
Abstract
Purpose:
This study aimed to assess the effects of modern board games (MBG) on executive functions, quality of life, and volitional behaviors in elderly individuals residing in nursing homes.
Methods:
A 12-week randomized controlled trial was conducted in a nursing home with 30 participants (age = 83.2 years). Participants were randomly assigned to either the experimental group (EG; n = 16) or the control group (CG; n = 14). The EG engaged in twice-weekly MBG sessions facilitated by trained professionals, while the CG continued with their usual activities without additional interventions. Cognitive performance was assessed using the Cambridge Cognitive Examination (CAMCOG-R) and the Test of the Paths (TESEN). Quality of life was evaluated using the FUMAT scale, and volitional behaviors were measured using the Volitional Questionnaire.
Results:
The EG demonstrated significant improvements in executive functions, including comprehension (9.9%, P < 0.05), remote memory (22.6%, P < 0.05), and attention and calculation (83.3%, P < 0.05), as measured by the CAMCOG-R. No significant changes were observed in the TESEN test. The EG also showed significant gains in quality of life, with improvements in emotional well-being (5.0%, P < 0.01), interpersonal relationships (15.4%, P < 0.05), personal development (7.5%, P < 0.001), and social inclusion (6.3%, P < 0.001) on the FUMAT scale. Volitional behaviors, particularly competence (7.1%, P < 0.05), also improved significantly in the EG.
Conclusion:
MBG offer a promising nonpharmacological intervention to enhance executive functions, quality of life, and volitional behaviors in elderly individuals in nursing homes. The structured facilitation of these games, tailored to participants’ cognitive levels, may support cognitive stimulation and foster social engagement in this population.
Keywords
Introduction
Board games have garnered increasing attention as beneficial activities for older adults, particularly in the context of cognitive decline prevention and the enhancement of social engagement.1,2 The cognitive demands required by many traditional board games stimulate multiple cognitive functions, including memory, attention, and executive functions, which are areas particularly vulnerable to aging. 3 Previous randomized controlled trials (RCTs) involving elderly populations have shown that games like chess, Go, or card games improve verbal fluency and memory.4–7 Additionally, board games promote social interaction, which is a critical aspect of cognitive interventions, as they support verbal communication and the maintenance of cognitive engagement in daily life. 8 The combination of these factors suggests that traditional board games serve as an effective tool for cognitive training and social enrichment among older adults, thereby enhancing their overall quality of life and well-being.
In Spain, older people have a long custom of playing traditional board games (e.g., dominoes, parcheesi, and goose) and card games (brisca and tute). 9 These games depend mainly on chance rather than on the skill of the players. In addition, in many of these games, there is little or no interaction between players. On the contrary, modern board games (MBG) differ significantly in several key aspects that may provide unique cognitive and social benefits. First, MBG tend to rely less on chance, emphasizing strategic decision-making and long-term planning, which can better engage cognitive processes like executive function and problem-solving. Additionally, many MBG are more thematic and immersive, often involving elaborate storylines and detailed environments, which can enhance engagement and memory retention through narrative-driven gameplay. Furthermore, the mechanics of MBG are typically more complex, involving multiple phases of gameplay and requiring players to make a greater number of decisions, thereby offering continuous cognitive challenges. Unlike traditional games that are often strictly competitive, many MBG are also collaborative, encouraging greater face-to-face interactions and teamwork among players, which fosters communication and cooperation, essential components for cognitive health and emotional well-being in older adults. 10
In Spain, it is very common for many older people to live in nursing homes, either because they do not have family members or because they are unable to care for themselves. This aging population often faces a significant decline in cognitive capacity and executive functions, which can severely impact their quality of life. Executive functions, including problem-solving, planning, working memory, and cognitive flexibility, are particularly vulnerable to the aging process. 11 This decline can manifest in difficulties with daily activities such as managing schedules, following multistep tasks, or adapting to new situations, which compromises the autonomy and well-being of the residents. 12 In addition, cognitive impairments often contribute to a greater sense of social isolation, reduced participation in communal activities, and an overall decrease in mental stimulation, which can accelerate the decline of both cognitive and emotional health. 13 Furthermore, nursing home environments may not always provide adequate opportunities for cognitive engagement or social interaction, which exacerbates these problems. 14 Addressing these deficits with targeted interventions, like cognitive stimulation through engaging activities, is crucial to improving the cognitive and emotional health of elderly individuals in institutionalized settings.
MBG build on the established benefits of traditional games. This study explores how MBG interventions impact elderly individuals in institutionalized settings. The only study to date that has evaluated the effects of MBG on elderly populations through RCT demonstrated that MBG and card games can improve cognitive performance, particularly in executive functions such as verbal fluency and motor impulsivity control. 15 Additionally, this research highlighted the potential for these games to serve as a viable cognitive intervention in maintaining cognitive health in elderly individuals. Furthermore, different experts have proposed that MBG can support the development of executive functions. 16 Thus, the present study aims to build on this foundational work by extending the scope of the investigation to include a 12-week intervention with MBG, specifically assessing their effects on executive functions, quality of life, and volitional behavior in elderly nursing home residents. Our study not only seeks to confirm the cognitive benefits observed in prior research but also to explore the broader impact of such interventions on the well-being and autonomy of the elderly population.
Methods
Participants
The study was conducted in a nursing home under the jurisdiction of the Provincial Council of Valladolid. Following discussions with the center’s social educator and director, a list of 30 residents was provided who met the inclusion criteria of being able to read, write, and engage in conversation. These 30 were all possible among the total residents. After the study objectives were explained to the residents, all agreed to voluntarily participate and provided written informed consent. Participants were then randomly assigned to one of two groups (Fig. 1): the experimental group (EG, n = 16; 8 males, 8 females; age = 83.2 ± 9.4 years) and the control group (CG, n = 14; 5 males, 9 females; age = 83.2 ± 8.9 years). Randomization was performed using the Statistical Package for the Social Sciences (SPSS), where participants were randomly allocated to each group with the constraint of maintaining 16 participants in the EG and 14 in the CG. The study received approval from the Research Ethics Committee of the European University Miguel de Cervantes on January 11, 2024 (Report 15/2024) and was conducted in accordance with the Declaration of Helsinki. The study was registered on ClinicalTrials.gov on March 12, 2024 (NCT06306365). Subject recruitment commenced on March 18, 2024.
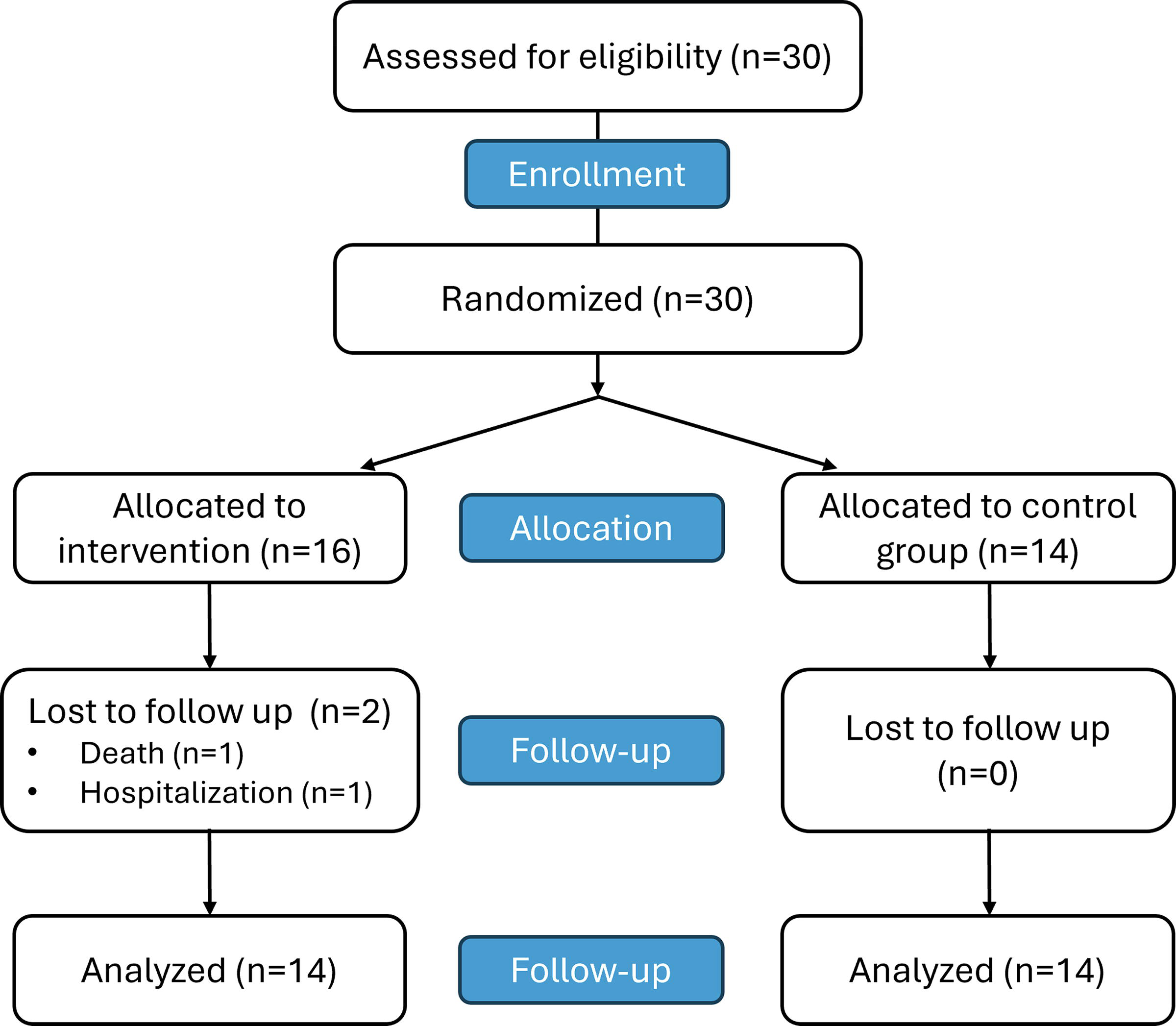
CONSORT flow diagram. Consort diagram of patients eligible, recruited, and numbers followed up and included in analysis.
Design
This study is a randomized clinical trial with a CG. A team of four psychologists, who were experts in administering the questionnaires used to measure the dependent variables, evaluated all participants. Assessments were conducted one week before and one week following the intervention. The psychologists were blinded to the participants’ group allocation (EG or CG) during the assessments. The independent variables included group (EG vs. CG) and time (preintervention vs. postintervention).
Over the 12-week study period, four facilitators, each experienced in board games and the specific methodology employed, conducted 90-minute sessions twice weekly (on Mondays and Thursdays) at the center. The 12-week duration was selected based on previous research indicating that this period is sufficient to induce measurable changes in executive functions. 6 Each facilitator worked with a fixed group of—three to four participants. Groups were formed based on initial cognitive assessments and social compatibility, ensuring a mix of abilities to promote peer learning and social interaction. Although initial plans included rotating group members, residents requested that the groups remain consistent throughout the study, resulting in each facilitator working with the same group of participants for the duration of the study. During each session, all subgroups played the same games to ensure consistency in the intervention.
Board games
In one of our previous studies, 17 a panel of six experts in board games, each with substantial experience (18.3 ± 4.1 years) in applying these games to various demographic groups, conducted an initial selection of 29 MBG potentially suitable for cognitive stimulation in older adults. Following a two-month trial conducted at another nursing home (Cardenal Marcelo, Valladolid, Spain) involving 16 residents, 18 games were selected that were understandable and easily usable by the elderly. These 18 games, including Unanimo party, Quick cups, 3·4 = Klatsch!, Blurble, Fauna, Pelusas, Pickomino, Point salad, Bee alert, Connecto, Spot it!, Ubongo, The Curse of the Maldita Diamond, Just one, Stotytelling, Kaleidos, Taboo: Kids vs. Parents, and Guess in 10 Junior: Animal Kingdom, were subsequently utilized in the current project. Further information on the 18 board games used in this study, including their design details and variations across regions, can be found on the Board Game Geek website: https://boardgamegeek.com. In the present study, participants were introduced to all board games for the first time during the intervention. Each game was employed at least twice across 24 sessions. Each session included two to three different board games, depending on the complexity and engagement level of the participants (Table 1). Additionally, a pedagogical sheet was developed for each game, which encompassed not only the fundamental information about the game but also included variations, adaptations (e.g., simplifying rules and/or reducing game complexity), and reflective activities to engage participants after gameplay. The facilitators received comprehensive training to master the rules, mechanics, and adaptations outlined in the pedagogical sheets, enabling them to effectively guide participants through the games and maximize engagement and cognitive stimulation during the sessions.
Board Games Used During the 12 Weeks of Intervention
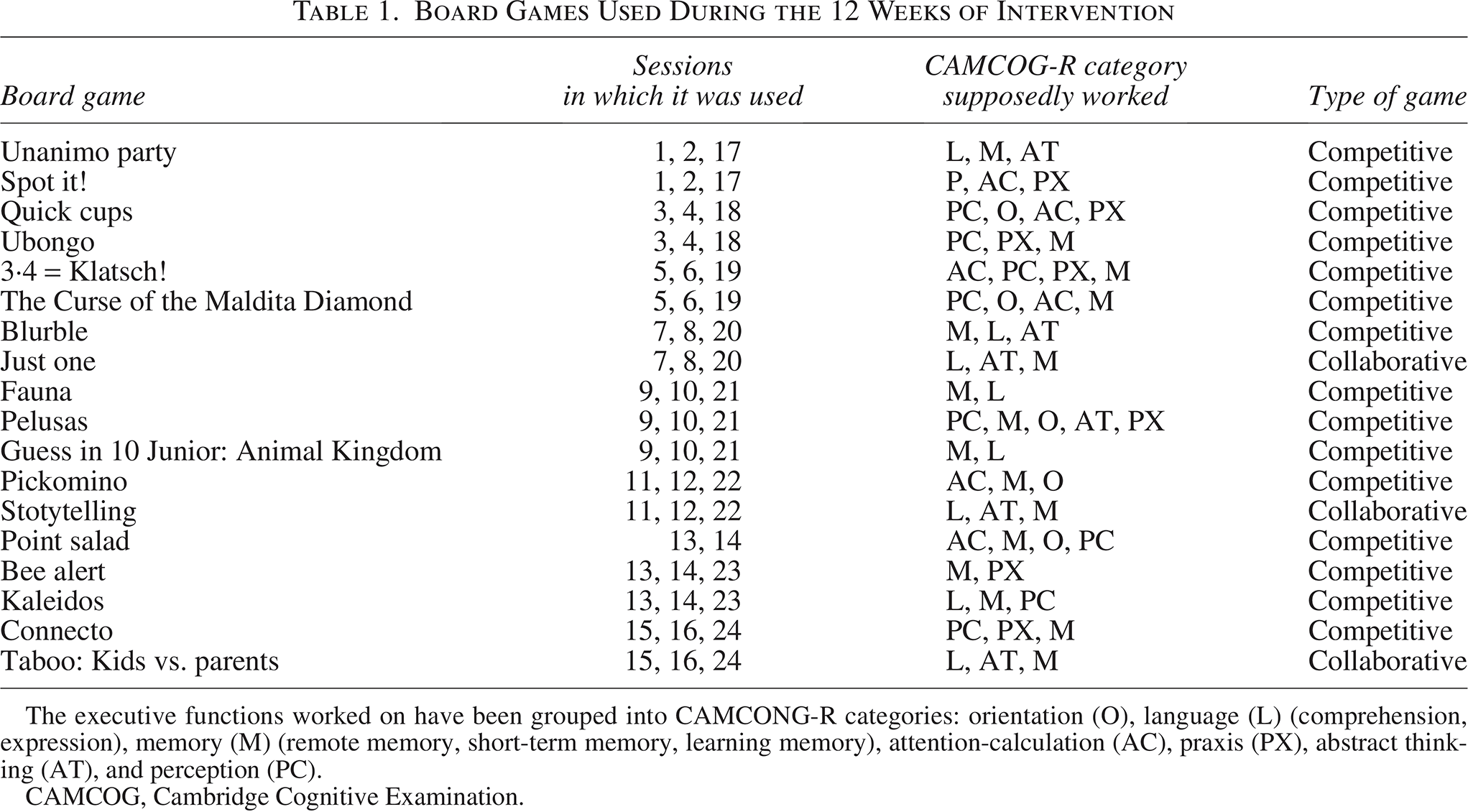
The executive functions worked on have been grouped into CAMCONG-R categories: orientation (O), language (L) (comprehension, expression), memory (M) (remote memory, short-term memory, learning memory), attention-calculation (AC), praxis (PX), abstract thinking (AT), and perception (PC).
CAMCOG, Cambridge Cognitive Examination.
Executive functions assessment
The Cambridge Cognitive Examination (CAMCOG-R), 18 a comprehensive neuropsychological assessment tool designed to evaluate cognitive function in older adults, was used. It corresponds to Section B of the CAMDEX-R 19 (Revised Cambridge Examination for Mental Disorders of the Elderly) and is specifically structured to assess multiple cognitive domains. It consists of 67 items that cover a wide range of cognitive domains, including orientation, language comprehension and expression, memory (both recent and remote), attention, praxis, calculation, abstraction, and perception. A trained psychologist, through a structured interview, administered the CAMCOG-R. The examiner asked the participant to perform a series of tasks that corresponded to each cognitive domain. The test was conducted in a quiet environment to minimize distractions, ensuring that the participant was able to fully concentrate on the tasks. The examiner scored each item based on the participant’s performance, with higher scores indicating better cognitive function. Depending on the participant, application time ranged between 30 and 45 minutes.
The Test of the Paths (Test de los Senderos, TESEN) 20 is a screening test for individual application to evaluate the executive functioning of young people and adults through a visual-motor planning task. In the test, participants are required to complete four distinct path-drawing tasks. Task 1, connect the numbers 1 to 25 in ascending order. Task 2, connect the numbers 25 to 1 in descending order. Task 3, connect the numbers 1 to 20 in ascending order, alternating between two colors (yellow–blue–yellow…). Task 4, connect the numbers 1 to 20 in ascending order, alternating between two shapes (circle–square–circle…). For each task, the following metrics are recorded: execution time or speed (time taken to complete each path, measured in seconds); accuracy (number of correct connections [hits]); and the number of errors made. The following derived variables were calculated: precision ([hits − errors]/hits*100); execution efficiency ([hits − errors]/time*100). These variables were computed separately for each path. The total score for the test was derived by summing the scores across all four tasks. The test was conducted under the same conditions as the CAMCOG-R and by the same evaluator. Application time ranged between 12 and 104 minutes, since the test does not impose a specific time limit for task completion, allowing participants to progress at their own pace. Eighteen of the participants had to complete this test on a second day due to the difficulties they had with the first path. This flexibility accommodates the diverse range of cognitive and motor abilities observed within the EG.
Functional assessment tool
The FUMAT scale 21 was used to assess the quality of life in users of social services, as the participants of this study. The FUMAT scale was presented to participants in a structured interview format to ensure comprehension and accuracy in responses, given the age-related variability in cognitive and sensory abilities. The interviewer guided each participant through the questionnaire, reading the items aloud and providing clarification when necessary. This approach minimized potential biases due to literacy levels or visual impairments. From the original eight dimensions of the questionnaire, only four were selected for inclusion in this study. These dimensions were chosen based on their potential to be positively influenced through interventions involving MBG. The selected dimensions were emotional well-being (8 items), interpersonal relationships (6 items), personal development (8 items), and social inclusion (9 items). Each item was rated on a Likert scale (from 1 to 4), with responses reflecting the degree to which participants agreed or disagreed with the statements provided. As the scale requires administration by a social services professional who has been familiar with the participants for a minimum of three months, it was administered by the center’s social educator, who had established ongoing relationships with the participants. The administration of the scale took approximately 20–30 minutes per participant, depending on the individual’s pace and need for clarification.
Volition assessment
The Volitional Questionnaire 22 was utilized in this study to assess the volitional behaviors of elderly participants, specifically focusing on their motivation, decision-making, and persistence during tasks. The center’s social educator administered the test through direct observation. The assessment was conducted during routine activities within the care setting, allowing for a naturalistic evaluation of volitional behaviors. This professional observed the participants as they engaged in various tasks, such as social interactions, recreational activities, and daily living routines. During the observation, he recorded participants’ responses to challenging situations, their ability to initiate and sustain actions, and their level of engagement in the activities. The questionnaire items were rated on a standardized scale, capturing the degree of volitional behaviors exhibited. The collected data were used to derive scores for each volitional domain: exploration (5 items), competence (5 items), and achievement (4 items). Each item was assessed on a Likert scale as passive, doubtful, involved, or spontaneous.
Statistical analysis
The data were recorded in the Microsoft Excel spreadsheet, where all dimensions were calculated. They were subsequently analyzed statistically with the SPSS program for Windows. The normality of the data was checked with the Shapiro–Wilk test. In the variables in which normality was observed, a repeated measures analysis of variance (ANOVA) was applied. When the F-statistic was significant, Bonferroni pairwise comparisons were applied. When normality was not observed in the variables, pre- and postcomparisons were carried out with the Wilcoxon test and comparisons between groups with the Mann–Whitney U test. A significance level of 0.05 was used in all procedures. When the assumption of normality was met, the effect size was computed using the formula d = (M2 − M1)/SD1, where M2 and M1 represent the post- and preintervention means, respectively, and SD1 corresponds to the standard deviation of the preintervention measurement. In cases where normality was not observed, the effect size was calculated using the formula rb = z/n^0.5, where z is the Wilcoxon signed-rank test statistic and n denotes the sample size.
Results
Descriptive analyses
Of the 30 participants who initially enrolled in the study, one male and one female from the EG did not complete the study (Fig. 1). The male participant passed away a few days after the study commenced, and the female participant was hospitalized due to illness during the study. Both events were unrelated to the study. A t-test confirmed that the age distribution of the remaining participants was comparable between the EG and CG. The rate of attendance in the EG was 83.3%.
Executive functions assessment
Table 2 presents the variables recorded by the CAMCOG in both the EG and the CG at baseline and after the intervention. The EG demonstrated improvements in comprehension (9.9%, P < 0.05, d = 0.57), remote memory (22.6%, P < 0.05, d = 0.47), attention and calculation (83.3%, P < 0.05; rb = 0.60), and the overall questionnaire score (7.6%, P < 0.05, d = 0.32). In contrast, the CG exhibited no significant changes in any of the variables. Initial scores were comparable between the two groups; however, after 12 weeks, the remote memory scores in the CG were lower than those in the EG (−34.2%, P < 0.05, rb = 0.54).
Results Obtained in Each Dimension of CAMCOG
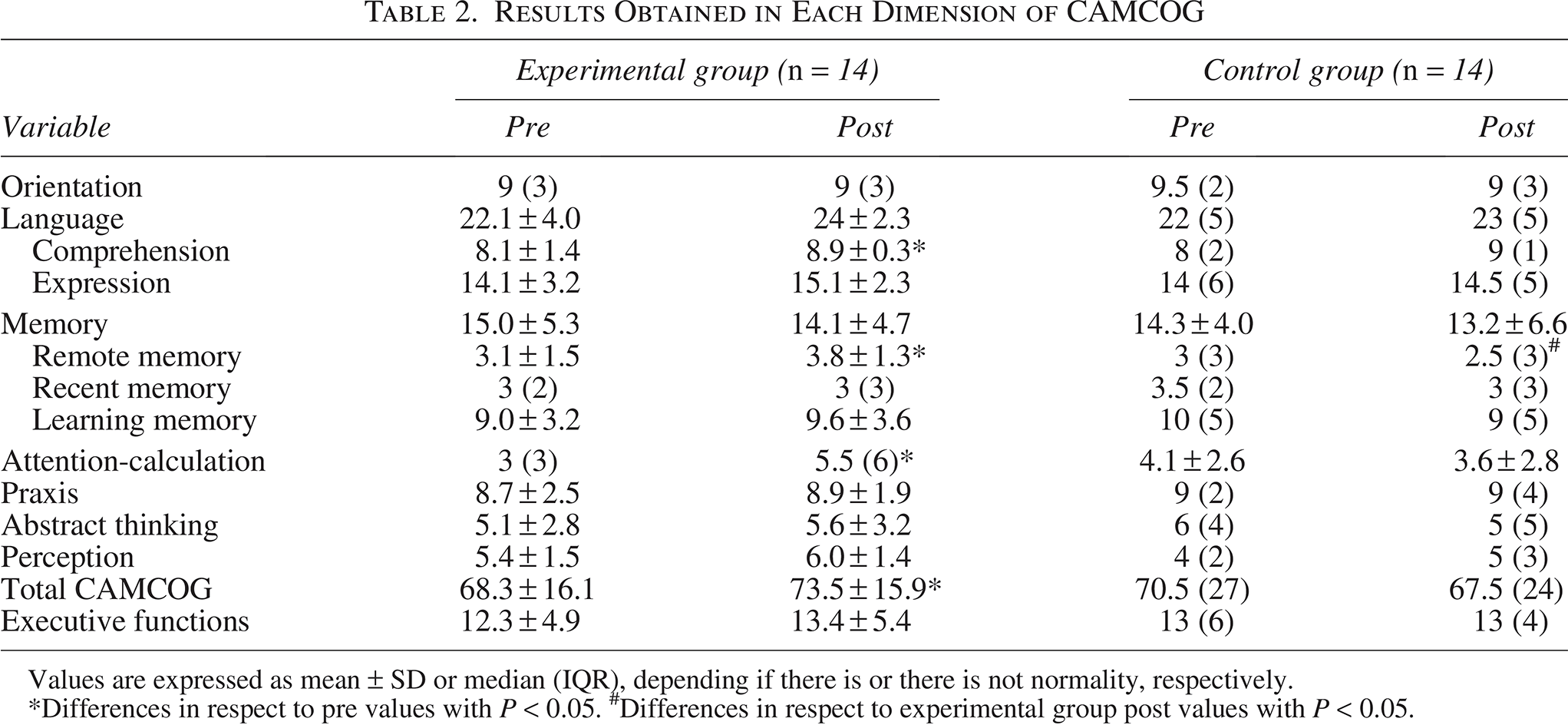
Values are expressed as mean ± SD or median (IQR), depending if there is or there is not normality, respectively.
*Differences in respect to pre values with P < 0.05. #Differences in respect to experimental group post values with P < 0.05.
Table 3 presents the TESEN results for both groups at baseline and postintervention. No significant differences were observed between the groups at either time point, nor were any significant changes detected within each group over time.
Results Obtained in Each Dimension of the TESEN
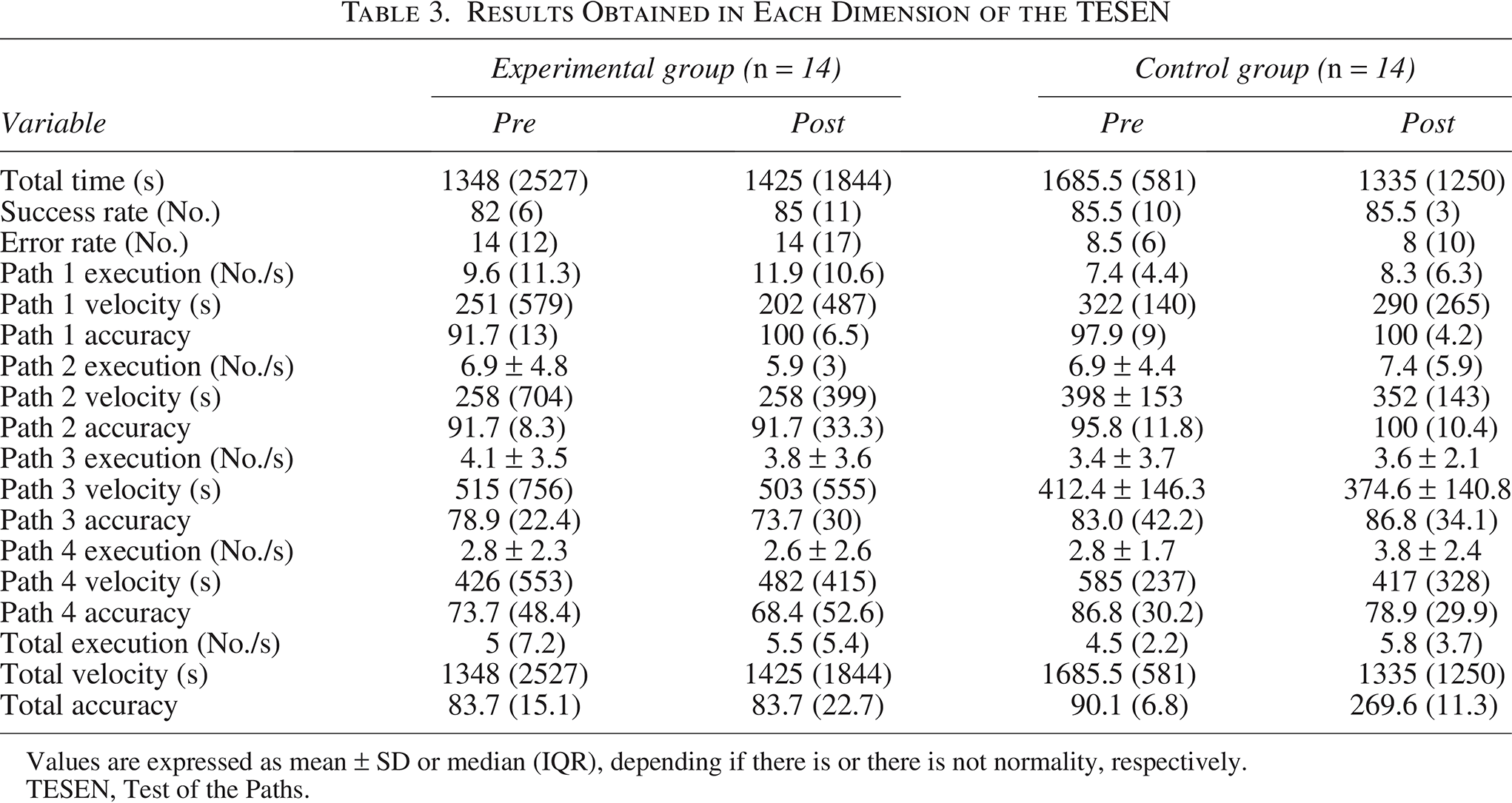
Values are expressed as mean ± SD or median (IQR), depending if there is or there is not normality, respectively.
TESEN, Test of the Paths.
Functional assessment tool
Table 4 presents the results obtained from the FUMAT scale. In the EG, all four variables showed significant increases: emotional well-being improved by 5.0% (P < 0.01, d = 0.30), interpersonal relationships by 15.4% (P < 0.05, rb = 0.60), personal development by 7.5% (P < 0.001, d = 0.43), and social inclusion by 6.3% (P < 0.001, d = 0.53). In the CG, an improvement in personal development was noted (P < 0.05, rb = 0.68); however, the increase was significantly greater in the EG compared to the CG (7.5 ± 7.1% vs. 2.2 ± 2.5%, P < 0.05, rb = 0.46).
Results Obtained in Each Dimension of the FUMAT Scale
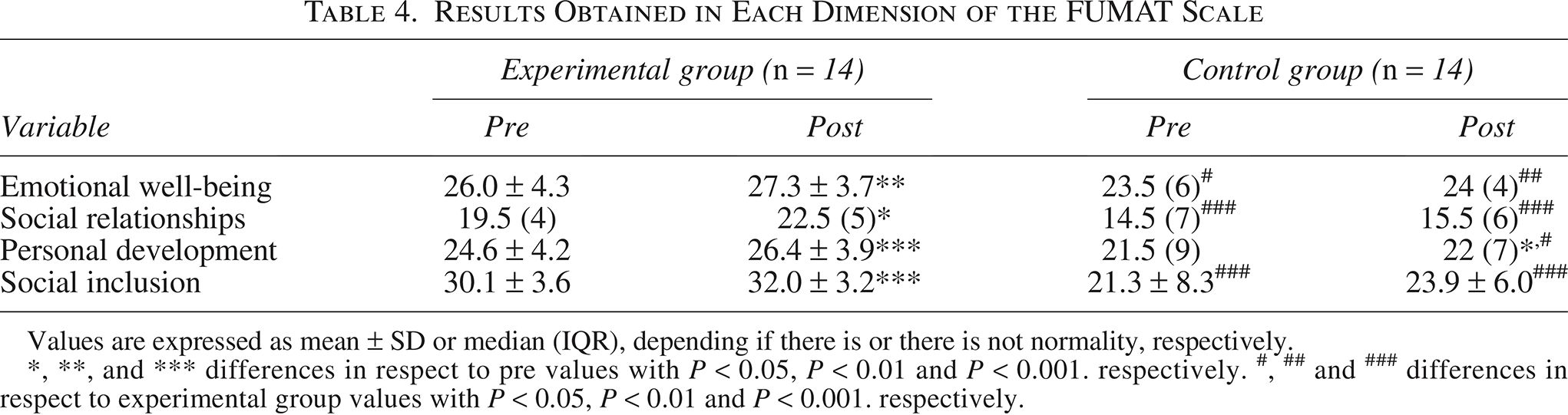
Values are expressed as mean ± SD or median (IQR), depending if there is or there is not normality, respectively.
*, **, and *** differences in respect to pre values with P < 0.05, P < 0.01 and P < 0.001. respectively. #, ## and ### differences in respect to experimental group values with P < 0.05, P < 0.01 and P < 0.001. respectively.
At baseline, despite random group assignment, the CG exhibited lower values than the EG in emotional well-being, interpersonal relationships, and social inclusion (Table 3). These differences persisted in the post-12-week assessment, with additional significant differences observed between the groups in personal development at this time point.
Volition assessment
Table 5 presents the values of the three variables analyzed in the Volitional Questionnaire. In the EG, a significant improvement in competence was observed (7.1%, P < 0.05, rb = 0.54). The CG showed a significant increase in exploration (7.7%, P < 0.05, rb = 0.66). Differences were noted between the EG and CG both at baseline and postintervention, with the EG consistently displaying higher values across all time points.
Results Obtained in Each Dimension of the Volitional Questionnaire
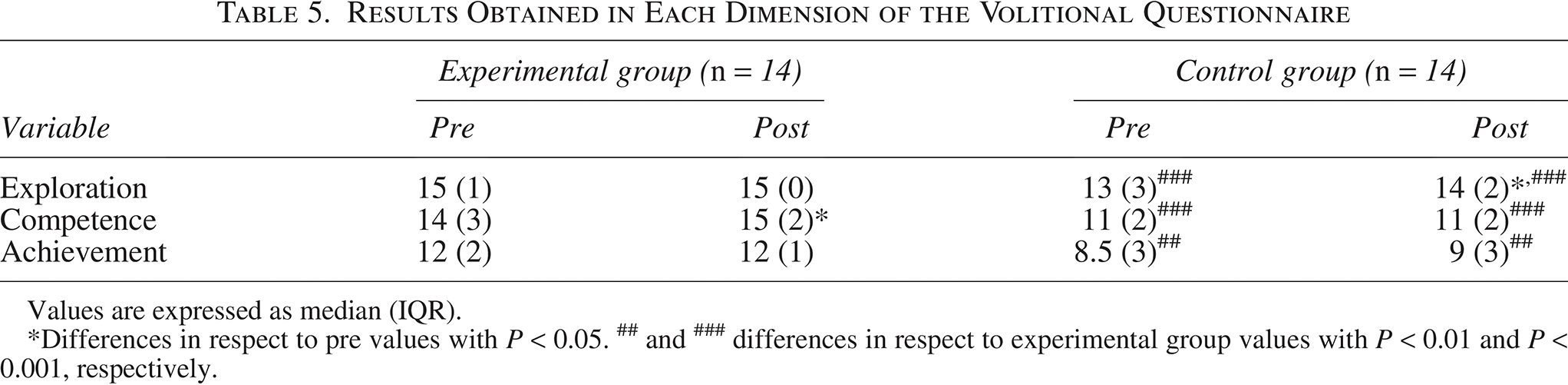
Values are expressed as median (IQR).
*Differences in respect to pre values with P < 0.05. ## and ### differences in respect to experimental group values with P < 0.01 and P < 0.001, respectively.
Discussion
The main findings of the present study showed notable enhancements after the MBG intervention in executive functions, particularly in comprehension, remote memory, attention, and overall cognitive performance, as measured by the CAMCOG-R. Additionally, the MBG sessions improved quality of life, with significant increases in emotional well-being, interpersonal relationships, personal development, and social inclusion. Volitional behaviors, specifically competence, also improved significantly after the game sessions.
The observed improvements in executive functions, as measured by the CAMCOG-R, are aligned with previous research that highlights the positive impact of MBG on cognitive functions, particularly executive functions such as verbal fluency and inhibitory control in the elderly. 15 Estrada-Plana et al. 15 observed significant improvements in these domains, which suggests that engaging elderly individuals in modern board game activities could serve as a viable strategy to slow cognitive decline in institutional settings. The findings of Miyake et al. 23 and Diamond 24 on the unity and diversity of executive functions suggest that various cognitive tasks may target different aspects of executive function. MBG, with their complex mechanics and immersive gameplay, may stimulate specific executive functions, such as shifting and inhibition, more effectively compared to traditional games that rely heavily on chance. Given the vulnerability of executive functions to aging,23,24 engaging older adults in cognitively stimulating activities becomes crucial. MBG, as proposed by Vita-Barrull et al., 16 offer a valuable opportunity to exercise these functions, particularly through strategic decision-making and problem-solving, which are often missing in traditional games. Furthermore, as demonstrated by Anguera et al., 25 immersive cognitive training using adaptive video games significantly enhances cognitive control in older adults, particularly in multitasking and sustained attention. These improvements in cognitive control suggest that similarly immersive MBG could also foster gains in executive functions, contributing to the maintenance of cognitive health in aging populations.
The lack of significant changes in motor impulsivity control or executive efficiency, as measured by the TESEN test, may be attributed to the task-specific nature of cognitive improvements. Previous studies highlighted that executive function gains may not generalize across different task modalities and are often dependent on the specific cognitive processes targeted by the intervention. 26 It is possible that the duration of our 12-week intervention was insufficient to produce significant changes in motor impulsivity control or executive efficiency. Previous research suggests that improvements in executive functions, such as cognitive control and multitasking abilities, often require more prolonged and intensive training to manifest in broader executive domains. 25 Finally, the complexity of motor impulsivity control may require more targeted interventions that focus specifically on motor skills and attention regulation. MBG, while cognitively engaging, may not sufficiently challenge the motor systems involved in impulsivity control. 27
The functional assessment results from the FUMAT scale in this study demonstrated significant improvements in the EG across all four measured dimensions—emotional well-being, interpersonal relationships, personal development, and social inclusion—following the 12-week intervention with MBG. These findings are consistent with previous research that highlights the role of structured social activities in improving the quality of life of elderly individuals. Our findings are in consonance with the work of Pardasani et al., 28 who demonstrated that board game interventions improve emotional well-being, social interaction, and cognitive engagement. FUMAT scale has also been sensible to demonstrate that multimodal interventions targeting cognitive and social dimensions significantly enhance the quality of life in elderly participants. 29 Chen et al., 30 who observed that MBG boost self-efficacy in older adults by encouraging open expression and fostering a sense of competence, support our findings of enhanced personal development. The use of MBG, through group interaction and emotional expression, can also enhance interpersonal communication and reduce loneliness in older adults.30,31 These improvements, observed in the FUMAT scale, underscore the holistic benefits that MBG can offer to older adults in institutional settings.
The results from the Volitional Questionnaire suggest that MBG can stimulate volitional behaviors in older adults. This aligns with broader research showing that volition and goal-directed behaviors are critical for maintaining autonomy and cognitive function in aging populations. 32 Volitional behaviors are deeply connected to cognitive stimulation. Engaging in board games requires older adults to sustain attention, make decisions, and persist through challenges, all of which can positively influence their motivation to continue participating in cognitively demanding tasks. 33 Our findings suggest that the intervention helped maintain or even improve these behaviors in the EG. An interesting finding was the increase in exploration observed in the CG. According to the social educator at the center, this may have been influenced by the EG discussing their experiences and the enjoyment they were having during the board game sessions with other residents during daily activities. This likely sparked curiosity among the CG participants, which may explain the improvement in exploration as measured by this dimension of the Volitional Questionnaire. The social interactions between the groups, although not part of the formal intervention, could have inadvertently stimulated a sense of curiosity and engagement in the CG.
The applied methodology in this intervention was not limited to merely playing MBG; it involved a well-structured approach to ensure the maximum benefit for the participants. The facilitators were thoroughly trained to master the rules and mechanics of each game, ensuring that the participants could fully engage in the cognitive and social elements that the games offered. This structured facilitation is critical, as previous studies have emphasized the importance of understanding the mechanics to effectively guide and engage participants in board game interventions. 34 Furthermore, each game was accompanied by an educational sheet that provided several essential adaptations to suit the cognitive levels of the elderly participants. This allowed facilitators to modify the rules when necessary and ensure that the games remained accessible, even for those experiencing cognitive decline. 35 In addition, the educational sheet contained a series of reflective questions designed to promote discussion after each session, with the last 10 minutes of each session dedicated to reflection on the gameplay and its real-life applications. Such debriefing processes are integral to the success of serious games, as they allow participants to process their experiences and draw connections to broader cognitive and social goals. 34 These considerations should be central to future applications of board games as cognitive interventions for older adults.
This study has several limitations that should be considered when interpreting the findings. First, the sample size was relatively small and limited to a single nursing home, which may affect the generalizability of the results to other elderly populations or care settings. Second, the duration of the intervention was only 12 weeks, which limits our ability to assess the long-term sustainability of the observed cognitive and emotional improvements. Another limitation of this study is that the social educator responsible for administering the volitional and quality of life assessments was aware of the group assignments. This was unavoidable given the specific requirements of the questionnaires, which necessitate a professional who knows the participants well and interacts with them regularly. While we relied on the professionalism and objectivity of this individual, we recognize that this knowledge could have introduced an element of bias. Likewise, the observed baseline differences between the EG and CG in certain volitional variables and functionality measures, despite the random group assignment, should be considered when interpreting the results. Finally, while the study focused on cognitive and volitional outcomes, it did not explore other potentially relevant factors such as physical health, mood disorders, or individual preferences for different types of games, aspects that could be the subject of future studies.
In conclusion, MBG offer a valuable intervention for improving cognitive function, quality of life, and volitional behaviors in elderly individuals living in nursing homes. Specifically, the significant improvements in executive functions, emotional well-being, interpersonal relationships, personal development, and social inclusion observed in the EG highlight the potential of MBG as an effective tool for cognitive stimulation and social engagement. The observed gains in volitional behaviors, particularly in competence, further support the notion that MBG can foster greater autonomy and motivation in older adults. Given these results, MBG represent a promising, nonpharmacological approach for enhancing the cognitive and emotional health of institutionalized elderly populations. Future research should explore long-term effects and investigate the broader application of MBG in diverse elderly populations and care settings.
Authors’ Contributions
Principal investigators: A.J.H. and R.M.S. Research design: A.J.H., A.L., C.A., and E.J.C. Development of board game sessions: A.L., C.A., E.B.B., and E.J.C. Data collection: E.C.A., J.M.S.R., M.H.M., and R.M.S. Data analysis: A.J.H. and E.C.A. Writing article: A.J.H. and R.M.S. Reading article and provide feedback: All authors.
Footnotes
Acknowledgments
The authors express their gratitude to Juan Antonio Alonso, social educator at the Doctor Villacián Center, for their collaboration in recruiting residents and assisting with several study assessments. The authors also extend their thanks to Juan José Zancada Polo, director of the center, and to the center’s staff, whose support was invaluable in facilitating the study’s smooth execution. The authors are especially grateful to the residents who participated, allowing them to share in this enriching experience. Additionally, the authors thank Celia Arranz Regidor (Akari) for her assistance during some of the gaming sessions.
Author Disclosure Statement
No competing financial interests exist for any of the authors of the study.
Funding Information
This research was supported by the Diputación de Valladolid (project code: 2023-JUMEMO3e).