ≥2,000 m than in those <1,500 m (5.3 vs. 3.9 per 100,000; p < 0.001) (Fig. 1D). Our sensitivity analysis including municipalities with zero and nonzero deaths (n = 1,159) showed the total cumulative number of COVID-19 cases was significantly higher in those with a mean elevation ≥2,000 m than in those <1,500 m (20.9 vs. 13.5 per 100,000 population; p < 0.001). The median of COVID-19 mortality rates was higher in municipalities with a mean elevation ≥2,000 m than in those <1,500 m (2.0 vs. 0.0 per 100,000 population; p < 0.001).
Individual-level analysis—Mexico
Overall, COVID-19 patients living at ≥2,000 m were only marginally older than those living <1,500 m. However, endotracheal intubation was considerably more common in those living at ≥2,000 m. Likewise, pneumonia and COPD were more common above 2,000 m, whereas hypertension and diabetes were less common (Table 3). Among fatal cases, endotracheal intubation was considerably more common in those living at ≥2,000 m. Likewise, male gender, pneumonia, and COPD were more common above 2,000 m. In contrast, hypertension, cardiovascular disease, and diabetes were less common above 2,000 m (Supplementary Appendix Table S1). Characteristics of COVID-19 cases by survival status are provided in Supplementary Appendix Table S2.
Characteristics of Mexican Subjects with COVID-19
p-Values obtained with the use of the Dunn's (rank-sum) test with Bonferroni adjustment.
COPD, chronic obstructive pulmonary disease; ICU, intensive care unit; IQR, interquartile range.
COVID-19 patients 65 years of age and older had a higher risk of death (adjusted IRR: 2.59; 95% CI, 2.42–2.78; p < 0.001) than COVID-19 patients younger than 65 years. Likewise, COVID-19 male patients had a higher risk of death than COVID-19 female patients (adjusted IRR: 1.55; 95% CI, 1.45–1.65; p < 0.001). We found a significant interaction between age and altitude and between gender and altitude on the association of altitude with pneumonia, requirement for endotracheal intubation, and mortality. Thus, we performed separate regression analyses for patients <65 years and for those ≥65 years of age. Likewise, we performed separate regression analyses for women and men.
Among patients younger than 65 years, those who were living at ≥2,000 m (including residents and foreign residents) had 24% higher risk of pneumonia than those who were living below 1,500 m (adjusted IRR: 1.24; 95% CI, 1.00–1.53; p = 0.044) adjusting for age, gender, pre-existing comorbidities, and population density of residence location (Fig. 2A). The requirement for endotracheal intubation was 78% higher at ≥2,000 m compared with that at <1,500 m (adjusted IRR: 1.78; 95% CI, 1.15–2.76; p = 0.010) (Fig. 2B). Likewise, the risk of death attributed to COVID-19 was 36% higher at ≥2,000 m than at <1,500 m (adjusted IRR: 1.36; 95% CI, 1.05–1.78; p = 0.022) (Fig. 2C). Among patients 65 years of age and older, we found no differences in the risk of pneumonia (p = 0.79), the requirement for endotracheal intubation (p = 0.12), or the risk of death (p = 0.11) between those who were living at ≥2,000 m and those who were living below 1,500 m (Fig. 2).
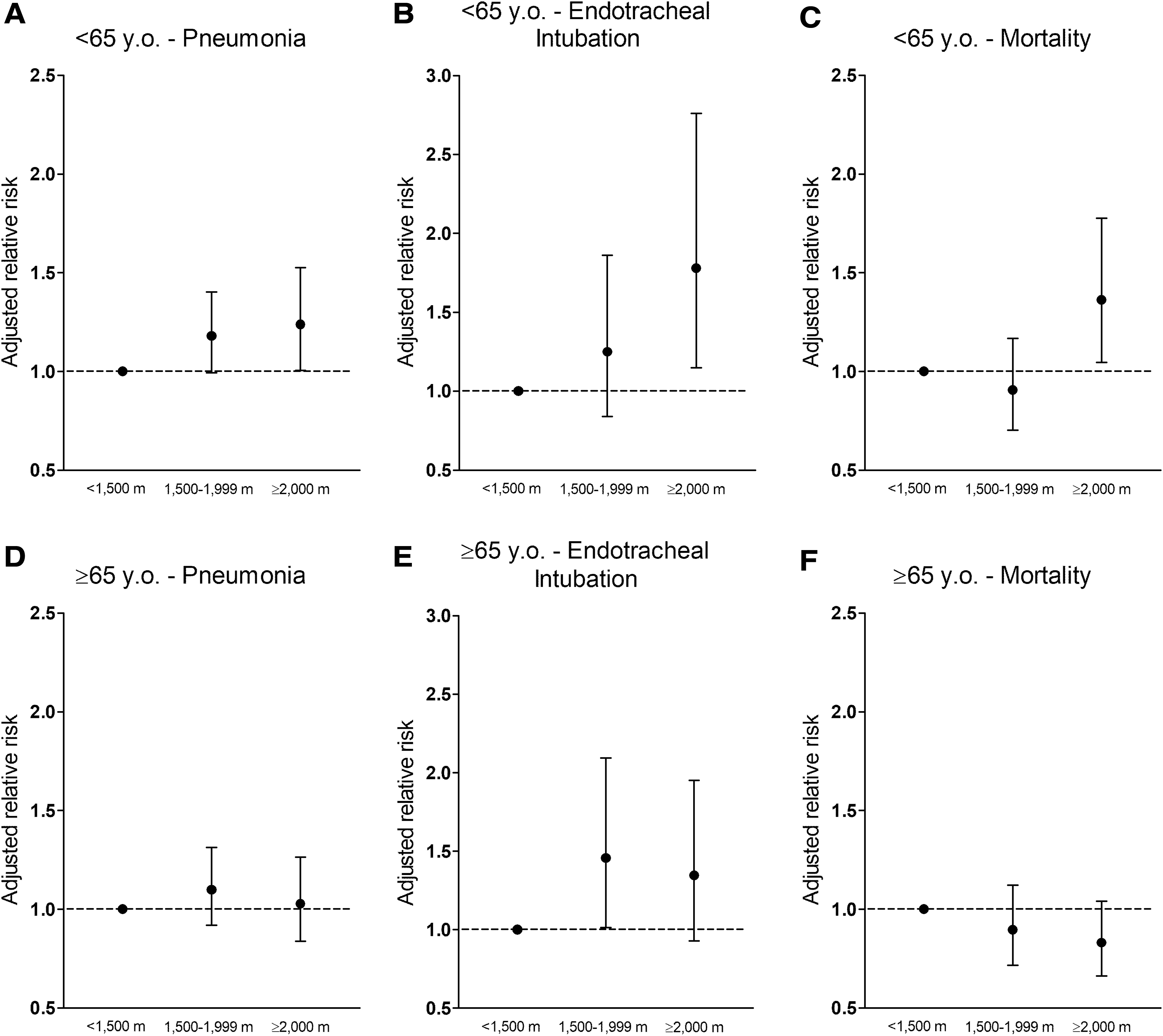
Association between COVID-19 outcomes and altitude categories in Mexican subjects with COVID-19 (n = 40,168). Upper panels show the adjusted relative risk (IRR) of pneumonia
Among women, we found no differences in the risk of pneumonia (p = 0.56), the requirement for endotracheal intubation (p = 0.10), or the risk of death (p = 0.20) between low and high altitude (Supplementary Appendix Fig. S1). In contrast, among men, those who were living at ≥2,000 m had 28% higher risk of pneumonia than those who were living <1,500 m (adjusted IRR: 1.28; 95% CI, 1.05–1.56; p = 0.016). The requirement for endotracheal intubation was 56% higher at ≥2,000 m than at <1,500 m (adjusted IRR: 1.56; 95% CI, 1.05–2.31; p = 0.028). Likewise, the risk of death attributed to COVID-19 was 31% higher at ≥2,000 m than at <1,500 m (adjusted IRR: 1.31; 95% CI, 1.03–1.66; p = 0.025) (Supplementary Appendix Fig. S1).
Discussion
We found a higher cumulative incidence of COVID-19 cases and higher mortality rates attributed to COVID-19 in populations with a mean altitude ≥2,000 m than in those with a mean altitude <1,500 m, both in the United States and in Mexico (Fig. 1). The differences in the cumulative incidence rates between low- and high-altitude counties may not be seen when the analysis is performed by states as geographical elevation will lose resolution.
Our regression analyses suggest that COVID-19 patients younger than 65 years who live >2,000 m have a 36% higher adjusted relative risk of death than those who live below 1,500 m (Fig. 2). Likewise, COVID-19 patients younger than 65 years have a more severe clinical manifestation >2,000 m, as indicated by a higher requirement for endotracheal intubation and a higher risk of pneumonia. This was not seen in older COVID-19 patients. Men, but not women, also have a 31% higher adjusted relative risk of death and a higher risk of severe clinical manifestation >2,000 m. It is unclear why the association between altitude and COVID-19 outcomes was significant in the younger population and in men only. This aspect requires further investigation. Our findings showed that older age and male gender were associated with increased COVID-19 mortality, consistent with findings from previous studies (Cummings et al., 2020; Parohan et al., 2020; Segovia-Juarez et al., 2020; Yu et al., 2020). One possible explanation for the lack of association between COVID-19 mortality and altitude among patients 65 years of age and older is that altitude may not further increase the already high risk of COVID-19 mortality in old patients.
The findings of this study must be interpreted cautiously. Severe hypoxemia and coagulopathy are more common in more severe cases of COVID-19 (Chen et al., 2020; Connors and Levy, 2020). Since chronic environmental hypoxia may aggravate lung disease (Stream et al., 2009) and promote hypercoagulability (Kicken et al., 2018), it is plausible that high-altitude hypoxia could contribute to the higher COVID-19 mortality and the severity of COVID-19 in some susceptible individuals, as suggested by our findings. However, our data cannot prove causality. Thus, other possible explanations should also be considered.
Certainly, possible differences in the number of imported cases (e.g., ski tourists and new migrants), population density, and public containment measures across regions could explain, at least in part, the higher cumulative incidence of COVID-19 cases in high-altitude populations. Anecdotal reports of a number of tourists with COVID-19 in Colorado ski resorts suggest that imported cases could represent a confounder in our estimates of COVID-19 cases in the United States but would be less relevant in Mexico. However, these factors probably would play a less important role in explaining the higher COVID-19 mortality and the severity of the disease at higher elevations. Since official information on the migration status of COVID-19 cases in the United States was not available, the possible role of imported cases to explain the higher incidence of COVID-19, and probably mortality, remains speculative.
Numerous factors are linked to COVID-19 mortality including old age, pre-existing comorbidities, limited available health care resources (Vincent and Taccone, 2020) (including number of beds, lack of intensive care units, equipment, and personnel), and reduced accessibility to health care, all of which could explain the higher mortality above 2,000 m. A strength of our study is that we used a mixed-model regression analysis in a large population of COVID-19 patients to examine the association between altitude and COVID-19 outcomes adjusting for age, gender, and major pre-existing comorbidities, while controlling for nested data. However, we cannot rule out the possible contribution of other unaccounted factors including other comorbidities (e.g., coagulopathies, cancer, and immunodeficiency) and ethnic/genetic differences. A recent study in the Province of Sichuan, China (Kong et al., 2020), showed a higher proportion of asymptomatic COVID-19 cases in populations located >3,000 m than in those located at lower altitudes (∼500–2,000 m). The authors suggest that asymptomatic cases may increase the likelihood of spreading the disease, although this possibility was not alluded specifically to high-altitude populations. Although this finding is interesting, from the data presented it is difficult to determine whether the incidence of cases between these two populations is different.
Additional factors to be considered are altitude-related environmental factors including ambient temperature, air pollution, radiation, and humidity (Woolcott et al., 2015), all of which have been associated with the transmission of SARS-CoV-2 (Liu et al., 2020). Although experimental studies have clearly shown that radiation may lower SARS-CoV-2 viability (Hessling et al., 2020), whether increased ambient radiation may play a significant role in the virus transmission, it still remains controversial (Yao et al., 2020). Conversely, the association between air pollution and COVID-19 incidence appears to be less controversial (Comunian et al., 2020). It has been argued that the lower air pollution at high altitude would contribute to the lower incidence of COVID-19 at high altitude (Arias-Reyes et al., 2020). However, we found a higher incidence of COVID-19 at high altitude. It should be noted that the biological mechanism underlying the association between air pollution and COVID-19 is still missing.
Our regression model was also adjusted for population density but not for health care resources (data unavailable). Information on migration status was also limited in our study population. Among those cases with known migration status (n = 139), the proportion of migrants >2,000 m was less than half of that <1,500 m.
Because we excluded counties and municipalities with zero deaths in our population-level analyses, our estimates do not represent national estimates of the total number of COVID-19 cases. The presence of zero deaths is a known problem when comparing estimates of mortality rates across populations. Different approaches (CDC, 2020; Ponnambalam et al., 2012; Dwyer-Lindgren et al., 2018; Shiels et al., 2019), including elimination of populations with fewer than 10 deaths (Ponnambalam et al., 2012; Shiels et al., 2019), have been used to circumvent this issue. All these methods are not exempt of error but are valid approaches for better comparison of mortality rates across populations. In our study, the excluded counties and municipalities contributed little to the total number of COVID-19 cases in the United States and Mexico (Supplementary Appendix Table S3).
Another limitation of this study includes possible misreport of COVID-19 cases and deaths. Underreporting of COVID-19 is a global problem (Krantz and Rao, 2020) as the number of cases largely depends on the number of tests performed and the type of test used. This can introduce bias when comparing incidence rates across populations and overestimate or underestimate the total number of deaths attributed to COVID-19. Likewise, it is possible that the number of reported deaths attributed to COVID-19 does not accurately represent the total fatal cases. Deaths occurring in nursing homes or private residences could be underreported.
Conclusions
In the United States and Mexico, populations located at an altitude above 2,000 m have a higher total cumulative number of COVID-19 cases and a higher mortality rate attributed to COVID-19 than those located below 1500 m. Among Mexican subjects with COVID-19, altitude is associated with COVID-19 mortality in men younger than 65 years. Our findings provide new information calling for careful re-examination of public health policies on COVID-19 prevention and deployment of health care resources for COVID-19 treatment to high-altitude populations.
Note in Proof
After submission of the revised version of this article, we became aware of a recent thorough review on the possible factors associated with SARS-CoV-2 transmission at high altitude by Pun et al., 2020.
Authorship Confirmation Statement
O.O.W. carried out study design, data collection, statistical analyses, data interpretation, and final draft writing. R.N.B. was involved in study design, data interpretation, and final draft writing. O.O.W. and R.N.B. have reviewed and approved the article before submission.
Footnotes
Acknowledgments
Author Disclosure Statement
O.O.W. has no competing financial interests. R.N.B. received grants from the NIH (DK7619 and DK29867).
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.