
Abstract
Australian and New Zealand Journal of Psychiatry 2006; 40:1031–1038
There is converging evidence that sufferers of obsessive–compulsive disorder (OCD) may manifest neurobiological deficits, with evidence from neuroanatomical, neurosurgical, neuropharmacological and neurophysiological domains (for reviews see [1–3]). Despite this, however, the aetiological determinants of OCD remain unclear.
Neuropsychological investigations have attempted to integrate the behavioural expressions of OCD with possible functional brain abnormalities and have yielded some reliable findings (for reviews see [4,5]). The most consistent finding in the literature is a deficit in inhibition. In addition, impaired set shifting ability is commonly reported, but planning ability appears unaffected. Inconsistent findings have been observed for working memory and verbal fluency. Several limitations with previous research may have contributed to the discordant results. These include the absence of an appropriate taxonomy of executive functions (stemming partly from the practice of using the terms ‘executive’ and ‘frontal lobe’ interchangeably), the paucity of ‘pure’ tests that measure cognitive functions, and the limited use of appropriate clinical control groups.
Moreover, whether these deficits in executive function are a trait- or state-related phenomenon has not been systematically examined. Consequently, it is unclear whether executive function deficits in OCD are stable characteristics that are consistently deviant from normal even during remission, or whether they are state-dependent, reflecting possible effects of acute psychopathology on cognitive processes. Notably few studies have examined the relationship between symptom remittance and neuropsychological functioning in adults with OCD [6–8], and no study has formally tested whether executive function deficits are trait or state markers in the disorder.
Discriminating between deficits that play an aetiologically significant role in OCD and those that may be the result of symptomatology has far reaching theoretical and clinical implications. For example, trait-like deficits may help identify individuals predisposed or vulnerable to develop OCD. This in turn would allow for prevention programs to be trialled. Identification of state-dependent deficits may help monitor the course of OCD, including fluctuations in response to treatment and the assessment of the overall response to treatment. This would not only aid clinical decisions but also shed light on the underlying pathophysiology of the symptomatic episode.
In studies designed to assess the effects of treatment, Kahn et al. [7] and Thienemann and Koran [6] reported improvement in patients, post treatment, in some domains of cognitive function (verbal fluency and inhibition). However, interpretation of these findings is limited because of methodological limitations including small sample size (n = 6 in Kahn et al.'s study [7]), no description of statistical analyses, limited information regarding the nature or degree of impairment, and possible practice effects. In another treatment outcome study, Bolton et al. also reported improvement in performance on some neuropsychological measures [8]; however, these changes were not correlated with changes in the Yale-Brown Obsessive Compulsive Scale (Y-BOCS) scores (consistent with [6]), which may be expected if it were assumed that the impairments were state-related. These findings suggest that factors other than the reduction in symptom severity are linked to an improvement in executive functions.
In a more recent study, Kim et al. investigated changes in neuropsychological functions over a 4-month period in patients with OCD, following pharmacological treatment [9]. At pretreatment, OCD subjects were reported to exhibit specific cognitive impairments, which were demonstrated to persist despite improvement in obsessive’ compulsive symptoms. These results are consistent with the interpretation that the deficits are stable trait-like features of OCD.
To help delineate possible state-trait factors, it is also critical to study executive functions during childhood and adolescence, before illness and treatment effects potentially confound the findings. However, investigations of cognitive function in children with OCD are limited [10–12]. A recent study reported that adolescents diagnosed with OCD failed to demonstrate any cognitive impairment [12]. In contrast, however, Behar et al. reported differences on measures of visuospatial functioning and problem solving between OCD adolescents and controls [10], and Rosenberg et al. reported deficits on oculomotor tests of response inhibition in non-depressed, psychotropic- naive children and adolescents [11]. These studies may be interpreted as indicating that neuropsychological impairments are trait-related; however, as indicated previously, they should be considered preliminary.
Examining deficit profiles in a longitudinal design has significant advantages especially in psychiatric conditions where variability between clinical characteristics, such as family, developmental and clinical histories (i.e. symptom onset, course, prognosis and treatment) renders it difficult to match individuals between groups even if a clinical control group was studied in a cross-sectional design. In relation to OCD, the assessment of cognitive functioning over the developmental course of the disorder also provides a method of assessing the progressive nature of these deficits. The authors are unaware of a study that has examined executive functions in a comprehensive way using a longitudinal design.
Therefore, although executive function deficits are commonly reported in people with Symptomatic OCD, it is currently unclear whether these deficits are state- or trait-related or whether they are specific to OCD, as compared with other anxiety disorders. The present study addressed these issues by examining executive function deficits comprehensively in Symptomatic and Remitted OCD groups compared with a Panic Disorder (PD) control group. Additionally, a subgroup of people with Symptomatic OCD was followed up to determine whether existing deficits persist after symptom reduction.
Method
Subjects
Study 1
Sixty subjects who had primary clinical diagnoses of Symptomatic OCD (n = 20), Remitted OCD (n = 20) and PD (n = 20) were recruited from Nepean Anxiety Disorders Clinic (Sydney, Australia). Clinical diagnoses were based on DSM-IV [13] criteria and were concordant with diagnoses based on the computerized version of the Composite International Diagnostic Interview [14]. Subjects also needed a score of 20 or greater (moderate-severe symptoms) on the Y-BOCS [15], to be recruited into the Symptomatic OCD group. The treating Clinical Psychologist or Psychiatrist conducted the diagnostic assessments.
Remitted OCD patients were those who previously qualified for a diagnosis of OCD, but obtained a current total score less than 10 (no symptoms) on the Y-BOCS. They were also defined as ‘much improved’ or ‘very much improved’ on item 18 of the Y-BOCS (responders to treatment) by their treating Clinical Psychologist or Psychiatrist. Remitted subjects were invited to participate in the study when attending follow-up appointments.
Exclusion criteria for all subjects were current or past history of neurological disorder (including Parkinson's Disease, Huntington's Disease or epilepsy), head injury with a loss of consciousness, psychotic, bipolar or substance abuse disorders, mental retardation, or colour blindness. No subject had comorbid OCD and PD diagnoses. Forty-three subjects were medicated at the time of testing (selective serotonin re-uptake inhibitors ([PD: 10; Sym OCD: 10; Rem OCD: 8], tricyclics [Sym OCD: 3; Rem OCD: 1], Type A reversible monoamine oxidase inhibitors [PD: 4; Sym OCD: 1; Rem OCD: 1] and benzodiazepines [PD: 2; Sym OCD: 1; Rem OCD: 2]).
Study 2
The 20 subjects recruited into the Symptomatic OCD group in Study 1 were followed up, and those that met remitted status were retested (n = 10). The mean time between testing was 1.40 years (SD = 0.52). Inclusion criteria for remitted status was: (i) DSM-IV diagnostic criteria for OCD was no longer met; (ii) a total score less than 10 (no symptoms) on the Y-BOCS was obtained; and (iii) they were defined as ‘much improved’ or ‘very much improved’ on item 18 of the YBOCS by their treating clinician. Of the 10 subjects, two were treated with medication only, one received cognitive behavioural therapy only and seven received a combination of medication and cognitive behavioural therapy treatments. Seven of 10 subjects remained on medication when tested during remission.
Measures and procedures
Study 1
A trained Clinical Psychologist (SB) assessed executive functions by a series of six tests: the computerized version of the Wisconsin Card Sorting Test (WCST [16], to measure set shifting), the Go/Nogo Task ([17], to measure inhibition), a vocal reaction time computer version of the Stroop Task ([18], also to measure inhibition), the Tower of London Test ([19], to measure planning ability), Controlled Oral Word Association (‘FAS’ version [20], to measure verbal fluency) and an Auditory/Tracking Dual Task ([21], to measure working memory). The National Adult Reading Test [22] was administered to estimate premorbid verbal IQ (NART-VIQ).
To assess severity of depressive and obsessive and compulsive symptomology, the Beck Depression Inventory – II (BDI-II [23]) and the Y-BOCS were administered. To examine whether the testing situation provoked comparable anxiety levels in each group, the state form of the State-Trait Anxiety Inventory (STAI-S [24]) was administered.
All neuropsychological tests were administered within a 90-minute, single session. Rest periods were employed and test order was counterbalanced to control for fatigue effects. The study was approved by Wentworth Area Health Service and University of Wollongong ethics' committees.
Study 2
All tests administered while subjects were symptomatic were readministered during the remitted stage.
Statistical analyses
Study 1
Demographic and clinical measures were subjected to manovas for (i) demographics (age of onset, age, sex, years of education) and (ii) clinical characteristics (Y-BOCS total score, BDI-II, STAI-S, NARTVIQ). With regard to between-group comparisons, two planned contrasts were performed: the combined Symptomatic and Remitted OCD groups versus the PD group, in order to determine whether a characteristic was specific to OCD; and the Remitted OCD versus Symptomatic OCD subjects to determine whether the characteristic was related to symptomatic status within OCD.
Separate manovas with the same between-group planned contrasts were conducted on each of the executive function domains of inhibition, set shifting, working memory and planning. This involved four tests with the dependent variables: (i) inhibition (Go/Nogo indices [percentage of omission and commission errors] and Stroop indices [number of errors and response time for baseline conditions 1 and 2 and the interference condition]); (ii) set shifting (perseverative errors and categories achieved); (iii) working memory (tone response time for the task completed independently and concurrently with tracking aspect of task, number of omission errors for the tone conducted concurrently, and the average time in error for the tracking task completed independently and concurrently); and (iv) planning (Tower of London indices [total number of moves in excess of the minimum]).
An anova tested for group differences on the executive function domain of verbal fluency (total number of words generated). To control for Type I error, a Bonferroni adjustment was employed such that within each manova alpha was divided by the number of dependent variables [25]. All statistical values reported are for twotailed tests.
When deficits were observed for the OCD group, the relationship between the executive function deficits and symptom severity was further analysed by Pearson's Product-Moment correlation coefficients ‘r’.
For deficits identified in OCD, the influence of medication was examined by conducting t-tests between medicated (n = 27) and nonmedicated (n = 13) OCD subjects.
Study 2
Repeated measures t-tests were conducted to examine the differences between Symptomatic and Remitted OCD status for clinical characteristics and for executive function measures.
Results
Study 1
Demographic and clinical characteristics
The combined OCD group had an earlier age of onset, t(58) = 5.93, p < 0.001 than the PD controls. No other differences were found on depression, state-trait anxiety, IQ, or demographic variables (age, sex, years of education) between the PD and the combined OCD group. As expected, the Symptomatic OCD subjects exhibited more obsessive-compulsive symptoms than Remitted OCD subjects on the Y-BOCS, t(38) = 19.85, p < 0.001. No differences were found between the Remitted and Symptomatic OCD groups on clinical (depression, statetrait anxiety and IQ) or demographic (age, sex, years of education, age of onset) variables (see Table 1).
Demographic and clinical characteristics for Symptomatic OCD, Remitted OCD and Panic Disorder subjects for Study 1 and Study 2
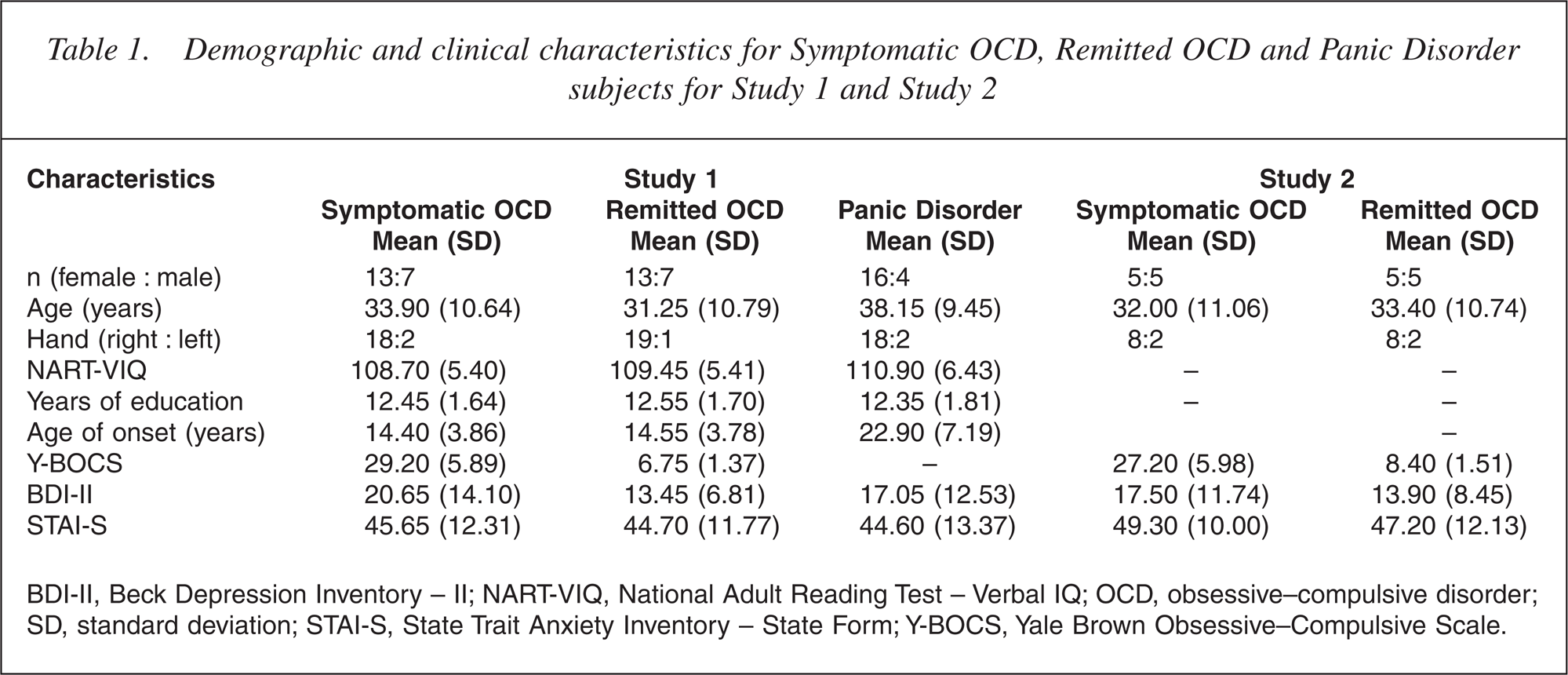
BDI-II, Beck Depression Inventory – II; NART-VIQ, National Adult Reading Test – Verbal IQ; OCD, obsessive–compulsive disorder; SD, standard deviation; STAI-S, State Trait Anxiety Inventory – State Form; Y-BOCS, Yale Brown Obsessive–Compulsive Scale.
Executive functions
Means and standard deviations for each executive function task arepresented in Table 2.
Performance on executive function tasks for Symptomatic OCD, Remitted OCD and Panic Disorder subjects for Study 1 and Study 2
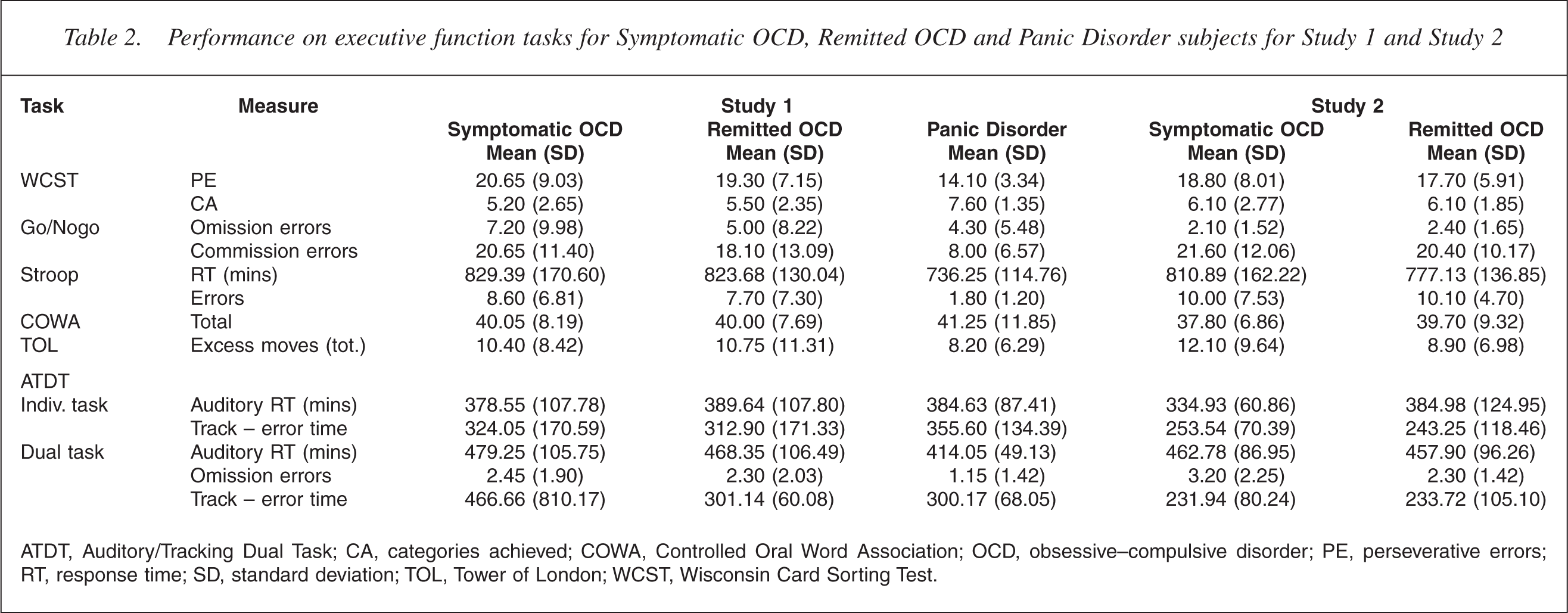
ATDT, Auditory/Tracking Dual Task; CA, categories achieved; COWA, Controlled Oral Word Association; OCD, obsessive–compulsive disorder; PE, perseverative errors; RT, response time; SD, standard deviation; TOL, Tower of London; WCST, Wisconsin Card Sorting Test.
Set shifting (WCST). The combined OCD group made more perseverative errors, t(58) = 3.10, p = 0.003 and achieved fewer categories, t(58) = 3.77, p < 0.001 than the PD group. There were no differences between the Symptomatic and Remitted OCD groups on these indices.
Inhibition (Go/Nogo Task, Stroop Task). There were no differences between the PD group and the combined OCD group on the percentage of omission errors made on the Go stimuli. For the Nogo stimuli, the combined OCD group had a higher percentage of commission errors than the PD group, t(58) = 3.97, p < 0.001. Hence, OCD patients exhibited a deficit in the inhibitory portion of the Go/Nogo task. The Symptomatic and Remitted OCD subjects did not differ on the percentage of omission errors or commission errors made.
For the baseline conditions of the Stroop Task (Blocks 1 and 2), there were no differences between the PD subjects and the combined OCD group for the number of errors made. However, the combined OCD subjects made more errors than the PD controls on the interference trial of the vocal Stroop Task, t(58) = 3.99, p < 0.001. The Symptomatic and Remitted OCD groups did not differ on the number of errors made on the baseline conditions, or on the interference trial.
No differences were found between the PD group and the combined OCD group for reaction time for the baseline conditions (Blocks 1 and 2) and the interference condition of the Stroop Task, after adjusting for alpha. The Symptomatic and Remitted OCD groups also did not differ on reaction time for the baseline conditions, or on the interference trial.
The combined OCD group's scores on the Y-BOCS did not correlate significantly with any of the set-shifting or inhibition measures.
Planning (tower of London test) and verbal fluency. Neither of the between-group comparisons was significant for planning and verbal fluency measures.
Working memory (auditory/tracking dual task). Performance on the tracking task (average time in error) was transformed to reduce skewness (natural log). When performing the tone and tracking tasks independently, the OCD groups performed as well as the PD group. Performance was also comparable when performing these tasks concurrently. There were no differences between the Symptomatic and Remitted OCD groups on the tone task or the tracking task when performed concurrently.
Effect of medication
No differences were found between the medicated and nonmedicated OCD subjects on any of the significant executive function measures or on depression or test-induced anxiety.
Study 2
Demographic and clinical characteristics
Group data for subject's demographic and clinical characteristics are presented in Table 1. It was found that when symptomatic, OCD subjects displayed more obsessive–compulsive symptoms (on the YBOCS) than when they were remitted, t(9) = 11.52, p < 0.01. As measured by the BDI-II, despite a decrease in the severity of depression once OCD subjects remitted, this change did not reach significance. As measured by the STAI-S, test-induced anxiety did not differ as a function of Symptomatic OCD status.
Executive functions
Table 2 presents subjects' group data for performance on each executive function task. The results are clear and consistent in that little change occurred for the OCD group, with deficits observed in the symptomatic stage and persisted during the remitted phase. This pattern of results applied to each of the executive functions studied.
For the subgroup of OCD subjects studied longitudinally, symptom reduction was not accompanied by improvements in executive function. This was consistent for performances across all tasks.
Discussion
The aims of this research were to confirm the presence of executive function deficits and, if they occurred in OCD, to determine whether they were state- or traitrelated. Study 1 found that compared with an anxiety control group, subjects with OCD exhibited specific deficits in executive functions of set shifting and inhibition, but performance in the domains of planning, working memory and verbal fluency was found to be comparable. At follow-up (Study 2), performance on these measures remained unchanged. Results suggest that firstly, not all executive functions are impaired in OCD individuals, and secondly, over the course of the disorder executive function deficits and non-deficits remain stable and do not deteriorate with the duration of the illness or improve with symptom remittance. The findings may be interpreted as evidence that some executive function deficits are trait rather than state markers in OCD. To our knowledge, this is the first study to demonstrate that executive function deficits within OCD are trait-like.
Examination of executive function deficits over a longitudinal course is relevant given the chronic nature of OCD. Although the current research partially fulfils this goal, the research has not examined whether a similar pattern of inhibition and set shifting deficits exist before onset of the illness (premorbid trait markers). If it was determined that the specific executive function deficits predate illness onset, the benefits include the possibility of reliably identifying at-risk individuals. Furthermore, this would allow for the development of prevention programs that address the specific impaired executive functions (i.e. inhibition) and the examination of the efficacy of these strategies in arresting the development of obses-sive–compulsive symptoms. Thus, identifying trait markers would also have implications for choice of treatment strategies with individuals diagnosed with OCD.
Study 1 did not find any evidence that the medications typically used to control the symptoms of OCD had an affect on executive functions. This suggests that our findings were not confounded by medication, and is consistent with previous literature [26]. Statistical analyses for the possible effects of medication between the subgroups in Study 2 were not conducted because of the small sample sizes of medicated versus non-medicated individuals. However, as medication status remained stable for OCD subjects from symptomatic to remitted stages of the illness, it is unlikely that this factor was responsible for the findings.
The pattern of persistent neuropsychological deficits despite symptom control is consistent with the notion that a neurobiological deficit underlies OCD symptomatology. Furthermore, the current research appears to suggest that such a core set of deficits remain untouched by treatments that nevertheless control symptoms. The persistence of these underlying deficits may be responsible for, or be associated with, mechanisms underpinning further relapses. Future research should determine whether such a pattern of persistent deficits occurs equally for groups of patients treated with cognitive behavioral therapy (CBT), medication, and CBT plus medication. Finally, although the weak statistical power associated with small numbers in Study 2 weakens the reliability of the results, this should be viewed in the context that performance on executive functions (based on mean values) barely improved and, in several instances, grew marginally worse. Such a pattern of results is more stable and less sensitive to reversal even with additional numbers. It is acknowledged, however, that the conclusions could be generalized to the population with more certainty, had larger numbers been employed. Thus, future research would benefit from studies replicating these findings with larger sample sizes.
Consistent with Thienemann and Koran [6] and Bolton et al. [8], no relationship was evident in this study between symptomatology (Y-BOCS) and impaired inhibition and set shifting for the combined Symptomatic and Remitted OCD group. These findings are also consistent with a trait hypothesis, where it would be expected that executive functions are independent of symptoms.
As a ‘non-clinical’ control group (i.e. normal controls) was not included, it is possible to argue that the relatively poor performance on the executive function measures was not due to performance decrements of the OCD groups, but performance enhancements of the PD group, thus, arguing that OCD subject's performance is not in fact ‘deficient’. The findings of the limited research on executive functioning in PD subjects indicates unimpaired functioning [26–28], with PD subjects performing comparably with normal control subjects. Hence, given the lack of evidence for performance enhancements in PD subjects, it may be argued that the results represent decrements in the OCD group. Moreover, on the neuropsychological measures where normative data were provided (i.e. Controlled Oral Word Association), performance of the PD and normative data were compared and it was revealed that PD subjects performed in the normal range. This further contributes to the unlikeliness that the findings were attributed to performance enhancements in the PD group. However, future research using a ‘non-clinical’ control group would enhance the experimental design of studies, and help clarify the issue of performance decrements on executive function measures in OCD subjects. A further caveat of the results is that the PD group had a significantly later age of onset; therefore, it cannot be ruled out that the OCD group was more impaired as a result of a longer duration of illness, rather than a result of the type of illness.
In conclusion, this research assessed the stability of executive function deficits in OCD across the course of the disorder, while subjects were both symptomatic and subsequently remitted. This research found that impairments in inhibition and set shifting are stable characteristics found to be consistently deviant from normal levels even during symptoms remission. These findings have significant theoretical and clinical implications.