
Abstract
A low socioeconomic status (SES) has been linked to disproportionate access to health care in many diseases, leading to worse disease severity at initial presentation. There is a paucity of these data in the pulmonary hypertension (PHTN) population. We studied the association of SES, as measured by zip code–based median annual household income, with World Health Organization functional class (WHO-FC) at time of first evaluation in PHTN patients. All patients evaluated at our center with a right heart catheterization revealing a mean pulmonary artery pressure of ≥25 mmHg within 12 months of initial evaluation were considered for the study. Demographics, WHO-FC, and zip codes were obtained from retrospective chart analysis. The 2010 US census was used to obtain zip code–based annual median income. The income groups were divided into quartiles. Patients were categorized by their WHO-FC and zip code–derived median income. Similar analyses were conducted for pulmonary arterial hypertension (PAH) patients. Survival was estimated with the Kaplan-Meier method. Data were analyzed in SAS, and P < 0.05 was considered significant. There were 228 PHTN patients (70 [30.7%] male, 158 [69.3%] female). As median income decreased, the FC at presentation increased, signifying higher disease severity (Spearman correlation: r = −0.161, P < 0.0515). This association between median income groups and WHO-FC at initial evaluation was significant (χ2 test: P < 0.0168). There were 116 PAH patients (32 [27.6%] male, 84 [72.4%] female). There was again a negative relationship between income and initial FC (Spearman correlation: r = −0.0307, P < 0.0007). A lower SES was associated with worse disease, as measured by WHO-FC.
Keywords
Socioeconomic status (SES) is a combination of sociological and economic factors that combines a family's work experience, income, and social status in relation to others in the same economy. Access to health care is defined by the Institute of Medicine as the timely use of personal health services to achieve the best possible outcome. 1 In the United States, persons with a lower SES suffer disproportionately from many diseases and show a higher rate of mortality than those with a higher SES.1,2 In addition, a lower SES has been linked to disproportionate access to health care in many diseases, which leads to poor health outcomes. 1 In pulmonary medicine, the relationship with SES has been studied in a few chronic conditions, such as chronic obstructive pulmonary disease (COPD), 3 asthma, 4 and cystic fibrosis. 5 However, there is a paucity of similar data in the population of patients with pulmonary hypertension (PHTN).
Pulmonary arterial hypertension (PAH) is a rare and devastating form of PHTN characterized by progressive increases in pulmonary vascular pressure and pulmonary vascular resistance that eventually may lead to right ventricular failure and death. 6 For this reason, early diagnosis and treatment are critical for preventing disease progression. Unfortunately, the diagnosis of PAH is often difficult to make and can require multiple physician visits and referral to a medical specialist (i.e., cardiologist, pulmonologist) with specific training in pulmonary vascular disease. For these reasons, the mean time between onset of symptoms and diagnosis is more than 2 years, despite the increased awareness of the disease. Despite the development of numerous therapies over the past 20 years, the delay to diagnosis has not decreased over the past 3 decades.7,8 Right heart catheterization (RHC) is needed to make the diagnosis of PAH and distinguish it from other forms of PHTN. RHC is a costly, hospital-based, invasive procedure and may not be readily accessible to people with a lower SES. 9 It has been reported that SES affects outcomes in PAH, 10 but there is limited information on how SES affects clinical presentation and disease severity at time of diagnosis. We decided to study the effect of SES on PHTN disease severity at the time of initial presentation.
METHODS
Patient population
We conducted a retrospective review of data collected on 243 consecutive PHTN patients (World Health Organization [WHO] groups 1–5) who were initially seen at the Advanced Lung Disease Center at North Shore–Long Island Jewish Medical System from 1998 to September 2013. Patients who had RHC before or up to 1 year after initial evaluation with a mean pulmonary artery pressure (mPAP) of ≥25 mmHg were included the study. Patients who had an mPAP of ≥25 mmHg, a pulmonary capillary wedge pressure (PCWP) of <15 mmHg, and no significant left heart or chronic lung disease were classified as having PAH, as per WHO classification. 11
SES determination
It is customary for our patients, at the time of initial evaluation, to fill out a registration/demographics form that includes address, zip code, and referring physician. Data were collected retrospectively from patient demographic sheets taken at initial registration on which patients provided zip codes. The 2010 US Census Bureau American FactFinder web program (http://factfinder.census.gov) was used to obtain information on median household income based on patient-provided zip codes. This methodology has been validated as a marker of SES, according to the Agency for Healthcare Research and Quality (http://www.ahrq.gov). In addition, it has been found that census-based aggregate variables such as zip code are a viable proxy for SES. 12 This study was approved by the North Shore–Long Island Jewish Medical System Institutional Review Board (IRB 14–202A).
PHTN severity measures
The dependent variable measure to determine PHTN disease severity relies heavily on functional capacity. The clinical severity of PHTN was classified according to a system originally developed for heart failure by the New York Heart Association and then modified by the WHO for patients with PHTN. 13 Functional-class (FC) assessment divided the patients into three groups—WHO-FC I or II, III, and IV—based on National Institutes of Health registry average survival by WHO-FC. 7
Statistical analysis
PHTN at initial presentation was defined as an RHC before or up to 1 year after initial evaluation with an mPAP of ≥25 mmHg. PAH was defined as an RHC in the same time frame but with mPAP ≥ 25 mmHg and PCWP < 15 mmHg.
Separate analyses were carried out for PHTN and PAH. Associations between categorical factors were examined with the χ2 or the Fisher exact test, as appropriate. Relationships between continuous factors were examined by calculating the Spearman correlation coefficient. The association between age at first contact and median income was examined with the Mann-Whitney test. Not all variables met the assumptions required for parametric tests (i.e., t test, Pearson correlation); therefore, nonparametric tests (i.e., Mann-Whitney test, Spearman correlation) were used for all analyses for consistency. For median income and FC, survival was estimated with the KaplanMeier product-limit method, and the log rank test was used for comparisons. Both factors and their interaction were then included in a Cox regression to examine the joint effects of median income and FC on survival. All analyses were performed in SAS, version 9.3 (SAS Institute, Cary, NC). Results were considered statistically significant at an α level of 0.05.
RESULTS
Of the 243 patients with PHTN, 228 of them had an RHC either before or within 12 months after their initial visit to our center and were included in this study. Of these patients, 70 (30.7%) were male and 158 (69.3%) female. At initial presentation, their mean age was 61 years (standard deviation: 15 years). Zip code–based median annual household income ranged from $34,804 to $157,907, with a median of $77,352. Patient demographics are presented in Table 1. Median annual household income was divided into quartiles (<$60,530, $60,530–$77,352, $77,352–$94,678, and >$94,678).
Patient demographics
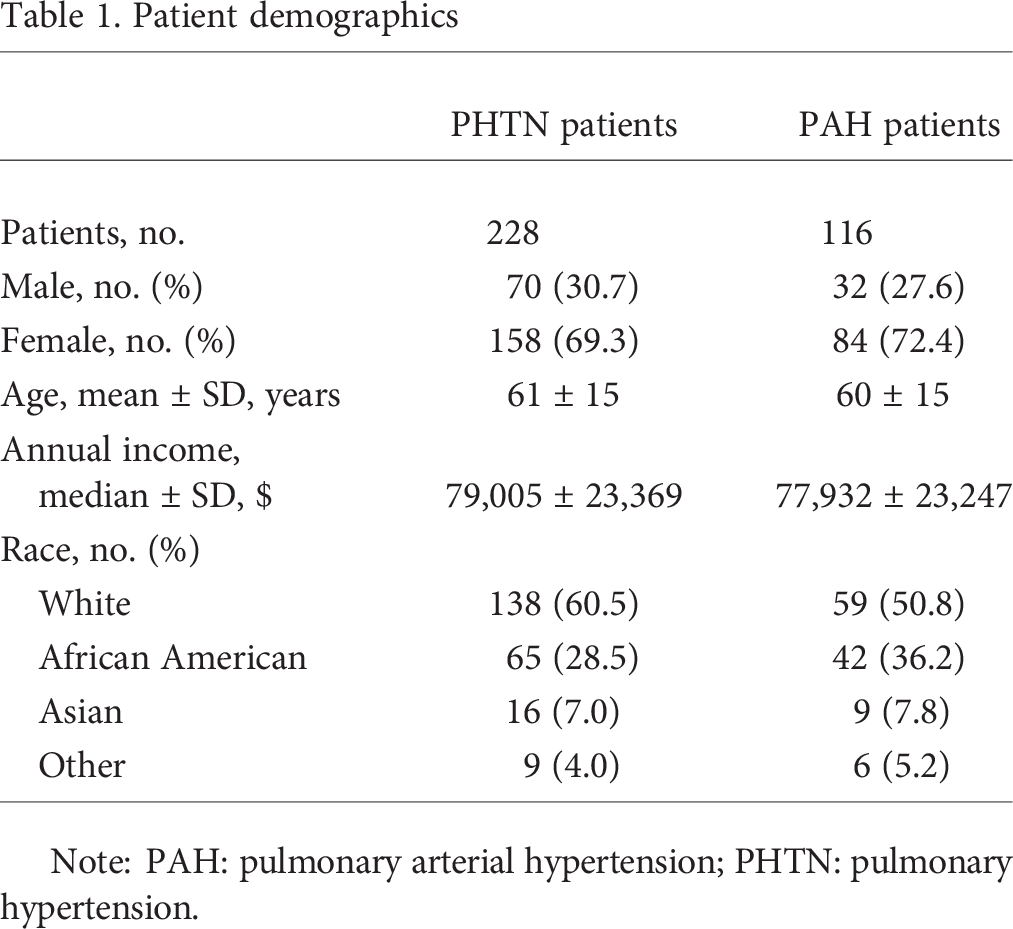
Note: PAH: pulmonary arterial hypertension; PHTN: pulmonary hypertension.
For patients with PHTN in the lowest quartile income group, 14 (24.6%) were in WHO-FC I/II at initial presentation and 43 (75.4%) in WHO-FC III/IV. For the second-lowest income quartile, 13 (23.6%) were in WHO-FC I/II at initial presentation and 42 (76.4%) in WHO-FC III/IV. For the third income quartile, 28 (47.5%) were in WHO-FC I/II at initial presentation and 31 (52.5%) in WHO-FC III/IV. For the highest income quartile, 22 (38.6%) were in WHO-FC I/II at initial presentation and 35 (61.4%) in WHO-FC III/IV (χ2 test: P < 0.0168; Table 2; Fig. 1). There was a negative relationship between WHO-FC and income in the PHTN cohort (Spearman r = −0.161, P < 0.0151). WHO-FC at time of initial presentation was a strong predictor of long-term survival in patients with PHTN. Analysis of the Kaplan-Meier curve revealed that survival was significantly better for patients in FC I or II than for those in FC III and better in FC III than in FC IV, as previously described in the literature.7,14
World Health Organization functional class (WHO-FC) at diagnosis in relation to socioeconomic status in pulmonary hypertension patients
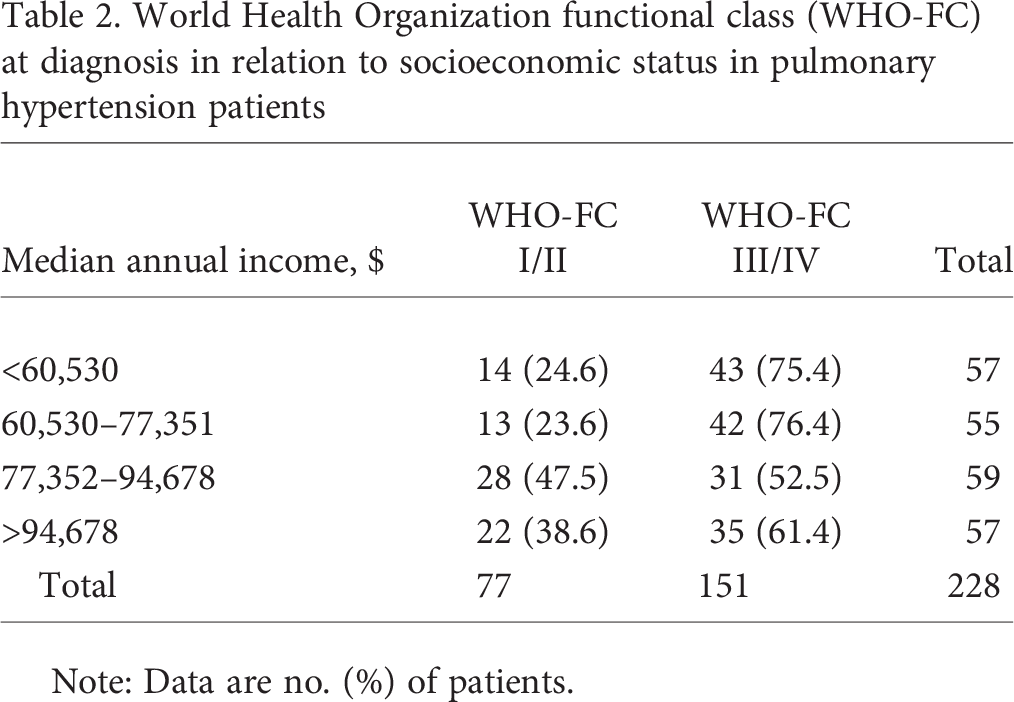
Note: Data are no. (%) of patients.
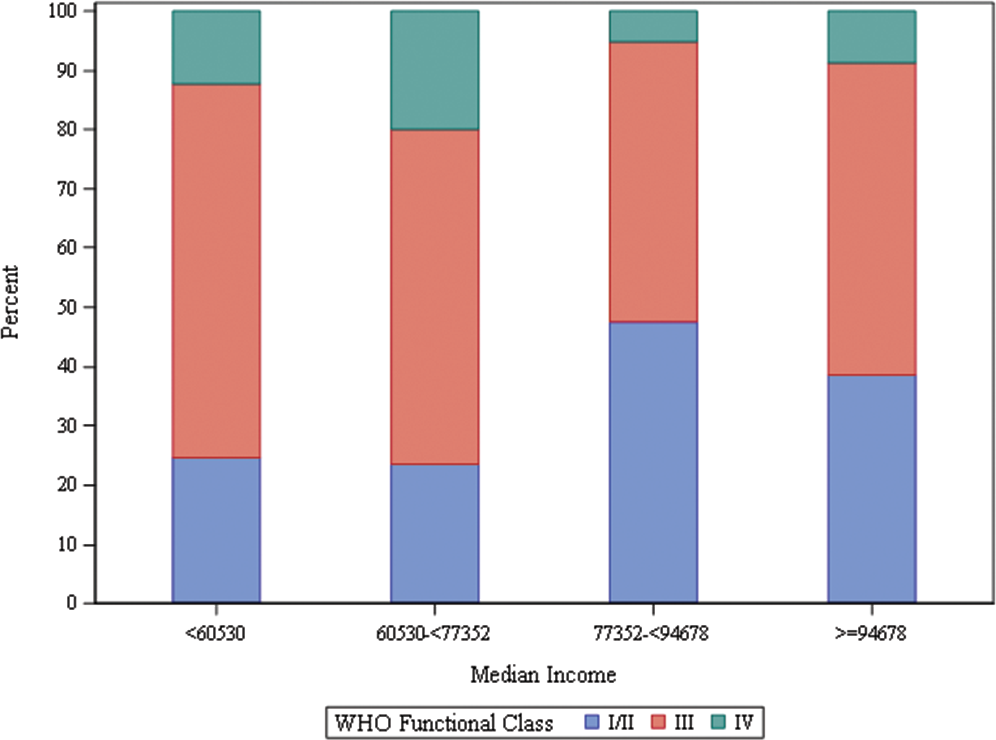
World Health Organization (WHO) functional class at diagnosis in relation to socioeconomic status in pulmonary hypertension patients.
Of the 228 PHTN patients, 116 had a PCWP of <15 mmHg and so were considered to have PAH, as per WHO criteria. 11 Of these PAH (WHO group 1) patients, 32 (27.6%) were male and 84 (72.4%) were female. At initial presentation, their mean age was 60 years (standard deviation: 15 years). Median annual income was $75,020 (Table 1). The same income quartiles as for the 228 PHTN patients were used.
Thirty-three (28.4%) of the PAH patients were in the lowest quartile, followed by 28 (24.1%) in the second-lowest, 24 (20.7%) in the third, and 31 (26.7%) in the highest income quartile. For the lowest-quartile income group, 5 (15.2%) were in WHO-FC I/II at initial presentation and 28 (84.8%) in WHO-FC III/IV. For the second income quartile, 8 (28.6%) were in WHO-FC I/II at initial presentation and 20 (71.4%) in WHO-FC III/IV. For the third income quartile, 11 (45.8%) were in WHO-FC I/II at initial presentation and 13 (54.2%) in WHO-FC III/IV. For the highest-income quartile, 14 (45.2%) were in WHO-FC I/II at initial presentation and 17 (54.8%) in WHO-FC III/IV. Data are presented in Table 3 and Figure 2. The difference in WHO-FC by income quartiles was statistically significant (χ2 test: P < 0.0307). There was a negative relationship between WHO-FC and income (Spearman r = −0.30968, P < 0.0007)]. As was true for patients with PHTN, WHO FC at the time of initial diagnosis was a strong predictor of long-term survival in patients with PAH. Analysis of the Kaplan-Meier curve revealed that survival was significantly better for patients in FC I or II than for those in FC III and better in FC III than in FC IV, as previously described in the literature.7,14
World Health Organization functional class (WHO-FC) at diagnosis in relation to socioeconomic status in pulmonary arterial hypertension patients
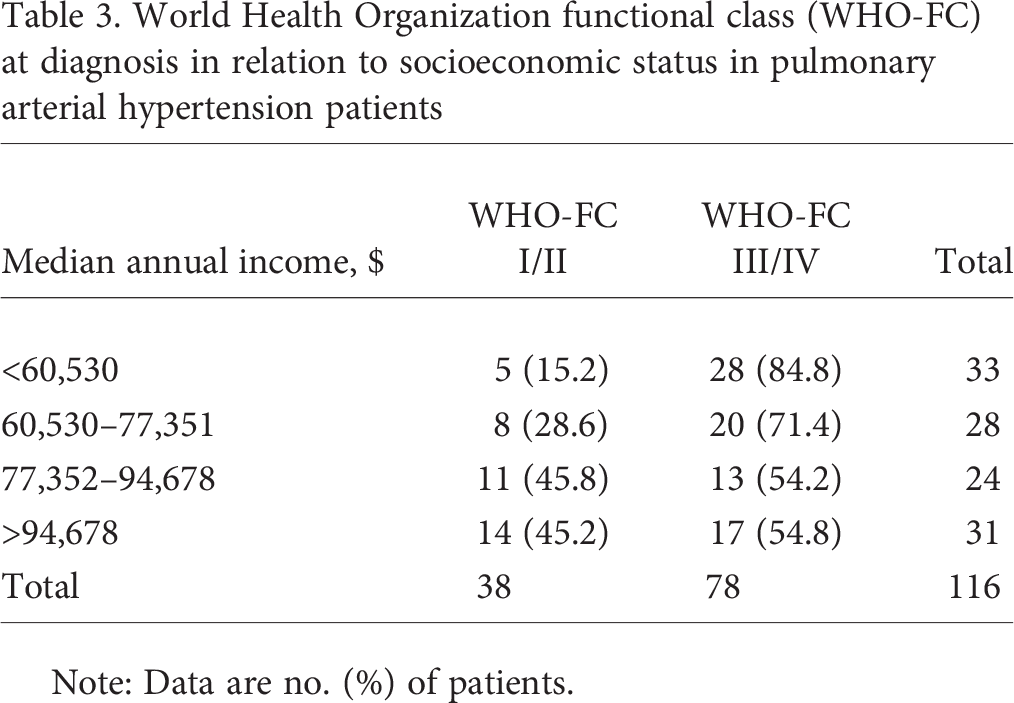
Note: Data are no. (%) of patients.
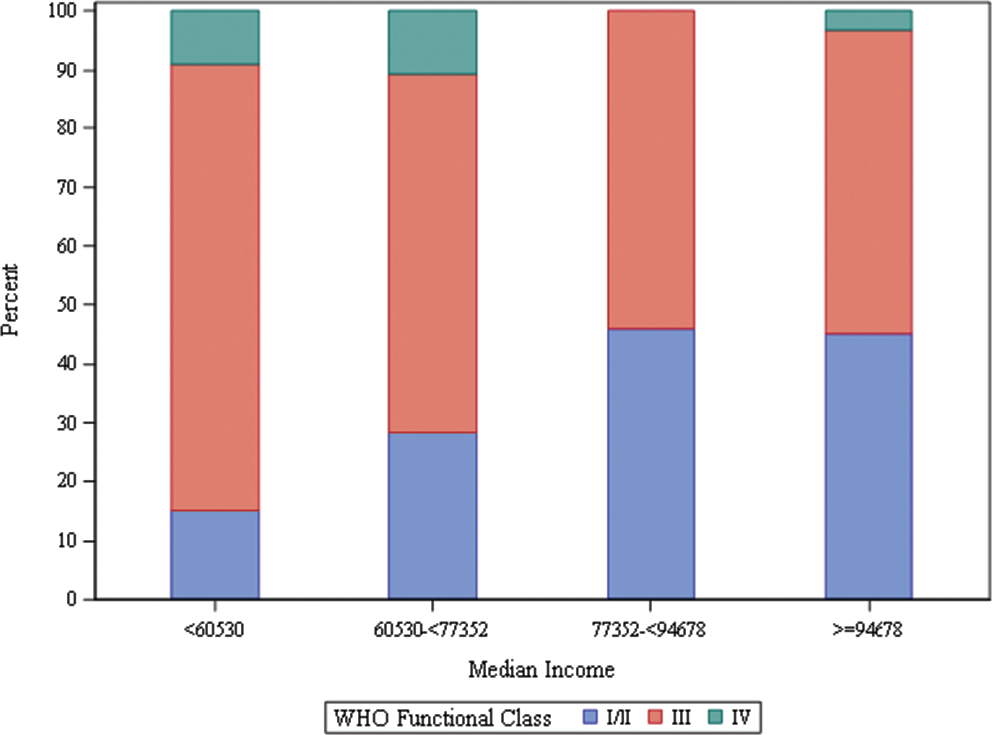
World Health Organization (WHO) functional class at diagnosis in relation to socioeconomic status in pulmonary arterial hypertension patients.
DISCUSSION
Although many factors contribute to SES, the zip code as a surrogate of SES has been well validated by the Agency for Healthcare Research and Quality. The purpose of this study was to report the PHTN disease severity at time of first presentation based on a patient's zip code–based median household income. Because of our center's proximity to the border between Queens and Nassau Counties, New York, we studied an economically (Queens County median annual income: $57,001; Nassau County median annual income: $97,960; US Census Bureau, State and County QuickFacts; http://www.census.gov/quickfacts) and ethnically diverse population. In this retrospective cohort study, we found that a lower SES is associated with more clinically advanced pulmonary hypertensive disease at first presentation, based on WHO-FC. Furthermore, poor WHO-FC was associated with mortality considerably greater than that for patients who presented with less functional impairment. SES plays a vital role in access to health care, and our results indicate a significant delay in diagnosis in patients with low SES, as evidenced by more severe symptoms of functional limitation at the time of initial diagnosis.
Access to health care and SES
Our findings focus attention on the more advanced disease stage at time of presentation, based on SES. Patients with PHTN, which commonly presents with dyspnea on exertion, often present first to primary-care physicians. However, access to primary healthcare providers, even in a universal healthcare system, favors the perceived wealthy, as exhibited by Olah et al. 15 In that study, the proportion of calls resulting in an appointment being offered was significantly higher when the callers presented themselves as having high SES than when they presented themselves as having low SES and when the callers stated the presence of chronic health conditions than when they did not. 15 PHTN is a disease that is most often diagnosed by a pulmonary or cardiovascular specialist. It has been observed in many developed countries that, despite the type of healthcare system, nationalized or privatized, patients with high SES are much more likely to receive a medical specialist consultation than patients with low SES. 16 Disease severity and stage of disease at first presentation are heavily linked in many types of cancers, 17 cardiovascular disease, 18 and even other pulmonary conditions.4,5
PAH and SES
PAH (WHO group 1 PHTN) is a disease of the small pulmonary arteries that leads to a progressive rise in pulmonary artery pressure and pulmonary vascular resistance, resulting in right heart failure. 19 There now exist many pharmaceutical options for the treatment of PAH 6 that may also be used in early stages of the disease. 20 For this reason, an early referral is imperative, as studies have shown that prognosis is better for patients who present in FC I or II than for those who present in FC III or IV.21,22 In fact, 5-year mortality rates in FC III and IV are more than double those of patients in FC I or II. 6 The results of our study support these earlier findings, as patients with PHTN or PAH had considerably better survival if they were in FC I or II at time of initial presentation than if they were in FC III or IV. The associated conditions linked to PAH are many and include connective-tissue disease, such as systemic sclerosis. 11 In the GENISOS study by McNearney et al., 23 which studied scleroderma patients, it was seen that African American and Hispanic ethnic groups had a lower SES and a statistically significantly greater incidence of physical exam findings suggestive of PHTN (P2 being louder than A2 on heart auscultation), compared to white patients.
Effects of SES on timing referral
Our study shows that patients with a lower SES, based on median household income, presented in a more severe disease state. The reason for this phenomenon is uncertain, but it is likely due to decreased access to primary and subspecialty health care. It is well known that late referral is detrimental to outcomes in many disease states. For example, increased mortality has been well documented in end-stage renal disease. 24 Referral of patients to centers adept at handling PHTN is essential for early diagnosis and initiation of therapy; however, a lower SES may exclude patients from obtaining this subspecialized care. With the number of pulmonary hypertension centers increasing more than 5-fold in the past 20 years, there is no paucity of available referral centers, 25 yet it seems as though patients with a lower SES are being referred later in their disease process. In support of this trend, a qualitative study by Bernheim et al. 26 found that for patients with a lower SES, physicians, to make health care more affordable, would use less expensive medications, avoid specialist referral, accomplish more in a single visit, and postpone testing.
The etiologies of PHTN are many, and, as in all cases, an early diagnosis is imperative for improved outcomes. However, across all groups of PHTN a lower SES plays a detrimental role. In the case of sarcoidosis (WHO group 5 PHTN), a lower SES was significantly associated with more extensive lung involvement, and patients with incomes less than $20,000 were 3.5 times as likely to present with stage 3–4 disease. 27
Conclusion
Our study suggests that patients with low SES have more advanced PHTN and PAH at time of diagnosis than patients with higher SES. A lower SES has been associated with worse outcomes in PAH, and the findings from our study suggest that this may be due to more advanced disease at the time of initial diagnosis. Our data appear to be consistent with those for other chronic pulmonary conditions in terms of later stage of disease at initial presentation, based on SES. However, PHTN and PAH differ from conditions such as COPD and asthma because of the greater effect of delay in diagnosis on final clinical outcome. Further larger studies should be conducted to confirm our findings that SES affects disease severity at initial diagnosis and to determine the primary impediments preventing patients with low SES from receiving earlier diagnoses.