
Abstract
Introduction:
Veterans use cannabis as a chronic pain treatment due to a combination of the easing of restrictions and dissatisfaction with care standards. The segregation of medical cannabis from conventional health systems may translate to opportunities and disadvantages that are not well defined. Our study aimed to characterize how Veterans with chronic pain approach using cannabis for symptom management, including product access, developing a treatment plan, and its integration into daily life.
Materials and Methods:
We used an interpretive description design and conducted semi-structured interviews with U.S. Veterans in Michigan who had chronic pain; were aged 21 years or older; and (a) used cannabis, (b) were planning to use cannabis, or (c) interested in learning about how cannabis could help with pain. We analyzed deidentified interview transcripts to develop themes that focused on how Veterans approached new and continued use of cannabis for chronic pain management.
Results:
Participants were Veterans with chronic pain, median age = 50 years (n = 32). Participants described how factors at the individual, relationship, community, and societal levels influenced their interest in and use of cannabis for chronic pain. We identified five main themes: (1) cannabis supports holistic wellness, but there are also undesired effects; (2) medical cannabis requires a personalized treatment approach; (3) Veterans seek expanded access to medical cannabis and more assurance regarding product safety and efficacy; (4) sociopolitical attitudes and advocacy shape medical cannabis acceptability; and (5) the interest in research to inform treatment approaches and facilitate access.
Discussion:
This article illustrates how Veterans approached using cannabis for chronic pain management. Findings illuminate the potential value of cannabis for Veterans with chronic pain while also highlighting numerous obstacles and limitations related to its use. There are opportunities for health care providers to support Veterans who are interested in cannabis while research regarding efficacy and safety continues. Future efforts should engage Veterans to collectively work toward a better understanding of cannabis as a pain treatment option.
Introduction
Chronic pain is disproportionately more prevalent among Veterans in the United States and associated with poorer quality of life and suicide-related outcomes.1–3 Chronic pain treatment has low remission rates and can result in unnecessary surgeries.4,5 The legacy of opioid-based treatment protocols for chronic pain contributes to higher rates of opioid use and misuse among Veterans, 6 which can exacerbate pain symptoms. 7 These realities have contributed to Veterans’ dissatisfaction with chronic pain care 8 and interest in novel pain treatment options, including cannabis. 9 Coinciding with an increase in state-level legalization of cannabis across the United States, 10 Veterans report using cannabis to manage their pain symptoms and as an alternative to opioids.11,12 However, medical cannabis is often segregated from conventional health systems and pain care settings, which may translate to a variety of opportunities and disadvantages that are not well defined. Addressing this knowledge gap could inform advances in chronic pain research, education, and care.
Thus far, there is limited qualitative literature about U.S. Veterans’ views and experiences regarding cannabis within chronic pain management. Prior work focuses on the perceived risks and benefits of cannabis among younger U.S. Veterans and active military (aged 18–29 years) where participants considered cannabis acceptable for managing pain and preferred cannabis over opioids, alcohol, and benzodiazepines. 13 In another study, U.S. Veterans (aged 60 years or older) described stigma associated with their cannabis use and hiding their use due to stigma. 14 There is also a collection of research about cannabis use for pain symptoms that is not specific to Veterans.15,16 In these studies, participants talked about experimenting with cannabis products (e.g., cannabinoid ratios, potency); varied success when replacing or supplementing opioids with cannabis; and how cost, uncertain legal status, stigma, adverse effects, safety, and a lack of experience among physicians posed challenges to appropriately using cannabis for pain management.16–23
There are several opportunities to extend existing evidence regarding cannabis for chronic pain in Veterans who have a distinct culture and unique health care needs. 24 For example, providers in the Veterans Health Administration (VA) cannot prescribe medical cannabis due to federal regulations, regardless of state-level legislation. 25 Additionally, rates of post-traumatic stress disorder (PTSD) and long-term opioid use are relatively high among U.S. Veterans.26–28 Both PTSD and opioid use have notable relationships with chronic pain, where PTSD can worsen pain symptoms, 29 and long-term opioid therapy is not considered an effective treatment for chronic pain with severe adverse effects. 30 Thus, the overall appropriateness, acceptability, and benefits of medical cannabis as part of an integrative health approach may be distinct among Veterans. In this qualitative study, we aimed to illustrate how U.S. Veterans approach new and continued use of cannabis for chronic pain management, including product access, developing a treatment plan, and its integration into daily life.
Materials and Methods
Study design
This study was part of a larger program of work aimed at advancing the quality of chronic pain care and research among Veterans by centering the lived experiences of Veterans and using community-engaged research approaches that prioritize equity and inclusion. The qualitative interviews in this study provided a foundation for establishing the University of Michigan Community Advisory Board for Veteran Care and Research (Veteran CAB) and informed the design of clinical trials on cannabis-based therapies for chronic pain (Bergmans et al. 31 ). Given our interest in developing better approaches to research, education, and health care for Veterans, we used an interpretive description design, which stipulates the application of pertinent preexisting evidence during analysis to generate practical recommendations.32,33 The University of Michigan Institutional Review Board designated this study exempt from ongoing review. We adhered to the Standards for Reporting Qualitative Research guidelines (Supplementary Data S1). 34
Reflexivity
A critical research paradigm and five preconceptions informed our work, including our interview guide development and data interpretation. We used a critical research paradigm due to its alignment with social justice and health equity, its consideration of systemic oppression (including within health care systems and public policy), and its focus on what should be done to reform circumstances. Our preconceptions were (1) chronic pain increases the risk of substance use disorders and suicide-related outcomes; (2) long-term opioid therapy for chronic pain is ineffective and increases the risk of adverse effects such as overdose; (3) there is a lack of treatment protocols regarding cannabis for chronic pain; (4) cannabis use is stigmatized in U.S. society; and (5) there are factors across individual, intrapersonal, and societal domains that may influence how Veterans approach using cannabis for managing chronic pain (consistent with Bronfenbrenner’s ecological systems theory 35 ). Members of the study team have had contact with the study population through clinical and community-engaged research activities.
Study sample and recruitment
Participants had to be U.S. Veterans in Michigan who had chronic pain; were aged 21 years or older (the legal age for recreational cannabis purchasing); and (a) used cannabis, (b) were planning to use cannabis, or (c) were interested in learning about how cannabis could help with pain. We allowed for a range of experiences and perspectives concerning cannabis use to facilitate data richness across multiple relevant viewpoints. We determined eligibility with a screening questionnaire (Supplementary Data S2) and required individuals to provide documentation that confirmed their identity and Veteran status. We opened recruitment on December 5, 2022, via an online research recruitment platform, social media advertising, and snowball sampling to obtain a convenience sample. Given that this study functioned as a foundation for a program of work related to Veterans’ lived experiences, chronic pain, and cannabis use (representing circumstances that can be sensitive and stigmatized), we were uncertain of Veteran interest and engagement in this study. Evidence suggests that convenience sampling is beneficial for recruiting within hard-to-reach communities. 36 Individuals received $25 for participation.
Data generation
After reviewing relevant literature, authors with expertise in cannabis and cannabinoid research, health equity, chronic pain, and Veteran health developed a semi-structured interview guide tailored to cannabis use status (Supplementary Data S3). We aimed to recruit at least 30 participants to ensure data saturation, informed by previous work. We collected data using videoconferencing software that was compliant with the Health Insurance Portability and Accountability Act (HIPAA). Prior to completing a semi-structured interview, participants provided verbal consent. During data generation, we monitored saturation by creating summary statements and assessing data repetition (defined as two participants or more) across priori categories, including (a) cannabis benefits and adverse effects, (b) knowledge concerning cannabis as medicine, and (c) talking about cannabis with others. We completed 32 interviews based on who expressed interest in the study prior to confirming data saturation and ending recruitment. Interview duration ranged from 17 to 87 min (median = 40 min). An external HIPAA-compliant service transcribed the interview recordings verbatim, and we deidentified the data prior to analysis.
Analysis
We used an inductive thematic analysis approach that was data driven to better prioritize participant perspectives and facilitated a dynamic coding process where interpretation could evolve based on new insights. 37 First, seven authors open coded the transcripts to identify salient concepts under the supervision of a senior author and with the support of a coding template (Supplementary Data S4). After each transcript was independently coded by two authors, they independently transferred the quotes that represented salient concepts to copies of the coding template, which one author compared for consistency. This included coding and transferring unexpected data segments as a separate (i.e., “other”) code. At weekly team meetings, we reviewed data segments for relevance to our research question, coding discrepancies, and unexpected findings. Group discussion allowed us to reach consensus and supported coding fidelity. We then created detailed profiles for each participant, which included text memos and pictorial diagrams to describe salient concepts and relationships between concepts (e.g., Supplementary Data S5). We used these within-person profiles to generate categories that represented the data across participants. Category development focused on how Veterans with chronic pain approached using cannabis for symptom management.
To increase the trustworthiness and rigor of our research, we sought input from representatives of the study population.38,39 On December 7 and 20, 2023, we presented our categories to the University of Michigan Veteran CAB. The Veteran CAB is a diverse group of people who are Veterans, represent Veteran groups, or provide health care to Veterans. Veteran CAB members did not propose specific changes but provided additional context and examples related to our categories.
Once we received Veteran CAB feedback, we converted our categories to preliminary themes and created a corresponding coding scheme to refine our themes. Specifically, we used MAXQDA 2024 (VERBI Software) to apply the coding scheme to each transcript. In this iterative process, we adapted the themes to reflect any findings that conflicted with the original coding scheme. This approach resulted in the final five themes, which achieved inductive thematic saturation and conceptual depth (i.e., at least two participants exemplified each example of qualitative experience within the themes) after the first 17 interviews. We verified our final themes with the Veteran CAB on March 14, 2024.
Results
Participants were Veterans with chronic pain, median age = 50 years (n = 32, Table 1). Regarding gender, 6 participants were women and 26 were men. Regarding race, 1 participant was Asian, 2 were multiracial, 3 were Black, and 26 were White. Additionally, 2 participants were Hispanic. Among participants, 23 reported currently using cannabis for chronic pain (i.e., participants with current use, PCUs), and 9 reported that they were either planning to initiate use or interested in learning more about how cannabis could help with pain (i.e., participants with no cannabis use, PNUs). On average, participants concluded active military duty 23 years ago. Most (78%) currently received at least some of their care through the VA, 53% were married, and 59% had a 4-year college degree or above. Financial hardship was reported by 25% of participants (i.e., food insecurity, housing insecurity, lack of access to transportation, and/or skipping medications or doctors’ visits due to the cost).
Participant Characteristics
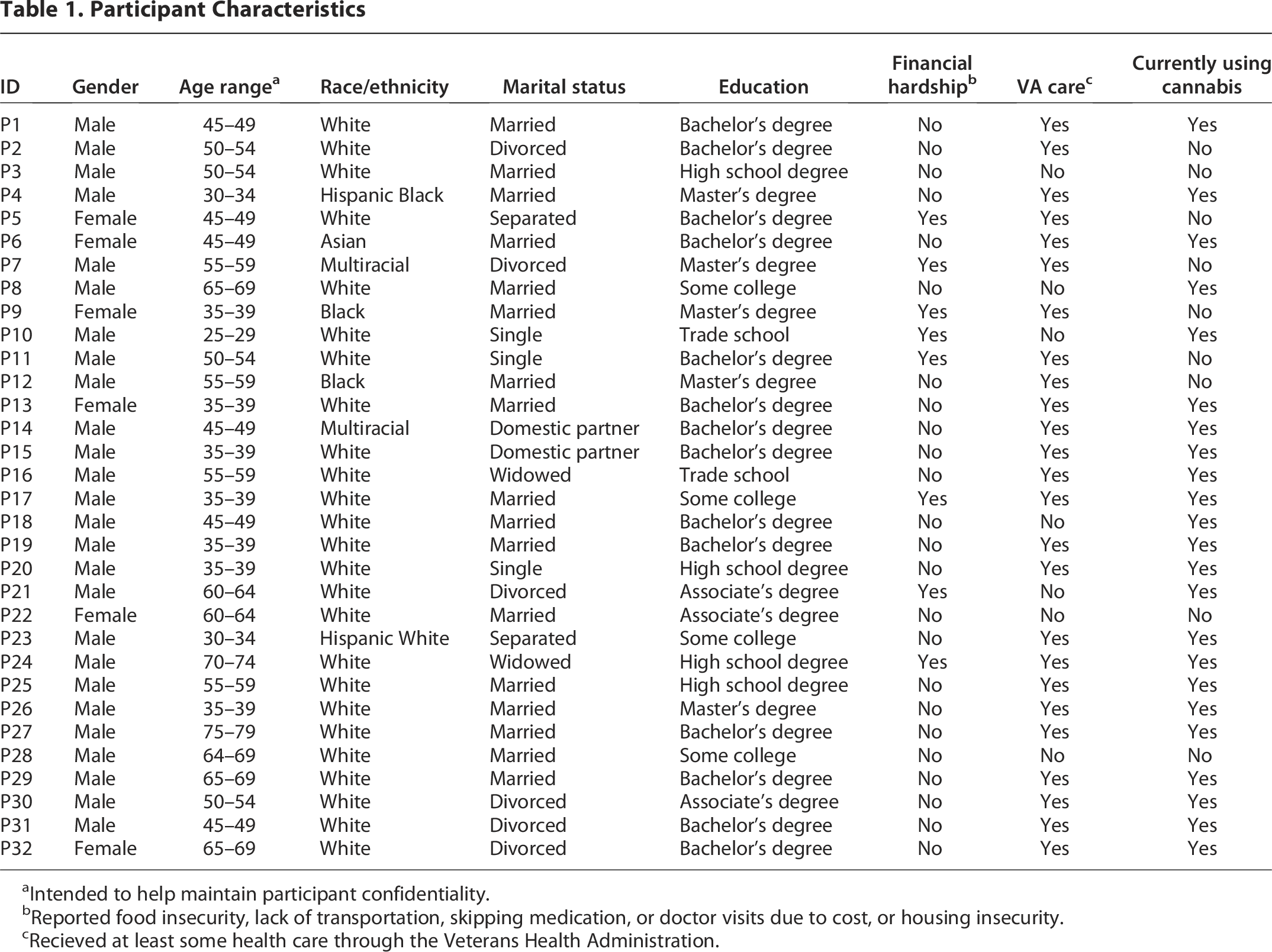
Intended to help maintain participant confidentiality.
Reported food insecurity, lack of transportation, skipping medication, or doctor visits due to cost, or housing insecurity.
Recieved at least some health care through the Veterans Health Administration.
Five main themes reflect how Veterans with chronic pain approached using cannabis for symptom management (Table 2). These themes illustrate how Veterans considered cannabis’s potential health benefits, developed a treatment approach, obtained products, integrated cannabis use into their daily life, and desired more evidence to inform their treatment approach and cannabis access. To provide further description, these themes represent factors across multiple domains, consistent with Bronfenbrenner’s ecological systems theory, that influenced this process. Presented in Figure 1, individual factors that determined a participant’s approach to cannabis use included prior experience with cannabis (both positive and negative), symptom severity, safety and stigma concerns, and cannabis access. Social networks were influential as a resource for emotional support and cannabis education and products. Health care factors included whether a participant’s provider was considered supportive and knowledgeable of medical cannabis use, the undesired effects of alternative pain treatments, and the lack of cannabis-based prescriptions for pain. At the policy level, cannabis restrictions affected where participants lived and their employment. Additionally, the lack of regulation increased concerns about cannabis product quality and safety for some participants.
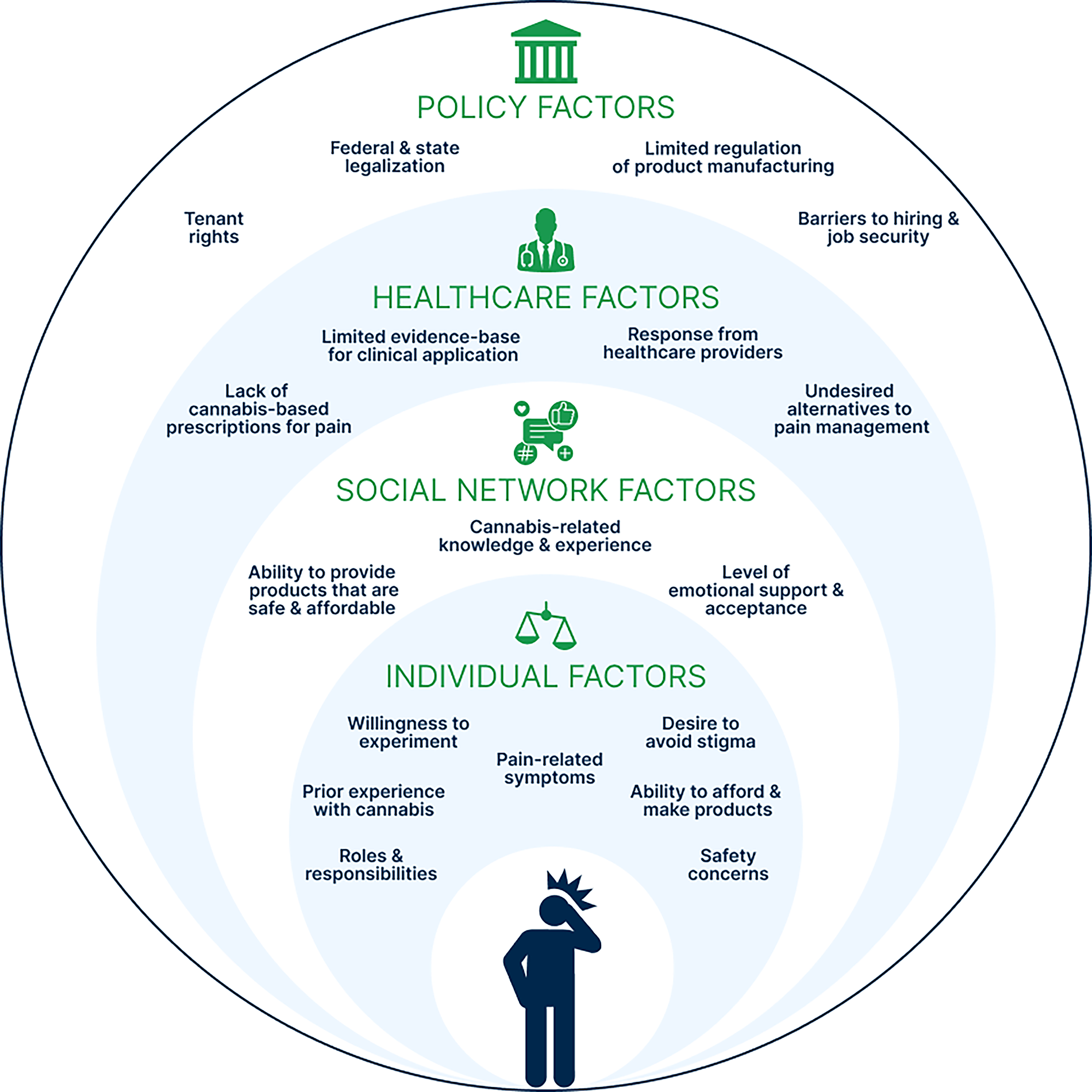
Factors across multiple domains influenced how Veterans with chronic pain approached symptom management, based on participants’ qualitative experiences.
Five Main Themes That Describe How Veterans with Chronic Pain Approach Using Cannabis for Symptom Management
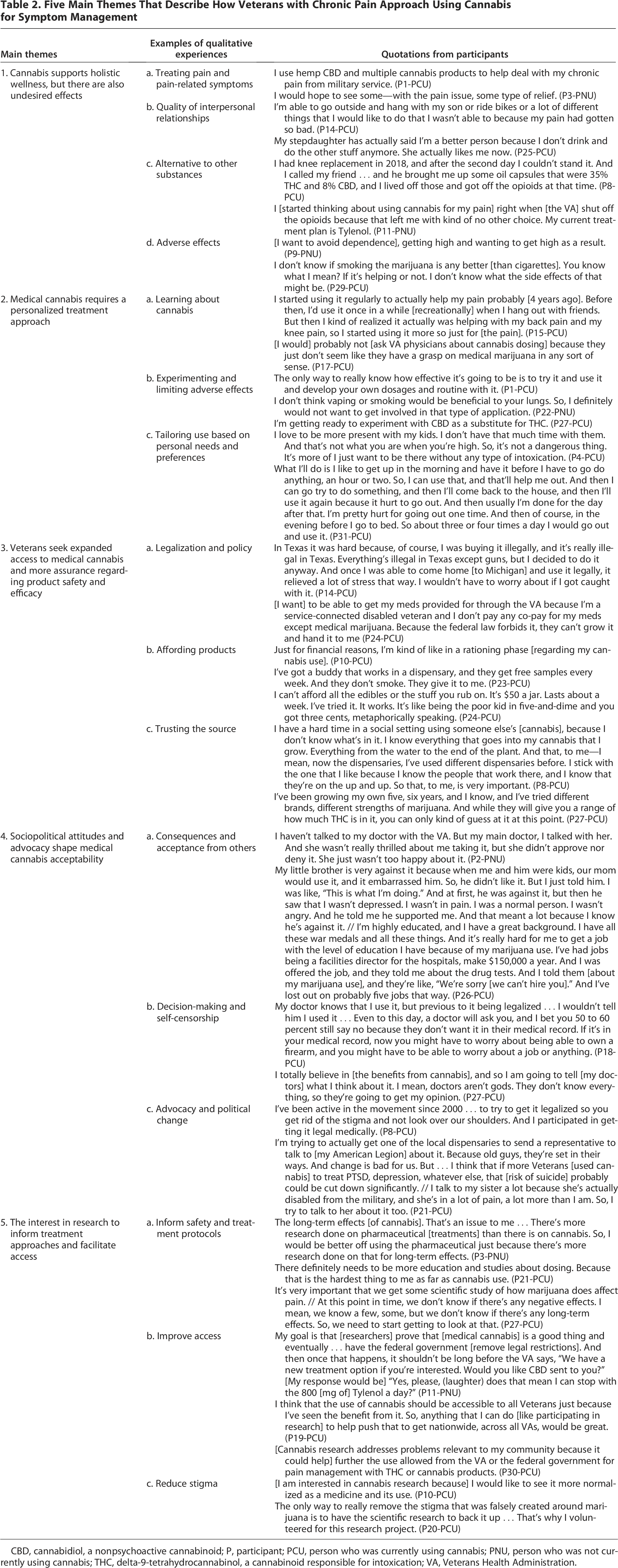
CBD, cannabidiol, a nonpsychoactive cannabinoid; P, participant; PCU, person who was currently using cannabis; PNU, person who was not currently using cannabis; THC, delta-9-tetrahydrocannabinol, a cannabinoid responsible for intoxication; VA, Veterans Health Administration.
Theme 1. Cannabis supports holistic wellness, but there are also undesired effects
Participants described the experience and potential advantages of using cannabis to support chronic pain management across multiple domains of wellness, including physical, mental, emotional, and social benefits. Concurrently, participants weighed these benefits against cannabis’s undesired effects that had the potential to decrease quality of life.
PCUs said cannabis had both physical and mental health benefits related to their pain. Cannabis alleviated pain by easing pain, numbing pain, eliminating pain, making pain bearable, distracting from pain, and reducing swelling. PNUs talked about their hopes for pain relief from cannabis, such as the ability to complete household chores and avoid surgery. One participant detailed how cannabis was necessary for treating the combination of her physical and psychological pain:
When [my memory] started coming back … and then when my son died, my pain level went sky high because that psychological pain wrapped up the physical on top of all that I was dealing with … I was at the point where I had to [use marijuana]//I wouldn’t be here if I had a gun and I didn’t have marijuana. (Participant [P]32-PCU)
PCUs explained how symptom improvement allowed them to engage in other behaviors that benefited their health and well-being. This included higher levels of physical activity, better sleep quality, participating in recreational activities (e.g., going ice fishing, painting), and eating a healthier diet. PCUs also highlighted how the effects of cannabis improved the quality of interpersonal relationships, including as a parent, grandparent, or spouse. As one participant said:
[Because of my pain] I missed out on a lot of stuff with my kids. There’s so much I would have loved to have done with my children when they were younger … that probably hurt the most. // [After using cannabis for pain] I went out to visit [my kids and grandkids] … and they had never ever had the opportunity to play frisbee with their dad. I just had the greatest time playing frisbee with my kids and that was magic. (P14-PCU)
PCUs said cannabis helped decrease and cease use of opioids, alcohol, and nonsteroidal anti-inflammatory drugs because it was more effective and had fewer adverse effects. One PCU preferred that he and other Veterans use cannabis over opioids for pain to decrease the risk of an overdose, and because opioids could be a means of suicide (P25-PCU). Another PCU said that commercially available cannabis was more accessible than opioids since VA physicians were reluctant to prescribe opioids (P14-PCU). PNUs hoped that cannabis would decrease their use of opioids and other medications, which they considered to have a worse risk profile and be insufficient for managing pain.
Participants identified undesired effects from cannabis, including intoxication, drowsiness, smelling like cannabis, vomiting, dependency, paranoia, and harms to respiratory health from smoked products. Increased appetite was a concern for some, but it was helpful for those who had early satiety. Cognitive impairment was noted by three PCUs. However, PCUs considered it a benefit when cannabis helped with forgetting traumatic events from active duty and preventing unwanted dreams due to PTSD.
Theme 2. Medical cannabis requires a personalized treatment approach
Participants navigated limited empirical evidence and clinical guidance, which existed alongside alternative sources of information, to inform their cannabis treatment approach. Participants educated themselves as a first step to cannabis use, and PCUs pursued continuing education. Some participants were initially exposed to cannabis through recreational use in their youth. Nearly half of participants said they learned about cannabis for pain from people they knew, such as family members, friends, coworkers, and other Veterans. For example,
[I started thinking about using cannabis for my chronic pain] within the last year. Seeing a family member make use of it for arthritis pain gave me the idea. (P9-PNU)
Participants talked about the limitations of getting information from cannabis dispensaries: two PNUs were skeptical of retailers given their intrinsic financial motivation, and one PCU felt that dispensaries focused more on recreational use over medicinal use. Participants also learned about cannabis online from research papers and testimonials. This was helpful for some, but others found it difficult to identify reputable sources. A few participants sought guidance about cannabis from physicians, which included “there’s no data on it, don’t use it” (P4-PCU), “edibles are the preferred method” (P6-PCU), and “if it was legal, we’d prescribe it” (P23-PCU). One PCU said he would not consider talking to physicians about cannabis due to their lack of knowledge (P17-PCU).
Past use and undesired effects influenced participants’ treatment approach with cannabis, which often featured experimentation to determine dosing and administration routes. One PNU talked about starting slowly with lower doses of delta-9-tetrahydrocannabinol (THC, a cannabinoid responsible for intoxication) due to negative experiences associated with prior recreational use. Some PNUs only wanted to consider products that were not smoked or were not psychoactive due to the potential for undesired effects. Some PCUs talked about reducing THC use or replacing THC with cannabidiol (CBD, a nonpsychoactive cannabinoid) and limiting the use of smoked products for similar reasons. Although experimentation was expected, the potential for undesired effects was a concern for some. A PNU described the process as “somewhat risky” (P9-PNU), and an experienced PCU said he still had “dosage anxiety” (P21-PCU).
In addition to selecting cannabis products based on efficacy and adverse effects, there were additional needs and preferences that influenced cannabis use behaviors. For some, this meant abstaining around children because they felt it was not age appropriate. A PNU wanted to avoid products such as gummies that would appeal to young children in her home (P9-PNU). PCUs preferred cannabis before bed to improve sleep and to prevent drowsiness or intoxication from interfering with daily responsibilities. Multiple participants described how symptom flares determined the frequency and timing of cannabis use throughout a day. Some participants timed their use so that cannabis’s effects could help them accomplish tasks, for example, to get “in that grind mode” (P10-PCU) or to be “more introspective” for a philosophy course (P13-PCU).
Theme 3. Veterans seek expanded access to medical cannabis and more assurance regarding product safety and efficacy
Participants talked about how sourcing cannabis was impacted by legalization, cost, and safety concerns. The legalization of recreational cannabis, no longer having to adhere to military policies, and the opening of local dispensaries increased PCUs cannabis use and PNUs interest in cannabis. For example:
“Once it became recreational and I could buy it, then I started buying it regularly to help with my pain.” (P19-PCU)
At the same time, participants said the inability of physicians to prescribe cannabis products for pain was a barrier to treatment. Participants also talked about how the cost of cannabis led to rationing products or seeking free samples. A PNU was worried that cannabis was going to help with his pain symptoms (P11-PNU), which would then require finding a way to finance treatment. One PCU wished that the VA “would give you a card that you could use at dispensaries that has so much on it a month … where it covers a portion of what you buy” (P17-PCU). Another participant explained how she approached her limited access to cannabis:
[I use cannabis sparingly] because you don’t know when you’re going to be able to find it again to buy and from a reputable, safe person that you can buy it from. And believe me, when you get down to a little bit, you just save it. You just save it until it’s an emergency because you can’t waste it on funny games. (P32-PCU)
Similarly, some participants emphasized the importance of trusting their cannabis source to ensure safety and consistent dosing, whether this meant only frequenting a single dispensary or making their own products.
Theme 4. Sociopolitical attitudes and advocacy shape medical cannabis acceptability
Public perceptions and legal restrictions of cannabis could have a profound impact on participants’ choices and actions regarding medical cannabis. Participants faced varying degrees of personal consequences and social acceptance from cannabis use. Reception from health care providers ranged from threatening to “call the authorities” if a PCU came to a visit smelling like cannabis (P14-PCU), to helping a PCU prevent adverse interactions with prescribed medications (P27-PCU). One participant elaborated:
I got a real judgmental kind of look from [my old doctor], and then the whole mood, the whole vibe that I got from him just shifted. And I never liked going back to him, just because every time I did, I just felt like I was doing something wrong. (P15-PCU)
This spectrum also existed within participants’ personal lives. Some described cannabis as a way to bond with others, and family members encouraged and reminded participants to use cannabis. Conversely, one participant said his cannabis use was held against him in a child custody case following divorce (P31-PCU), and another said he was not hired for five jobs due to his cannabis use despite receiving medals for his active military duty and having a graduate degree (P26-PCU).
Cannabis restrictions and stigma influenced participant decision-making and self-censorship. Although some did not care who knew about their use, others were more cautious and wanted to know someone’s views before disclosing information. One PCU relocated across the country for graduate school because his chronic pain was getting worse, and cannabis was not legal where he lived previously (P4-PCU). Local acceptance also made the participant more comfortable to talk about his cannabis use:
I talk to a lot of people about [my cannabis use]. Mostly because in this place at this point in my life, and this program, no one cares, right. [The city where I live has] a very pot-friendly culture. If I were still in [Alabama], I probably wouldn’t talk to as many people about it, or the conversation would be different. (P4-PCU)
Some participants considered cannabis legalization a prerequisite to changing public opinion. PCUs advocated for cannabis within their social networks and politically to raise awareness about its medicinal value and address misconceptions.
Theme 5. The interest in research to inform treatment approaches and facilitate access
Participants desired more research to inform their symptom management. For example:
I just want to see if it’s really medicinal or not because a lot of people are saying it is, and a lot of them are saying it’s not. So, I’d like to know for sure. I asked [my pharmacist] about it, and he didn’t really know. He said there weren’t enough studies and statistics out yet. That kind of steered me away from trying it back then. I didn’t want it to interfere with my other meds. (P28-PNU)
Additionally, participants wanted research to address challenges associated with using cannabis for chronic pain, including more evidence-based options for personalizing their cannabis use, selecting cannabinoid ratios and strains, and harm reduction. For example:
I make my own edibles and stuff. Research on how that is different than smoking, how smoking is different than vaping, how vaping chemicals is different than vaping flower. All these were a stock of significant money that I had to put down [to] investigate for personal use. If there was something that would have [clarified], “Here’s the effect of each one of these, and here’s the best way to consume each method,” I could have just saved myself a lot of money. (P4-PCU)
Participants also considered further research necessary for increasing affordable access, such as cannabis prescriptions for pain and reducing stigma.
Discussion
In this qualitative study, we interviewed U.S. Veterans to illustrate how they approached cannabis use for chronic pain. We identified five themes: (1) cannabis supports holistic wellness, but there are also undesired effects; (2) medical cannabis requires a personalized treatment approach; (3) Veterans seek expanded access to medical cannabis and more assurance regarding product safety and efficacy; (4) sociopolitical attitudes and advocacy shape medical cannabis acceptability; and (5) the interest in research to inform treatment approaches and facilitate access. Prior work describes the experiences of people who use cannabis for pain,15–23 with a minimal focus on Veterans in the United States and other countries such as Canada where medical and recreational cannabis are legal.13,14,40 Our results are consistent with previous findings that cannabis can provide comprehensive health and social benefits to those with chronic pain, treatment approaches are often tailored over time, and people face barriers to access despite legalization. Our results also extend existing evidence by detailing the unique benefits and challenges of using cannabis for symptom management among U.S. Veterans with chronic pain and by applying Bronfenbrenner’s ecological systems theory to characterize how factors across multiple domains can influence this process.
In this study, participants used cannabis to provide a combination of pain relief and mental health benefits, such as ameliorating symptoms associated with suicide-related outcomes and PTSD and improving interpersonal relationships. This is relevant because Veterans have an elevated risk of suicide, 41 PTSD symptoms, 42 alcohol use disorder, 43 and other mental health concerns, including higher rates of social isolation.44,45 However, the evidence surrounding cannabis as a treatment or risk factor for mental health conditions is inconclusive.46,47 The potential therapeutic effects of cannabis on mental health may depend on whether someone has comorbid chronic pain, the types of cannabinoids used, or other contextual factors, which requires further study.
Our results demonstrated the value of social support when using cannabis for chronic pain. Friends, family members, and others offered education, cannabis products, and treatment support in the absence of clinical guidance or resources. Physicians are often limited in their ability to offer cannabis as a pain treatment option given the current scientific and regulatory landscape. Although there are cannabis-based prescriptions approved by the U.S. Food and Drug Administration (e.g., dronabinol capsules for loss of appetite, CBD solution for seizures), none are approved for chronic pain. Additionally, there is a lack of relevant training and stigmatized perceptions of cannabis use in health systems,48–51 which decreased the willingness of participants in our study to talk about cannabis with health care providers. As research regarding cannabis for chronic pain continues, there is an opportunity for health care providers to improve patient-provider communication and promote harm reduction. Examples include collecting cannabis use history; sharing information about federal legal status and state regulations; and risk–benefit discussions that review existing evidence, potential drug interactions, and product safety. 52
Limitations
These results, which reflect the lived experience of U.S. Veterans residing in Michigan, may not be representative of all Veterans or specific Veteran subgroups. Michigan legalized medical cannabis in 2008 and recreational cannabis in 2018, following 10 U.S. states that previously legalized cannabis for recreational use. Along with Canada and some regions in the European Union, Michigan has more progressive cannabis policies than many other areas worldwide.
Conclusions
Our findings illuminate the potential value of cannabis for Veterans with chronic pain, while also highlighting numerous obstacles and limitations related to its use. There are opportunities for health care providers to support Veterans who are interested in cannabis as a chronic pain treatment while research regarding efficacy and safety continues. Future efforts should engage Veterans and include Veteran perspectives to collectively work toward a better understanding of cannabis as a pain treatment option.
Authors’ Contributions
R.S.B., A.S.B.B., and K.F.B. conceived of this study and obtained funding. R.S.B., V.K., A.S.B.B., and K.F.B. designed the study approach and materials. J.S., V.K., and S.D. collected the data. R.S.B., C.Y., L.Z.X., R.W., J.S., S.R., and S.D. analyzed the data. R.S.B. wrote the first draft of the article. All authors contributed to data interpretation and article revisions, and all authors approved of the final version to be published.
Footnotes
Acknowledgments
This work would not have been possible without the contributions of study participants and members of the Veteran CAB, including John Booher, B. Danielle Engle, Stuart K. Jacobson, Ronald Kidd, Kali Lake, Biyyiah A. Lee, Regina Murray, Carmencita Pinckney, and Jason Lee Straw.
Author Disclosure Statement
R.S.B. reported receiving personal fees from Tonix Pharmaceuticals Inc for consulting outside the submitted work. K.F.B. sits on a data safety and monitoring board for an ongoing clinical trial with Vireo Health (unpaid) and received an honorarium from Viatris Inc. for a podcast on fibromyalgia not related to the current work. All other authors have no interests to disclose.
Funding Information
This work was performed using funds granted by