
Abstract
Background:
Men with chronic scrotal content pain (CSCP) commonly present to various providers within the healthcare system. Despite its prevalence, little research has been done to understand risk factors for the development of CSCP. In many cases, the cause of pain is unknown, and there are no widely accepted protocols for evaluation or management.
Objective:
To characterize associated symptoms and concomitant concerns of those presenting with CSCP.
Design and methods:
Retrospective review of validated questionnaires including the Chronic Orchialgia Symptom Index (COSI), the internal index of erectile function, the NIH-chronic prostatitis symptom index, the American Urological Association symptom index/international prostate symptom score, the hip dysfunction and osteoarthritis outcome score, the Oswestry low back pain questionnaire, the patient health questionnaire-9, the general anxiety disorder-7, and a comprehensive intake form on men presenting to a single urologist’s office with CSCP was performed. The analysis included constructing linear best-fit lines between subjective chronic testicular pain rating and other numerical rating scales.
Results:
Questionnaires from 94 male patients were reviewed. The average pain subscore on the COSI was 8.00 out of 17. When assessing the association between pain and other domains, more severe chronic scrotal pain was associated with worse pain in and around the genitourinary system (p < 0.001), worse urinary symptoms (p = 0.001), worse hip (p = 0.001) and back (p < 0.001) symptoms, worse sexual function (p = 0.025), and worse anxiety (p = 0.019) and depression (p = 0.003) symptoms. Patients in our study were found to have a wide variety of presentations with differing aggravating and relieving factors, urological and surgical histories, and interventions.
Conclusion:
Men presenting with CSCP may present with many co-occurring symptoms. More severe scrotal content pain may be associated with worse symptoms in multiple other domains. In order to create a personalized treatment plan, a more comprehensive understanding of these men is critical. Future studies should focus on further developing a standardized approach for assessing these patients and how directed interventions on associated symptoms may impact outcomes.
Introduction
Chronic scrotal content pain (CSCP) refers to unilateral or bilateral pain localized to the scrotum lasting at least 3 months that significantly interferes with daily activities. 1 CSCP is estimated to account for 2.5%–5% of urology consultations and affects about 100,000 men in the United States per year. 2 While causes of acute scrotal pain have been thoroughly reviewed in the literature, there is minimal research regarding CSCP. 3 Etiologies include spermatocele, varicocele, infection, trauma, tumors, and post-vasectomy pain syndrome, but up to 50% of cases remain idiopathic. 4 Further complicating the understanding of CSCP etiology is that, while these structural abnormalities are common findings, it is unclear if/when they are the cause of the CSCP. As such, there is no recognized and accepted standard protocol for evaluation or treatment of this often debilitating condition. 5
Chronic scrotal content pain presents in a variety of ways. The pain may be unilateral or bilateral, constant or intermittent, and spontaneous or exacerbated by certain activities. 6 The pain may remain localized to the scrotum or may radiate to surrounding areas, including the groin, hip, and/or lower abdomen. The heterogeneity of CSCP makes the assessment and treatment of this condition particularly challenging.
Chronic scrotal content pain may have a significant impact on patients’ quality of life. The pain may interfere with the ability to work and socialize and may also limit sexual activity. Furthermore, chronic pain conditions are commonly associated with major depression and anxiety disorders, and as such, depression and anxiety may also be associated with CSCP. 7 Limited research has been done to assess the effects of CSCP on quality of life, but one study found men reported less frequent sexual thoughts and decreased sexual desire, as well as less frequent sexual activity, diminished arousal, and lower orgasmic function. 6
The differential diagnosis for CSCP is broad. Increasing research supports the role of pelvic floor dysfunction (PFD) as a contributing cause of CSCP. Underactivity and/or overactivity of these pelvic floor muscles can lead to bothersome symptoms related to micturition, defecation, sexual function, and/or pelvic pain. 8 In one study of 41 male patients presenting with chronic testicular pain, 93% had at least 1 symptom suspicious of PFD. However, the prevalence of PFD within the patient population presenting with CSCP remains unknown, and there is a lack of screening tools to aid in the diagnostic process.
Another condition that can lead to chronic pain in the genital region includes urologic chronic pelvic pain syndrome (UCPPS). UCPPS, which encompasses both interstitial cystitis and chronic pelvic pain syndrome, is characterized by chronic pain in the pelvic region or genitalia that is often accompanied by urinary frequency and urgency. 9 Similar to CSCP, despite considerable research, there have been no definite etiological risk factors or curative treatments identified. Thus, differentiating between CSCP and UCPPS is difficult, and there is likely considerable overlap between these two chronic pain conditions.
To help further understand the patient population presenting with CSCP, we retrospectively reviewed questionnaires given to patients presenting to a single urologist’s men’s health clinic with CSCP to better understand the associated urinary, sexual, musculoskeletal, and mental health concerns of this patient population.
Materials and methods
Men 18 years of age or older presenting to a single urologist’s office at a tertiary care academic center with 3 or more months of unilateral or bilateral CSCP were asked to complete paper questionnaires during their clinic visit as part of standard clinical practice. Afterward, they underwent a comprehensive physical examination performed by the urologist. Depending on their presenting symptoms, they were offered a number of different treatments, such as pelvic floor physical therapy or referral to orthopedics for musculoskeletal evaluation. Patients who were minors or reported their scrotal content pain was less than 3 months in duration were excluded.
Patients completed an intake form developed by the urologist assessing detailed characteristics of their presenting pain, potential contributing factors/causes, and prior treatment(s). Patients also completed the Chronic Orchialgia Symptom Index (COSI), a validated survey assessing the severity of chronic testicular pain symptoms and response to therapy, comprising 12 questions in 3 domains (pain, sexual symptoms, and quality of life) with higher scores indicating more severe symptoms. 10 The five-item version of the International Index of Erectile Function (IIEF-5) was used to assess sexual function, with higher scores indicating less severe symptoms.11,12 The NIH-chronic prostatitis symptom index (NIH-CPSI), a nine-item validated tool for men with chronic prostatitis and chronic pelvic pain, was used to assess pain or discomfort in areas in and around the genitourinary system, urinary symptoms, and the impact of symptoms, with higher scores indicating more severe symptoms. 13 The American Urological Association Symptom Index (AUA-SI)/International Prostate Symptom Score (IPSS) was used to assess the severity of urinary symptoms, with higher scores corresponding to worse symptoms. 14 To evaluate for the presence and impact of pain involving the back and hip, the Oswestry low back pain disability questionnaire and hip dysfunction and osteoarthritis outcome score for joint replacement (HOOS, JR) were administered, respectively. The Oswestry questionnaire is a 10-question survey assessing the impact of back or leg pain on the ability to manage everyday life, with a higher score indicating a greater degree of disability. 15 The HOOS, JR. Hip Survey is a six-question tool used to assess the impact of hip pain on daily activities, with a higher score indicating worse hip health. 16 To assess mental health, the general anxiety disorder-7 (GAD-7) and Patient health questionnaire-9 (PHQ-9) were administered. The GAD-7 is a seven-item anxiety scale used to screen for generalized anxiety disorder, with a higher score indicating more severe anxiety. 17 The PHQ-9 is a nine-item tool to assess the severity of depression, with higher scores indicating more severe depression. 18 Lastly, the physical activity vital sign questionnaire was used to assess exercising habits, including the average amount of time patients engaged in moderate to vigorous exercise per day, as well as the number of days per week.
Some patients filled in multiple answers on a single-choice question. When these double answers occurred, the answer was not reported. In a few cases, patients filled out duplicates of a single survey. With these patients, the questionnaire with more severe answers was included. Questionnaires were then retrospectively reviewed, and data were recorded in Qualtrics.
For statistics, quantitative variables were reported as mean and standard deviation, while categorical variables were reported as percentages. Alpha values were pre-designated at 0.05. In addition, subjective chronic testicular pain rating was compared to each numeric pain scale rating in scatter plot format using the R package ggplot2. 19 To this, we overlaid a line of best fit to illustrate whether there was an association between the two variables. In addition, linear best-fit line calculations were also completed, including β and p values to assess if relationships between variables were significantly nonzero. Analysis was conducted in R version 4.0.2. 20
Results
Questionnaires from 94 patients were retrospectively reviewed from July 1, 2020, to August 1, 2022. Patient demographics are summarized in Table 1.
Demographics and baseline characteristics of study participants (n = 94).

Chronic orchialgia symptom index
For the COSI, 84 responses were included in the results and analysis. For the pain domain, the mean score was 8.00 ± 3.87 out of a possible total of 17. For sexual symptoms, the mean score was 1.78 ± 1.62 out of a possible 5. For quality of life, the mean score was 7.23 ± 3.88 out of a possible score of 15.
Chronic prostatitis symptom index
For the CPSI, 77 responses were included in the results and analysis. The mean CPSI pain score was 10.66 ± 4.19 out of a possible total of 21. The mean urinary symptom score was 3.15 ± 2.94 out of 10. The mean quality of life score was 7.79 ± 3.04 out of a possible 15. A significant association was found between the CPSI pain score and the COSI pain score (Figure 1). The beta-coefficient for the regression was 0.693 (p < 0.001).

Scatter plot of the chronic prostatitis symptom index and Chronic Orchialgia Symptom Index (n = 77).
The American Urological Association symptom index/International prostate symptom score
A total of 75 responses to the AUA-SI/IPSS questionnaire were included. The mean total score for the questionnaire was 10.51 ± 8.99 out of a possible score of 35. Out of the responses, 37/75 (49.3%) were mildly symptomatic (0–7), 22/75 (29.3%) were moderately symptomatic (8–19), and 16/75 (21.3%) were severely symptomatic (20–35). When plotted against the COSI pain score, a significant association was found (Figure 2). The beta-coefficient for regression was 0.158 (p = 0.001).

Scatter plot of the international prostate symptom score total score and the Chronic Orchialgia Symptom Index pain score (n = 75).
Hip dysfunction and osteoarthritis outcome score
For the HOOS questionnaire, 81 responses were included in the analysis. The mean total score was 4.36 ± 5.06 out of a possible score of 24. One-third (27/81) of patients reported no hip pain or symptoms, 24.7% (20/81) reported a score between 1 and 4, and 42.0% (34/81) reported a score of 5 or above. When charted against the COSI pain score, a significant positive association was found (Figure 3). The beta-coefficient was 0.275 (p = 0.001).
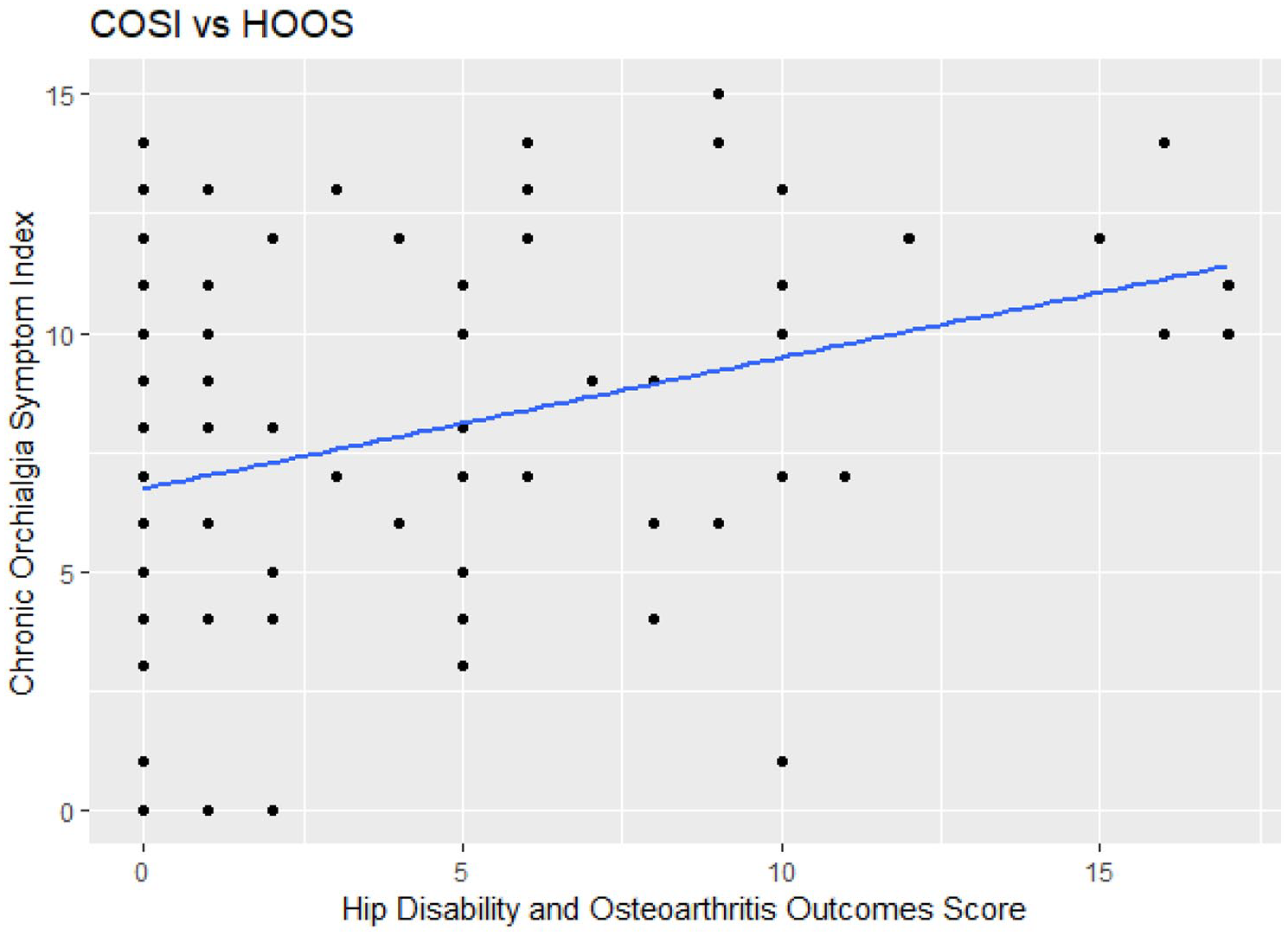
Scatter plot of the hip disability and osteoarthritis outcomes score total and the Chronic Orchialgia Symptom Index pain score (n = 81).
Oswestry low back pain questionnaire
For the Oswestry low back pain questionnaire, 83 responses were included in the analysis. The mean total score was 20.11% ± 18.21% out of a possible 100%. Using the established thresholds, 53/83 (59.6%) of patients had minimal functional disability (0%–20%), 21/83 (23.6%) had moderate disability (21%–40%), 14/83 (15.7%) had severe disability (41%–60%), and 1/83 (1.1%) would be classified as crippled (61%–80%). When compared to the COSI subjective testicular pain rating, a positive association was determined (Figure 4). The beta-coefficient was 0.109 (p < 0.001).
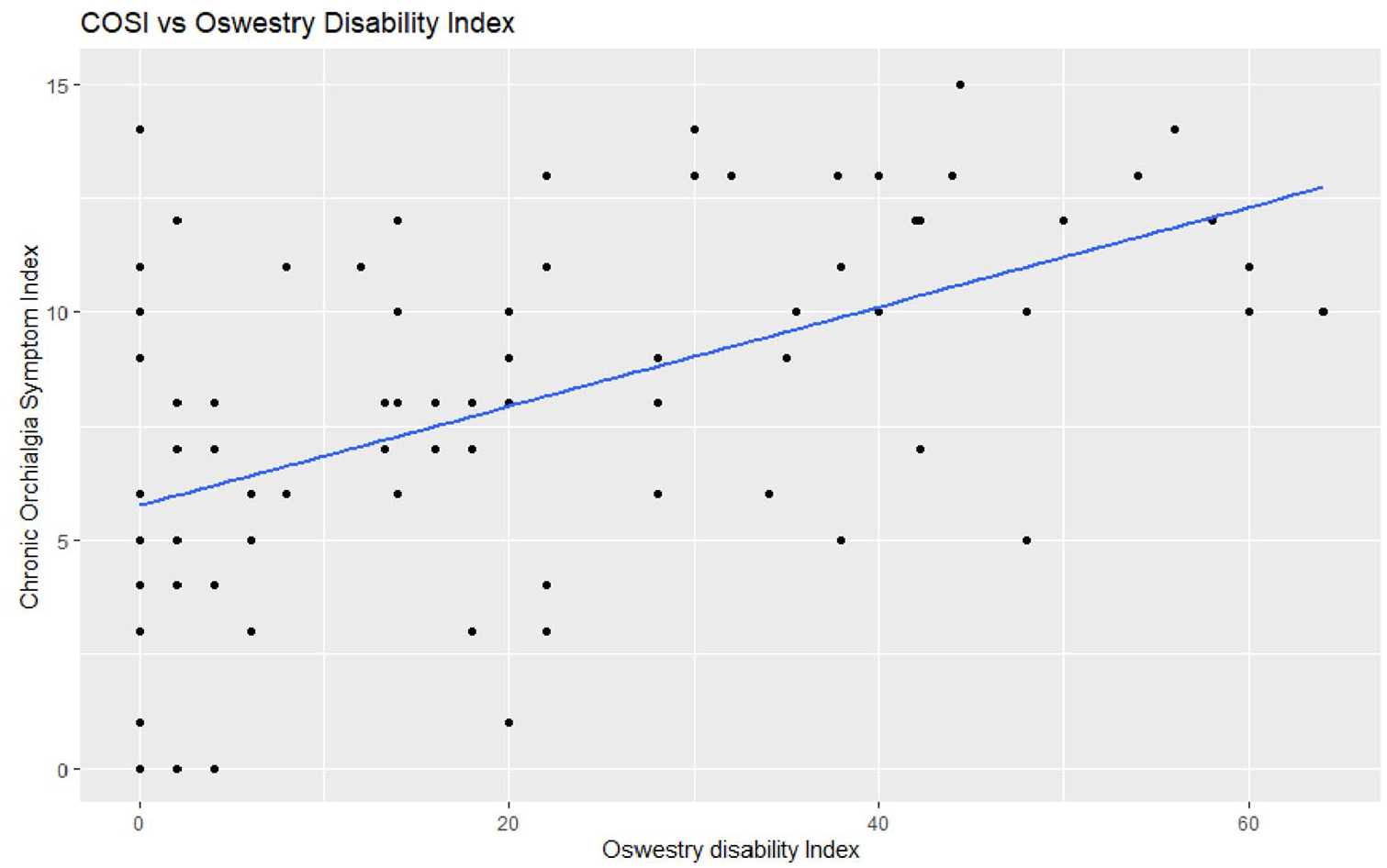
Scatter plot of the Oswestry disability index and the Chronic Orchialgia Symptom Index pain score (n = 83).
Patient health questionnaire-9
A total of 67 responses to the PHQ-9 were included in the analysis. The mean score for the PHQ-9 was 5.85 ± 5.88 out of a possible score of 27. Using the thresholds set by the PHQ-9, 10/67 (14.9%) of patients had no signs or symptoms of depression (0), 25/67 (37.3%) had minimal depression (1–4), 17/67 (25.4%) had mild depression (5–9), 9/67 (13.4%) had moderate depression (10–14), 3/67 (4.5%) had moderately severe depression (15–19), and 3/67 (4.5%) had severe depression (20–27). When plotting the PHQ-9 total score against the COSI pain score, a significant positive association was found (Figure 5). The calculated beta-coefficient was 0.233 (p = 0.003).

Scatter plot of the PHQ-9 total score and the Chronic Orchialgia Symptom Index pain score (n = 67).
General anxiety disorder-7
In total, 69 responses for the GAD-7 were included in the analysis. The mean score was 5.49 ± 6.16 out of a possible total score of 21. Using the stratifications provided by the questionnaire, 39/69 (56.5%) of patients reported minimal anxiety (0–4), 15/69 (21.7%) reported mild anxiety (5–9), 7/69 (10.1%) reported moderate anxiety (10–14), and 8/69 (11.6%) reported severe anxiety (15–21). When plotting the GAD-7 score against the COSI pain score, a positive association was found (Figure 6). The calculated ß-coefficient was 0.177 (p = 0.019).

Scatter plot of the GAD-7 total score and the Chronic Orchialgia Symptom Index pain score (n = 69).
International index of erectile function-5
A total of 51 responses to the IIEF-5 were included in the analysis. Questionnaires that were incomplete or marked no sexual activity were excluded. The mean score was 18.36 ± 6.21 out of a possible score of 25. Using the stratifications described by Rosen et al., 23/51 (45.1%) had no ED (22–25), 8/51 (15.7%) had mild ED (17–21), 11/51 (21.6%) had mild to moderate ED (12–16), 5/51 (9.8%) had moderate ED (8–11), and 4/51 (7.8%) had severe ED. A statistically significant negative association was found between the IIEF-5 score and the COSI pain score, indicating that lower IIEF-5 scores (more severe symptoms) were associated with higher pain scores (Figure 7). The calculated ß-coeficient was −0.192 (p = 0.025).
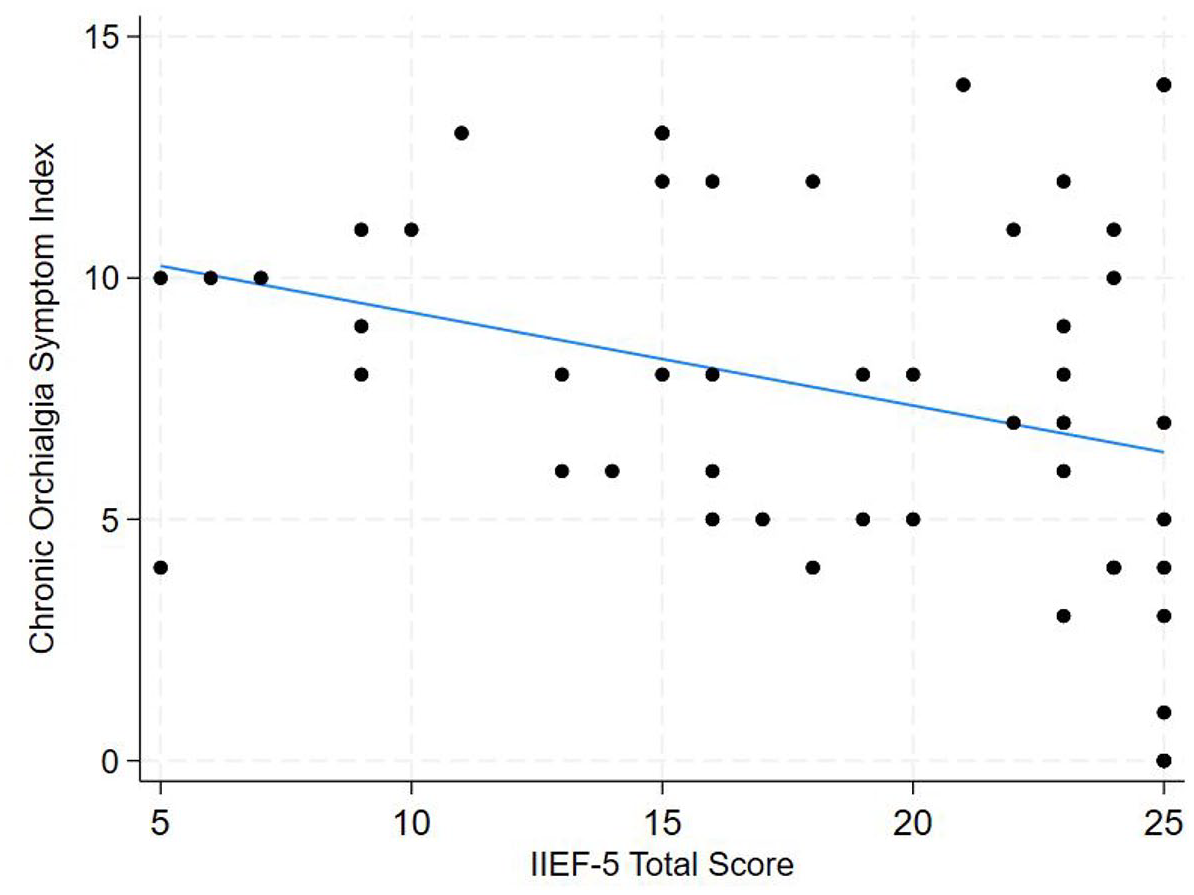
Scatter plot of the IIEF-5 total score and the Chronic Orchialgia Symptom Index pain score (n = 51).
Physical activity sign
A total of 42 responses to the Physical Activity Vital sign were reported. The mean number of days per week patients engaged in moderate to vigorous exercise was 3.22 ± 2.43 days. On the days patients exercised, the mean duration was 49.6 ± 72.9 min. The average total minutes per week of physical activity was 242.3 ± 407.7 min. For days per week spent on strength training, the mean was 0.92 ± 1.87 days.
Chronic orchialgia intake form
As part of standard clinical care, patients were asked to complete a comprehensive intake form at the time of presentation, with responses shown in Supplemental Figure 1. A total of 94 patients were included in the data. Patients reported a wide variety of testicular pain duration, quality, and frequency. While “sitting,” “standing,” and “walking” were activities reported to improve pain at the highest frequency (24/90, 17/90, 14/90, respectively), they were also the most common activities to worsen pain (32/82, 26/82, 36/82, respectively).
These patients also had a diverse range of previous urological and surgical history. Thirty-six of 92 patients reported having a possible injury or trauma to the scrotum. Some patients reported a history of STIs and UTIs (12/91 and 20/91, respectively), and 42% (39/92) reported being treated with antibiotics for the pain. For those who received antibiotics, over half reported that their pain did not change on antibiotic therapy (21/39). Only a minority of patients reported complete resolution (3/39) or improvement (7/39) with antibiotic therapy. Multiple patients also reported having inguinal/groin surgery (24/93), vasectomies (18/90), and other minimally invasive procedures (12/83). However, a majority of patients did not report having any of these potential risk factors.
Many of these patients had also seen multiple healthcare providers for their pain and reported having pain beyond their scrotum. Out of 90 patients, over half (47/90) reported seeing a pain management specialist about their pain, and 25 out of 89 patients reported also seeing a sports medicine specialist, orthopedic specialist, or physical therapist, as well. In addition to testicular pain, half of the patients reported experiencing chronic pain other than testicular pain at least half the time (45/90). A majority of patients reported having at least some lower back pain (60/90), and nearly half reported having at least some hip pain (45/91).
Regarding mental health and other social factors, over half of the respondents (45/89) reported being bothered by a low mood over the past month, and over half were bothered by their stress levels (53/88). Also, many patients reported having a lack of interest (30/87) and feeling lonely (28/89).
Discussion
Men presenting with CSCP are often complex patients. They frequently present with a variety of symptoms, and the source of pain is often unknown. And, despite how common this condition is, there is a lack of research regarding CSCP and its effects on patients. Therefore, we conducted this study to better understand the urinary, sexual, musculoskeletal, and mental health concerns of this patient population. Specifically, we looked at symptoms and functional impairments, including testicular and urinary pain, PFD, back pain, hip pain, depression and anxiety, and exercise. There was significant collinearity between these different measurements, and this could lead to delayed care by patients being sent to different clinics that may be unable to solve their underlying condition.
One often overlooked cause of CSCP is spinal cord/back pathology. Multiple case reports have looked at patients presenting with both chronic testicular/scrotal pain and low back pain. In many of these cases, treatment of the spine pathology led to significantly improved lower back pain and almost complete regression of testicular pain.21 –23 One aim of our study was to increase understanding of low back pathology symptoms in a larger population of CSCP patients. Using the Oswestry low back pain disability questionnaire, we found that approximately 40% of patients with CSCP experienced additional low back pain symptoms that were greater than minimal functional disability, with 23.6% reporting moderate disability and 16.8% reporting severe disability symptoms. In addition, we found a positive association where patients with worse scrotal pain symptoms were more likely to experience back pain symptoms. The data suggest that spinal cord/back pathology may be present in many men presenting with CSCP. Because spinal cord/back pathology has the potential to be the source of CSCP and does not appear to be uncommon, additional screening may be necessary in these patients.
Hip pathology has also been theorized to be a source of CSCP, but very little research has been conducted. In a recent study of 10 men reporting scrotal or testicular pain lasting > 3 months who had undergone a hip MRI, they found overt labral tears in eight men and labral fraying in the remaining two. 24 Five men underwent hip injection with a steroid and local analgesia directed at their hip pathology, with two reporting lasting resolution of pain and two reporting significant improvement. 24 An additional two men had complete resolution with 8 weeks of physical therapy. 24 Because of the potential link between hip pathology and chronic scrotal/testicular pain, we wanted to better characterize hip signs and symptoms in a larger sample of CSCP patients. Using the HOOS JR. Questionnaire, we found that a majority of CSCP patients (66.6%) had some degree of hip symptoms present. While there are no defined cutoffs for hip disability, the data suggest that these patients have a wide range of hip disability. Furthermore, those who had more severe hip pain also tended to rate their subjective scrotal pain higher, as well. Due to the high prevalence of apparent hip pain/disability in this population, hip pathology should be investigated as part of the standard of care for these patients.
PFD is another important factor to consider when treating patients with CSCP, as it may be a cause for the pain and may also impact treatment efficacy. According to a recent study by Murthy et al., microscopic spermatic cord denervation, one of the potential treatments for CSCP when primary conservative methods fail, has a significantly higher failure rate in patients with PFD. 25 In addition, pelvic floor physical therapy has been suggested as a viable treatment for reducing pain when PFD is present. Considering how important PFD can be for the diagnosis and treatment of CSCP, we wanted to make sure we assessed PFD in the CSCP patient population, which is why we utilized the NIH-CPSI, AUA-SI/IPSS, and the IIEF-5. We found many of our patients to have symptoms indicative of PFD. Over half of patients had moderate-to-severe urinary symptoms according to the AUA-SI/IPSS, and pain in the pelvic region was a common complaint. In addition, we found a positive association between CSCP and sexual dysfunction severity. All of these results support the current literature, which suggests chronic scrotal pain and PFD are interconnected. Thus, PFD should be consistently screened for in patients with CSCP to help with diagnosis and treatment.
Chronic pain conditions have been commonly associated with depression and anxiety, but few studies have focused on CSCP and its effect on mental health. In one study, 31% of patients with CSCP complained of depressive symptoms more than half the days of the month, with more severe pain levels correlating with higher rates of depression. 26 We wanted to build on this work by using a more robust scale for depression, as well as assessing for anxiety. Based on our results, we found that mental health concerns are indeed prevalent in this patient population. Using the PHQ-9, we found that 47.8% of patients reported having depressive symptoms in the past 2 weeks that would qualify them for mild depression or worse. 43.5% of patients reported having anxiety symptoms over the past 2 weeks, ranging from mild to severe anxiety according to the GAD-7. Furthermore, both anxiety and depression appear to be positively associated with subjective testicular pain, indicating that mental health concerns are a serious concern when treating these patients. Because of how intertwined it appears mental health is with CSCP, it becomes paramount to assess mental health as part of patient evaluation.
Exercise and chronic pain have an almost paradoxical relationship. On one hand, chronic pain can lead to poor physical function and act as a barrier to patients performing the physical activities they enjoy. However, historical evidence has supported physical activity as an efficacious method for treating pain. 27 And, in addition to modulating pain, multimodal exercise programs that utilize a range of activities have been shown to improve physical function and sleep, as well as elevate patients’ moods, leading to improved mental health. 27 Due to the importance of physical activity for general health and its role in chronic pain conditions, we wanted to determine how much physical activity patients with CSCP were completing each week, which we assessed using the physical activity vital sign. Our results showed that in the CSCP population, there was a wide variation in exercise habits. Based on the recommendations by the Department of Health and Human Services of 150 min of moderate exercise and 2 days of strength training, our patients are generally not meeting the strength training guidelines. 28 Because of this, patients may not be experiencing the potential benefits of exercise. While specific recommendations to guide patients and providers on specific parameters are still lacking, clinicians should still encourage patients to engage in physical activity that is tailored to their individual needs and abilities.
Our study is not without limitations. Patients were not required to answer all questions in any of the questionnaires, resulting in some incomplete surveys. In addition, not all patients received all of the questionnaires described, lowering the sample size for some of the questionnaires we reported in our study. Furthermore, many of the questionnaires administered are validated for people presenting with other conditions, not necessarily those presenting with CSCP. Therefore, the results of these questionnaires do not imply that these other conditions/symptoms cause or are necessarily associated with CSCP, only that they coexist at the time the questionnaires were completed. Lastly, we did not perform formal ordinal regression because of the lack of a control group in our sample and overall difficulty with controlling for confounders, limiting the predictive value of such models. While the relationships we found were significantly nonzero, there is a possibility that these relationships are not clinically significant or may not meaningfully change patient management.
Despite these limitations, our study provides a valuable glimpse into this difficult-to-treat patient population. Our results add to the growing literature that those with CSCP are complex in their presentation and possible etiologies, supporting the argument for a multidisciplinary approach to the evaluation and management of CSCP.
Future studies, including a larger study with formal regression and more robust control for confounding, are needed to further determine which questions and questionnaires are most important to use when evaluating patients presenting with CSCP. While a thorough interview and physical examination are the gold standard, time is often a constraint for many practicing clinicians. Our study provides a foundation for potential questions that should be asked of all CSCP patients, but more work needs to be done to narrow down the relevant questions. Ultimately, the goal is to help contribute to the literature needed to create a standardized approach for diagnosing and treating CSCP.
Conclusion
Patients with CSCP may present with many co-occurring symptoms, but this common and often debilitating condition is poorly understood. We found that patients in our clinic population present with a wide variety of pain, both in terms of severity and location. PFD symptoms, urinary symptoms, and symptoms of depression and anxiety also appear to be very prevalent in this population. Furthermore, we found many patients had symptoms dealing with their back and hip function, something that has not been studied in larger samples of CSCP patients. All these results point to a need to be thorough while interviewing patients with this complex condition. Further research is needed to better develop a standardized approach to these patients and assess how directed interventions on associated symptoms impact CSCP management.
Supplemental Material
sj-docx-1-tau-10.1177_17562872251348009 – Supplemental material for Characterizing patients with chronic scrotal content pain: a retrospective review of clinical presentations
Supplemental material, sj-docx-1-tau-10.1177_17562872251348009 for Characterizing patients with chronic scrotal content pain: a retrospective review of clinical presentations by Jacob Lam, Emily Solsrud, Alexander Hart, Abigail Moore and Amy Pearlman in Therapeutic Advances in Urology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.