
Abstract
Abstract
The endocannabinoid system (ECS) primarily consists of cannabinoid receptors (CBRs), endogenous ligands, and enzymes for endocannabinoid biosynthesis and inactivation. Although the presence of CBRs, both CB1 and CB2, as well as a third receptor (G-protein receptor 55 [GPR55]), has been established in the gastrointestinal (GI) tract, few studies have focused on the role of cannabinoids on esophageal function. To date, studies have shown their effect on GI motility, inflammation and immunity, intestinal and gastric acid secretion, nociception and emesis pathways, and appetite control. Given the varying and sometimes limited efficacy of current medical therapies for diseases of the esophagus, further understanding and investigation into the interplay of the ECS on esophageal health and disease may present new therapeutic modalities that may help advance current treatment options. In this brief review, the current understanding of the ECS role in various esophageal functions and disorders is presented.
Overview of Endocannabinoid System
The endocannabinoid system (ECS) primarily consists of cannabinoid receptors (CBRs), endogenous ligands, and enzymes for endocannabinoid biosynthesis and inactivation. 1 The ECS plays an important role in regulation of synaptic transmission in the central and enteric nervous systems (ENS) through both excitatory and inhibitory effects, mediating a variety of physiological processes including pain sensation and modulation, motor function, inflammation, and immunity. 2
CBRs belong to the superfamily of G-protein-coupled receptors and are expressed in two main forms, CB1 and CB2. 3 CB1 is mainly expressed in central and peripheral neurons, including the ENS, whereas CB2 is mostly expressed by inflammatory/immune cells.4–6 The ubiquitous distribution of CBRs in the ENS and gastrointestinal (GI) tract highlights its role in GI health and disease including motility, inflammation and immunity, intestinal and gastric acid secretion, nociception and emesis pathways, and appetite control7–9 (Table 1).
CNS, central nervous system; GERD, gastroesophageal reflux disease; GI, gastrointestinal; GPR55, G-protein receptor 55.
The CB1 receptor plays a role in intestinal motility by attenuating both large and small bowel muscle tone when activated.10–13 Within the upper GI tract, activation of CB1 decreases intragastric pressure and delays gastric emptying through inhibition of excitatory neurons.14,15 As demonstrated in rodent models, CB1 receptors play a role in energy regulation by driving consumption of food high in dietary fat. 16 After sham feeding in rats with high-fat foods, upregulation of CB1 receptors was found in rat small intestine, leading to inhibition of neural signaling events of satiety to suppress feeding. These findings suggest that CB1 acts through a positive feedback loop after dietary fat exposure to stimulate further consumption of higher energy foods. In another study, pharmacological inhibition of CB1 led to decreased amount of refeeding in rats after food deprivation, highlighting CB1 receptor's role in appetite regulation. 17 In addition, CB1 was found to be upregulated in rats fed a high fat, high caloric Western diet (WD). It was also suggested to play a role in hyperphagia after antagonism of CB1 with an inhibitor led to decreased food intake in rats fed a WD for 60 days. 18
CB2 receptors located in the central nervous system (CNS) have been shown to play a role in the emetic pathway; however, the receptor has also been found in inflammatory tissue and immune cells (plasma cells and macrophages) throughout the GI tract.19–22 CB2 is expressed in the GI tract but less extensively than CB1 receptors. 23 Evidence that upregulation of CB2 receptors occurs in patients with inflammatory bowel disease suggests that these receptors play a critical role in colonic inflammation. 7 Distinct from CB1 receptors effect on motility, CB2 receptors may further regulate motility in pathophysiological states with its expression being upregulated in inflammatory disease states.5,24
Presence of CBRs in human esophageal epithelium was first demonstrated in a study comparing patients with nonerosive esophageal reflux disease (NERD) and erosive esophageal reflux disease (ERD) to normal controls. 25 The authors found increased expression of CB1 mRNA in NERD patients compared with erosive esophagitis, but overall less expression compared with normal controls. Interestingly, CB1 protein expression was similar to patients with ERD, whereas NERD patients showed increased CB1 receptor levels when compared with healthy controls (Fig. 1). Although other GI inflammatory conditions have increased CB1 activity, there may be contribution of the inflammatory microenvironment that alters CB1 gene expression. 24
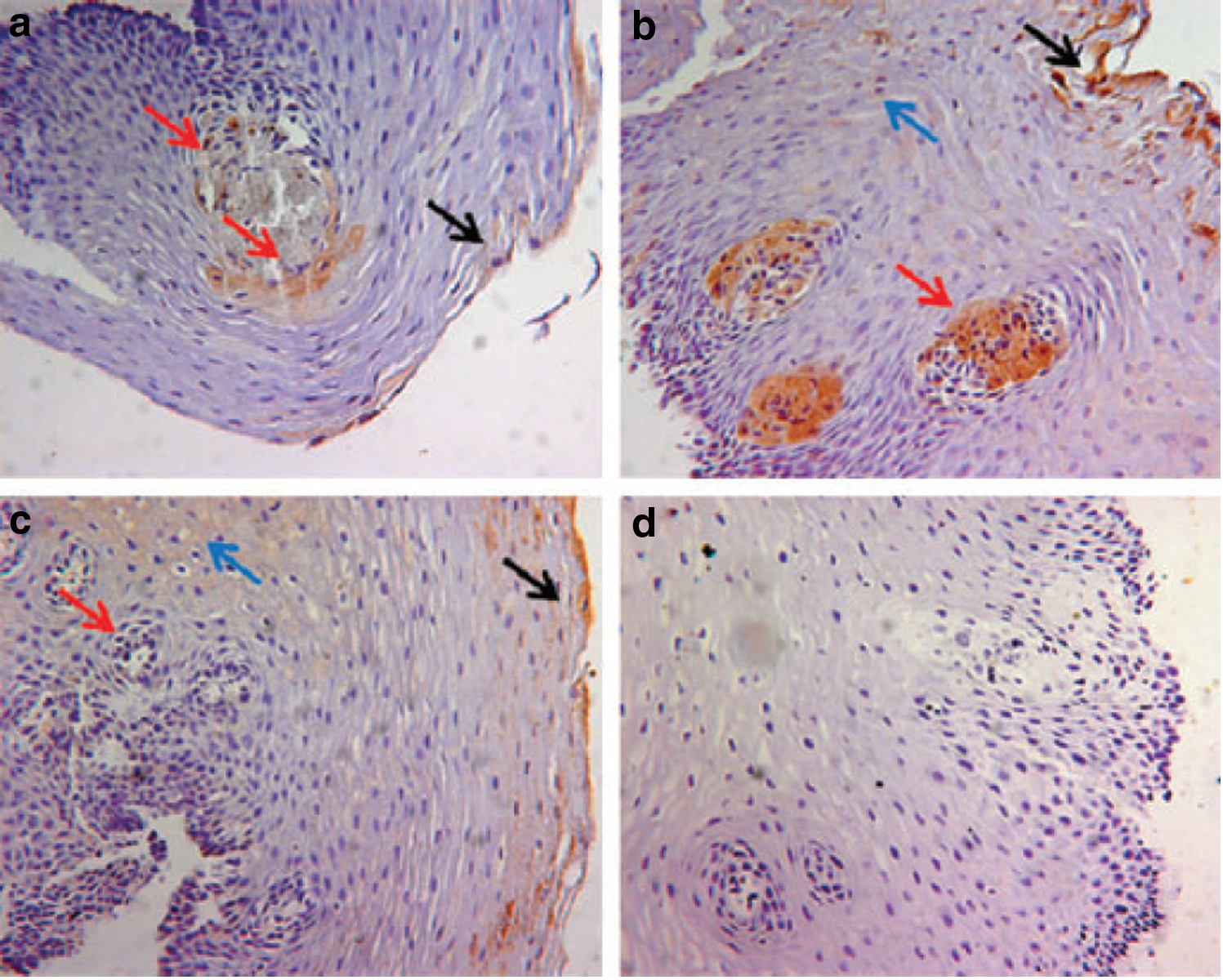
Immunostaining of CB1 receptor in histological sections of esophageal mucosa. Healthy subjects
Recently, a potential third CBR has been identified with implications in the GI tract. G-protein receptor 55 (GPR55) shares 13–15% sequence homology with the CB1 and CB2 receptors and responds to a multitude of endogenous and exogenous cannabinoid ligands as well as several lipids. 26 A recent study found activation of GPR55 after administration of a synthetic agonist slowed down whole-gut transit in mice in vivo, suggesting GPR55 may be involved in the regulation of gut motility. 27
Endocannabinoids are endogenously produced ligands that exert effects on CBRs. The major ligands, anandamide (AEA) and 2-arachidonylglycerol (2-AG), play a role in maintaining GI homeostasis and have been found at increased levels in GI disease states, including celiac disease, diverticulosis, and colorectal cancer.28–30 Exogenous cannabinoids, both plant-derived phytocannabinoids (cannabis sativa) and synthetic cannabinoids, also directly activate CBRs. They have been shown to play a role in both GI pathophysiology (e.g., cannabinoid hyperemesis syndrome) and therapies (e.g., antiemetics and appetite stimulant). 31
Although both CB1 and CB2 receptors have been found in the esophagus, few studies have focused on the role of cannabinoids on esophageal function. 21 Thus far, the role of GPR55 in esophageal motility has not been established. Given the varying and sometimes limited efficacy of current medical therapies for diseases of the esophagus, further understanding and investigation into the interplay of the ECS on esophageal health and disease may present new therapeutic modalities that may help advance current treatment options. In this review, the current understanding of the role of ECS in various esophageal functions and disorders is presented.
Swallowing Mechanism
The swallowing reflex is an important mechanism in controlling acid exposure in the esophagus, whereby increased swallowing decreases stasis and reduces acidic and nonacidic reflux. The role of the swallowing reflex in reducing reflux has been demonstrated after observation that supine sleeping patients experienced a decreased spontaneous swallowing reflex during 24-h pH monitoring, leading to increased acid and nonacid exposure. 32 CB1 receptor activation has been shown to decrease spontaneous swallows in human and animal studies. One study on dogs found administration of CB1 agonist suppressed spontaneous swallowing in a dose-dependent manner with an >80% decrease in spontaneous swallows at high doses (57 nmol/kg). 33 The authors noted that although administration of CB1 agonist decreased transient lower esophageal sphincter relaxations (TLESRs) thereby decreasing reflux events, the concomitant decrease in spontaneous swallows and clearance of refluxate potentially limit the benefits of decreasing TLESRs. The mechanism of action of CBRs on swallowing mechanism is likely centrally located through endogenous cannabinoid action, modifying synaptic neurotransmitter release. 34 The swallowing reflex, evoked by repetitive electrical stimulation of the superior laryngeal nerve in rats, was analyzed with and without combinations of both CB1 and CB2 agonists and antagonists. CB1 receptor antagonist injected directly into the nuclear tractus solitarius blocked the action of intravenous-administered CB1 agonist. The only study in humans to date found administration of the combination CB1/CB2 agonist Δ9-THC resulted in a significant reduction in the number of swallows wherein high doses (20 mg) led to a reduction in spontaneous swallows by 50%. 35
Esophageal Motility
CBRs, specifically CB1, play a role in GI motility and have mainly been studied in the small intestine and colon.8,10 Only two studies have evaluated the effect of ECS on esophageal motility in humans.35,36 Administration of Δ9-THC decreased basal lower esophageal sphincter (LES) pressure in a nondose-dependent manner, with onset occurring 45 min after meal ingestion, maximal effect around 100 min, followed by slow recovery. 35 This was confirmed in another human study that administration of rimonabant, a CB1 receptor antagonist, increased postprandial LES pressures in the first and second postprandial hours. 36
Previous studies in animal models did not demonstrate CBR action influenced esophageal motility. Lehman et al. demonstrated that CBR agonism did not influence the extent of LES relaxation. Similarly, CBR antagonists had no influence on esophageal peristalsis. 33 A recent case report suggested that exogenous phytocannabinoid use improved symptoms of dysphagia in a patient with manometric findings, consistent with type 3 achalasia. 37 Others have suggested that exogenous cannabinoid use, like chronic opiate use, may produce motor findings similar to type 3 achalasia. 38 The conflicting data support the need for further study of endo- and exogenous cannabinoids on esophageal motility. 39
Gastroesophageal Reflux Disease and TLESRs
TLESRs are the predominant mechanism seen in gastroesophageal reflux disease (GERD). TLESRs occur after gastric stimuli, mainly distension, to relieve counteracting gastric pressure on the LES.40,41 The LES response to gastric distension is vagally mediated through communication of the LES and crural diaphragm with afferent gastric pathways, brainstem integrative centers (nucleas tractus solitarus and dorsal motor nucleus), and efferent inhibitory pathways. 41 The action of CBRs on TLESRs and GERD was first demonstrated in animal models after the observation that administration of a CB1 agonist (WIN55,212-2) reduced the rate of TLESRs without altering the TLESRs latency or esophageal peristalsis. 33 The authors concluded that the action of the CBRs on TLESRs most likely occured via central pathways because no effect on the extent of LES relaxation was seen.33,42,43 Absence of CB1 receptors in preganglionic vagal motor neurons projecting to the gastric fundus or LES further supports the assumption that CB1 does not directly participate in vagal motor output modulation and rather relies on central activation. 42
Interestingly, the use of a CB1 receptor antagonist (rimonabant) in healthy human subjects enhanced postprandial LES pressure but unexpectedly decreased TLESRs. 36 This contradicts earlier data in an animal model with dogs that showed rimonabant enhanced the rate of TLESRs and reflux events that received acidified meal and intragastric air insufflation. 36 The authors attributed this discrepancy to different dosage, bioavailability, or interspecies differences of rimonabant. A possible explanation for the similar results from administrating CBR antagonist and agonists may be a result of rimonabant exerting potent CB1 receptor-independent pharmacological effects. 44
Gastric accommodation may affect TLESRs and play an important role in development of GERD. 45 Previous studies evaluated the effect of CB1 receptors on pain sensation during intragastric balloon distension, however, they did not find modulation of CB1 receptors with rimonabant-influenced mechanosensitivity of the proximal stomach. 46 It should be noted that baclofen has been shown to decrease TLESRs rate and increase basal LES pressure while not affecting meal-induced fundic accommodation, suggesting that the mechanism may not be as simple as binary, an observation previously suggested by Lehmann et al. 33 Other studies have suggested that using Δ9-THC inhibits gastric insufflation-induced LES relaxations in the decerebrate ferret, highlighting the need for further clarification of the relationship between gastric stimulation and TLESRs. 10
The effect of CBRs on gastric emptying has been studied in humans although the data are limited and conflicting.48–51 Although there may be some influence of CBRs, gastric emptying itself does not necessarily correlate with fundus accommodation and activation of TLESRs.
The presence of CBRs in the esophagus, specifically those affecting TLESRs, offers a potential therapeutic target for treating GERD. Using Δ9-THC, Beaumont et al. demonstrated decreased rate of TLESRs in healthy volunteers who received 10 and 20 mg of Δ9-THC on three occasions a week apart. 35 Delta(9)-THC significantly reduced the number of TLESRs and caused a nonsignificant reduction of acid reflux episodes in the first postprandial hour. In addition, lower esophageal sphincter pressure and swallowing were significantly reduced by Δ(9)-THC. 35 However, in the high dose of Δ9-THC (20 mg) group, central activity led to increased nausea and vomiting. Centrally acting CB1 receptor agonists produce the psychotropic effects and, therefore, selective targeting of peripheral CB1 receptors is necessary for effective therapy, with recent efforts to develop higher potency and effective CB1 agonists.52,53 Previous studies have looked at using CB1 antagonists; however, their therapeutic use is also limited by its side effect of major depression. 54
Newer methodologies for understanding the pharmacodynamics and pharmacokinetics of medication effects on TLESRs have been developed that may provide more accurate modeling of drug concentrations and their effects. 55
Bronchoconstriction
In patients with a chronic cough where lung disease, environmental exposure, and medications have been excluded, GERD is often a major cause. 56 The two main mechanisms implicated in reflux-related cough are microaspiration of refluxate and stimulation of vagal innervation of the esophagus, leading to esophagobronchial reflex arc. The CB2 receptor has been shown to play a role in inhibiting bronchoconstriction and microvascular leakage in reflux models using guinea pigs. After infusion of intraesophageal HCl, the inhibitory effect of bronchoconstriction by a CB1 agonist (WIN55,212-2) was blocked after administration of a CB2 antagonist (SR 144528) but not after CB1 receptor antagonist, demonstrating CB2 receptor's role as a downregulatory mechanism of sensory nerve activation. 57 CB2 receptor activation in models of direct airway damage has been shown to play an active role in reducing inflammation, potentially supporting protective role of CB2 in microaspiration of refluxate. 58
Visceral Hypersensitivity and Pain
Functional esophageal disorders are defined as the presence of esophageal symptoms in the absence of structural, inflammatory, or motor abnormalities. 59 Proposed pathophysiological mechanisms include alterations in neural processing between peripheral triggers and central perception of esophageal symptoms. 60 CBRs likely play a role in pain sensation and modulation through visceral antinociceptive action. 61 Previous studies have demonstrated an analgesic effect of cannabinoids in animal models through both CB1 and CB2 activation.62–64 In one important study, upregulation of the endocannabinoid AEA through inhibition of its degrading enzyme led to an attenuated behavioral response to noxious stimuli in rodents. 65 This suggests a central role of CB1 receptors in mitigating pain-related inputs to the CNS.
There are few studies of visceral sensitivity in the esophagus and the effects of CBR modulation. In a randomized, placebo controlled trial, administration of dronabinol for 1 month increased the threshold for first sensation, pain frequency, and intensity of pain during an esophageal balloon distention test. 66 Notably, anxiety and depression indices were unchanged after dronabinol administration. The mainstay of functional esophageal disorders relies on tricyclic antidepressants, selective serotonin reuptake inhibitors, and serotonin norepinephrine reuptake inhibitors, all of which have been found to influence psychiatric parameters, highlighting a possible difference in mechanism of action. 60
Role in Esophageal Neoplasm
Cannabinoids inhibit tumor cell growth and induce apoptosis by modulating cell signaling pathways. 67 Decreased frequency of CNR-1 gene, the gene encoding CB1 receptor, expression was found in tissue of esophageal cancer patients (10.8%) compared with controls (60.0%), and its presence is considered an independent predictor of survival. 68 However, recently a multivariate analysis revealed that CB1 receptor overexpression was independently associated with poor prognosis (p=0.019). Biological analysis of CB1 receptor overexpression using esophageal squamous carcinoma cell lines revealed that CB1 receptor activation appeared to promote cell proliferation and invasion. 69 Thus, the role of CB1 receptor expression in tumorogenesis needs to be further evaluated.
Conclusion
A more thorough understanding of the ECS in esophageal function and disease is needed. Recently, there has been a push to legalize cannabis for both medicinal and recreational use. There have also been reports of increasing use of both plant-derived cannabis and synthetic cannabinoids in the United States. 70 This may allow additional studies to be added to the few human studies to date on the effect of cannabinoid use in humans. Further study in this area is imperative for the development of future therapeutic potential of utilizing the ECS.
Authors' Contributions
J.G. was involved in literature review and is the primary author. R.K. was involved in literature review. R.S. was involved in study conceptualization and reviewed the article.
Footnotes
Author Disclosure Statement
No competing financial interests exist.