
Abstract
The overlap between anxiety and depressive disorders has been recognized since antiquity [1], leading to several theories attempting to explain the complicated relationship (e.g. [2, 3]). It has been argued previously that the relationship between anxiety and depression can be best understood when each is considered to have its own unique set of relatively specific symptoms, in addition to a core set of symptoms shared by both disorder groups [4, 5]. High correlations between many previous measures of anxiety and depression (e.g. [6–9]) can be understood as resulting from the over-inclusion of these nonspecific symptoms as items in previous questionnaires.
In the tripartite model, symptoms such as anhedonia and social withdrawal are considered to be markers of low positive affectivity, and are thought to be relatively specific to depressive disorders. In contrast, symptoms such as tachycardia, hot and cold flushes, and difficulty breathing are thought to be anxiety-specific symptoms of anxious arousal. Other symptoms such as insomnia, dysphoria, reduced appetite and indecisiveness are thought to represent a non-specific negative affectivity (NA) dimension shared between anxiety and depression [5]. While some authors have refined the complexities of the Anxious Arousal dimension (e.g. the integratedhierarchical model of Mineka et al. [4]), a basic structure of specific and non-specific symptoms has a strong body of support.
Further to proposing their tripartite model, Watson et al. went on to develop a pen-and-paper questionnaire, the Mood and Anxiety Symptom Questionnaire (MASQ [10, 11]), as a measure of various symptoms of anxiety and depression. The instrument was validated in large samples of student, community and clinical (substance problem) participants using exploratory factor analytic procedures [10, 11]. From these validation studies, Watson et al. drew support not only for the MASQ itself, but for their hypothesized underlying tripartite structure of anxiety and depressive symptoms. Although the threefactor structure was supported in all three samples, the clinical sample consisted of patients treated for substance problems rather than anxiety or mood disorders. In addition, the use of exploratory factor analysis did not allow measures of overall fit, or factorial invariance across the three samples, to be calculated.
Two studies have used item-level exploratory factor analyses to assess the factor structure of the MASQ. Keogh and Reidy used a sample of undergraduate students and interpreted their data as supporting the tripartite structure of the MASQ [12]. They did, however, raise concerns in a number of areas. First, they reported that clear discrepancies existed between analyses done at the item- and subscale-level unit of analysis. Second, they reported that it remained unclear as to the breadth of the Anxious Arousal factor, specifically whether it ought to incorporate somatic symptoms in addition to anxiety symptoms. Third, the investigators reported that a number of items of the MASQ were unstable in the solution, not loading exclusively on single factors. On the basis of these concerns, Keogh and Reidy recommended a strict set of criteria for future analyses, and the removal of items that are deemed to be impure markers of the underlying latent factors.
Similar results were reported in the earlier brief paper by Bedford [13]. In this study, Bedford reported that 29 items on the MASQ displayed complex or weak loadings on a tripartite factor structure. Keogh and Reidy similarly reported that many items from the MASQ did not load stably onto a three-factor structure [12]. Despite the MASQ authors reporting that the 90 MASQ items did load adequately onto a tripartite structure [11], it is clear in this original study that many items also display complex or weak loadings on a three-factor model. Bedford has recommended the removal of unstable or complex items to leave a more robust subset of symptoms [13]. These findings highlight a major weakness in the MASQ literature published to date, in that previous authors have concluded support for the MASQ tripartite structure based on examination of individual item loadings, rather than an overall objective statistic of goodness-of-fit. The use of confirmatory factor analytic methods is emphasized as a significant advance of the current research.
There exists one published study that is more stridently critical of the tripartite structure of the MASQ; however, the analyses used in this work are flawed in a critical way. Burns and Eidelson used the clinical data from the original MASQ validation studies (a sample of patients with substance use disorders) to conduct a confirmatory factor analysis [14]. Critically, they used only four of the five MASQ subscales, rather than the complete instrument. In this investigation, Burns and Eidelson also used subscale totals, rather than individual items as their unit of analysis, which makes comparison with other studies using item-level analysis difficult. The MASQ General Distress Mixed (MASQ-GDM) scale was excluded from the analysis for reasons not fully explained. Burns and Eidelson attempted to fit these four MASQ subscales to both a ‘tripartite’ model and a two-factor anxiety-vs-depression model. On the basis of their analysis, the researchers concluded that a two-factor model was a better fit to the data than the tripartite model. The conclusions drawn in this paper are weakened by the exclusion of the MASQ-GDM subscale. To exclude the subscale containing the items which are most representative of the non-specific factor is almost certain to reduce the coherence of this factor, significantly altering the final relationship between subscales and their latent factors. As such, this study cannot be integrated into the larger consensus within the MASQ literature.
Concerns about the factor structure notwithstanding the discriminant validity of the MASQ has been evaluated and found to be weak. Importantly, this poor validity has been demonstrated in a sample of anxious/depressed individuals. Recently, Boschen and Oei investigated the specificity of the MASQ subscales to anxiety and depression diagnosis, as well as the ability of the MASQ to differentiate anxious and depressive illness [15]. The ability of the MASQ to differentiate between anxiety and depression diagnoses was demonstrated to be poor. The researchers demonstrated that although a statistically significant discriminant function can be derived from the MASQ subscales, this is capable of accurately diagnosing less than 70% – clearly insufficient for clinical or research use in this capacity.
From the above review, it can be seen that the current body of literature around the MASQ is deficient in several key areas. First, there is outstanding debate over the structure of the instrument, and particularly whether all MASQ items comprise stable, robust, differentiable factors. Second, there remains no confirmatory factor analysis of the MASQ items, where individual items are used as manifest measures of the latent tripartite factors.
Third, despite being derived from a theory designed to enhance discrimination between anxiety and depression, the MASQ has yet to be assessed in a sample comprised of patients with predominantly mood and/or anxiety symptoms. The assessment of the MASQ factor structure in a clinical sample of patients with anxiety and depressive symptoms is particularly important for several reasons. The tripartite model which underlies the theoretical structure of the MASQ was derived primarily for the purpose of explaining strong correlations between anxiety and depression measures. Furthermore, testing in an anxious/depressed sample provides a test of the MASQ structure under demanding conditions: in a sample where symptoms are expected to show strong correlation. Evaluation of the MASQ's structure in this sample also provides some assessment of the likely clinical utility within this population.
Objectives of the study
The present study aims to address these three areas of weakness in the MASQ research. It attempts to clarify confusion regarding the factor structure of the complete MASQ item set through the use of confirmatory factor analysis, doing so using a clinical sample of anxious/ depressed patients. Furthermore, it aims to assess this factor structure using MASQ items and MASQ subscales as the units of analysis in different models.
Analyses in this study aimed to examine the factor structure of the MASQ in an anxious/depressed sample, using scale-level and item-level confirmatory factor analytic procedures. First, it was hypothesized that a similar pattern of correlations between MASQ subscales to previous studies would emerge (i.e. where depressionspecific and anxiety-specific scales show weaker correlations with each other than the general distress scales). Second, it was predicted that confirmatory factor analysis would show that a tripartite model fit the MASQ data more parsimoniously than alternative two- or five-factor models.
Method
Participants
The participant group was comprised of 470 individuals: 280 female and 189 male participants, with one of unspecified sex. The participants were aged from 17 to 70 years, with a mean age of 34.30 years (SD = 10.73 years). Participant data were drawn from a pool of 496 consecutive presentations for treatment at a University Psychology Clinic. After individuals with missing MASQ data were excluded, the final sample of n = 470 was obtained.
Using a clinical interview, participants were diagnosed according to DSM-IV diagnostic criteria by a postgraduate clinical psychology intern [16], in consultation with, and under supervision of, an experienced consultant clinical psychologist. Diagnosis was checked through the clinic procedure of having diagnostic reports read by a separate independent consultant clinical psychologist. Ninety-eight did not meet specific diagnostic criteria for neither a mood nor anxiety disorder, despite reporting significant symptoms. Anxiety disorder alone was diagnosed in 178 patients, while a depressive disorder alone was diagnosed for 102 patients. A total of 92 subjects met criteria for comorbid anxiety and depressive disorders at the time of intake.
Materials
Mood and Anxiety Symptom Questionnaire [10, 11]
The MASQ is a 90-item questionnaire designed to assess the validity of the tripartite model of anxiety and depression, requiring that subjects respond, on a Likert-type scale from 1 (‘Not at All’) to 5 (‘Extremely’), as to the presence and severity of a series of symptoms of anxiety and depression. Items were derived by the scale's authors from the symptoms listed in the diagnostic criteria of several anxiety and mood disorders. As originally constructed, the MASQ consists of five subscales. Two of these are thought to be comprised of symptoms which are specific to either anxiety or depression. The MASQ Anxious Arousal (MASQ-AA) and MASQ Anhedonic Depression (MASQ-AD) subscales are proposed as being specific to anxiety and depression, respectively. Three non-specific (‘general distress’) subscales can also be calculated. The MASQ General Distress Anxiety (MASQ-GDA), MASQ-GDM, and General Distress Depression (MASQ-GDD) are comprised of symptoms thought to show less specificity to either anxiety or depression, commonly occurring in either condition.
The original authors reported that the MASQ subscales all show adequate reliability (α ≥ 0.78) in five different samples, including student, community and clinical participants. The authors also asserted that the MASQ subscales showed good convergent and discriminant validity across their five samples [10, 11].
Procedure
The MASQ was presented at either their first or second session to each participant, and was collected at the clinic as part of routine clinical practice outcome evaluation. Patients completed the questionnaire during their session at the clinic.
Results
All initial data cleaning, descriptive statistics, reliability coefficients and correlations were conducted using SPSS 12.0.1 (SPSS Inc., Chicago, IL, US) running on a Microsoft WindowsXP-based IBMcompatible personal computer. Subsequent confirmatory factor analyses were run under AMOS 5.0 (Smallwaters Corp., Chicago, IL, USA) using the same SPSS datafile and IBM-compatible computing equipment and operating system.
Before analysis, the data were also screened for univariate and multivariate outliers, resulting in 60 cases being removed from the dataset, leaving a sample size of n = 410.
Internal consistency and correlations of MASQ subscales
The reliability of the five MASQ subscales seemed adequate except for the MASQ-AD subscale. This subscale demonstrated inadequate internal consistency of α = 0.66. Reliabilities of the MASQ subscales are presented in the diagonal of Table 1.
Correlations between MASQ subscales for the entire sample (n = 470)
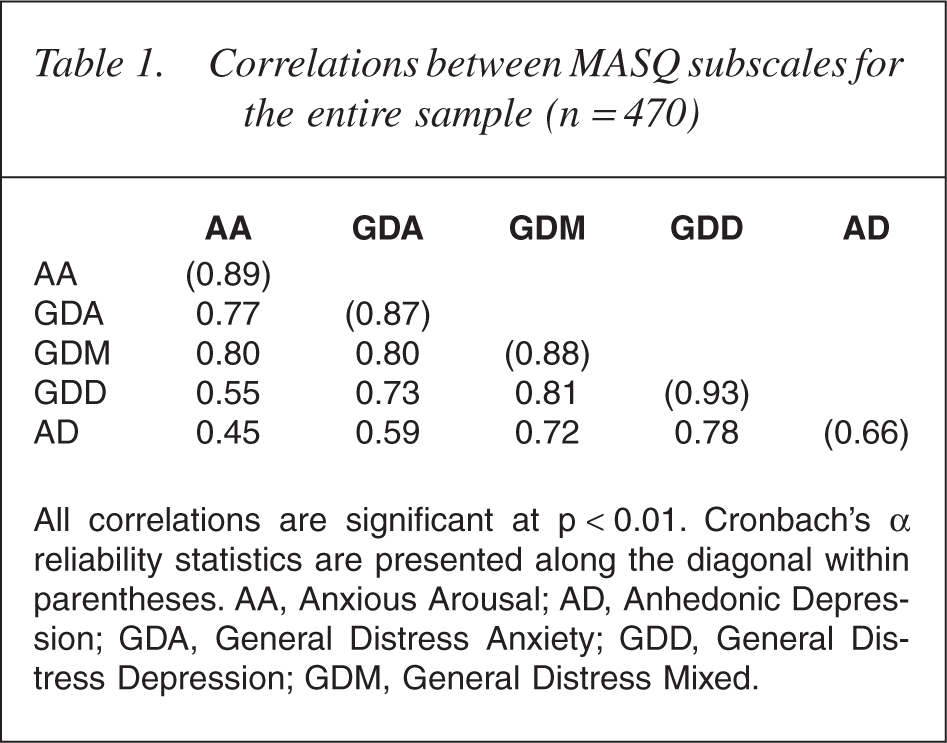
All correlations are significant at p < 0.01. Cronbach's α reliability statistics are presented along the diagonal within parentheses. AA, Anxious Arousal; AD, Anhedonic Depression; GDA, General Distress Anxiety; GDD, General Distress Depression; GDM, General Distress Mixed.
The tripartite model was developed with the aim of reducing the commonly observed covariance between anxiety and depression measures. Conceptually, the anxiety and depression specific subtests of the MASQ (MASQ-AA and MASQ-DD, respectively) should demonstrate weak correlations, indicating their specificity to one disorder. Table 1 shows the correlations of the MASQ subtests, revealing two noteworthy findings. First, there are extremely high correlations between subtests, suggesting that there is a large amount of redundancy. Second, it is clear that the correlation observed between the MASQ-AA and MASQAD subscales is significantly lower than that seen between less specific MASQ-GDA and MASQ-GDD subscales (r1 − r2 = 0.28, Z = 6.33, p < 0.0001).
Confirmatory factor analyses – rationale and sequence of model testing
Different approaches can be used in confirmatory factor analysis of a multi-subscale instrument like the MASQ. Using the five MASQ subscales as the unit of analysis allows assessment of the adherence of these subscales to a proposed factor structure. Alternatively, using the 90 items of the MASQ as the unit of analysis allows assessment of how well these items adhere to a particular structure.
In the present paper, both item-level and scale-level analyses are conducted. This more comprehensive analytic strategy was chosen for several reasons. First, it is known that item-level and scale-level analyses may yield different results. Each also measures subtly different aspects of model fit (latent structure of the subscales vs the substructure of items). Second, we sought to produce results that were comparable to both existing bodies of MASQ-related literature (that using itemlevel and scale-level analyses). Third, we wanted to produce a comprehensive evaluation of the MASQ's latent structure, examining the same dataset at the item and scale level.
A series of seven confirmatory factor analyses were conducted: three at the scale level and four at the item level of analysis. Because the most substantial criticism of the tripartite model was reported by Burns and Eidelson [14] using an incomplete set of MASQ scales, we sought first to clarify whether using the complete set of five MASQ scales would yield different results. As a result, scale-level analyses were considered first, followed by item-level models. Each model is based on a structure previously proposed (explicitly or implicitly) by previous researchers. The rationale for each individual model is given in the sections below.
Confirmatory factor analyses – scale-level analyses
Three confirmatory factor analyses were conducted at the scale-level unit of analysis. The first series of confirmatory factor analyses attempted to fit the five subscales of the MASQ to the hypothesized tripartite model. A total of three models were tested using MASQ scales as the unit of analysis, similarly to Burns and Eidelson [14]. Unlike Burns and Eidelson, all models tested incorporated all five of the MASQ subscales, including the MASQ-GDM subscale. Each of the models is introduced, explained and assessed in the following sections.
Confirmatory factor analytic procedures not only yield the loadings of measured variables on latent factors, but also provide a statistic measuring the overall ‘goodness-of-fit’ of the model to the dataset. Comparisons between different factor structures can be tested, allowing more direct comparison of competing models. Common practice in confirmatory factor analytic studies is to report not only the χ2 statistic, but also a number of statistics measuring goodness of fit and residual variance in the model, because of the effect of sample size on different indexes [17]. In addition to the χ2 statistic, the Normed Fit Index (NFI [18]), Goodness of Fit Index (GFI [19, 20]), Comparative Fit Index (CFI [21]), Root Mean Residuals and Root Mean Square Error of Approximation (RMSEA [22]) were calculated. For all models, AMOS 5.0, specifying a maximum likelihood estimation model, was used to calculate fit indices. All goodness-of-fit indices (NFI, GFI and CFI) were compared with a cut-off of ≥0.90 in determining adequate model fit. For the RMSEA, a cut-off of ≤0.05 was used. Modification indices were calculated by AMOS 5.0 based on whether addition of a path to the factor structure would improve model fit (χ2) significantly. These cut-offs are in line with current recommendations in the interpretation of Confirmatory Factor Analysis [23, 24].
Models which use scales as their unit of analyses require some parameters in the model to be estimated to achieve identification. In line with the recommendations of Jöreskog and Sörbom [19], the error variance for each of the subscales was estimated using the subscales alpha reliability and variance. This method has been demonstrated to be a sound approximation in determining error variance [25].
Model 1 – scale-level analysis, tripartite model, large NA factor
The first model tested (Model 1) attempted to fit the five subscales of the MASQ to a tripartite structure. For Model 1, a broad NA factor was considered, with all three of the MASQ General Distress subscales (MASQ-GDA, MASQ-GDD, MASQ-GDM) predicted to load on the latent NA factor. The MASQ-AD subscale was predicted to load on the depression-specific positive affectivity factor, while the MASQ-AA was predicted to load on the anxiety-specific Anxious Arousal factor (see Fig. 1). This model was not supported by the analysis. A summary table containing the results from the analyses of all models tested is provided in Table 2.
Models 1–3: scale-level analyses. NA, negative affectivity.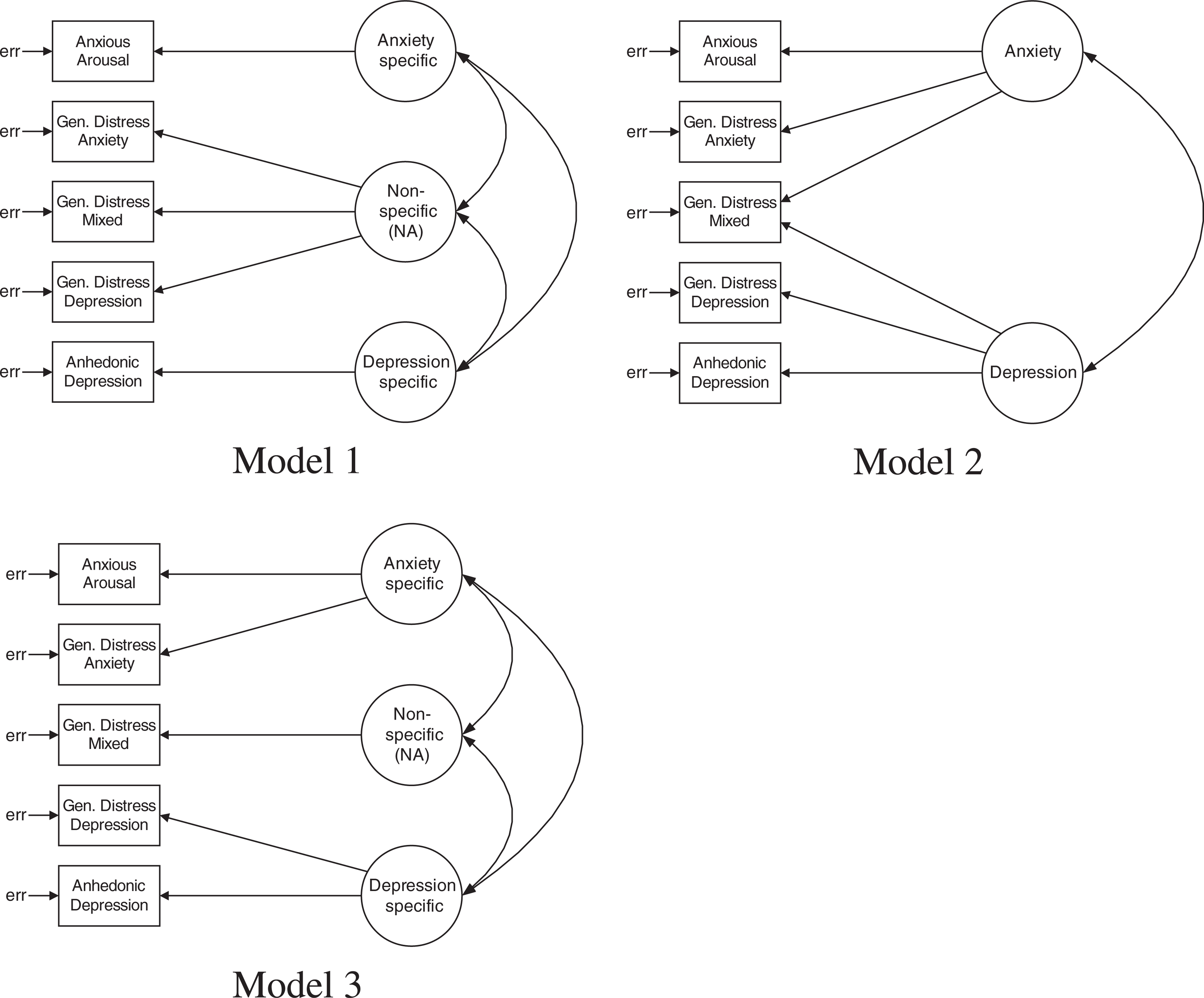
Summary table of results from confirmatory factor analyses
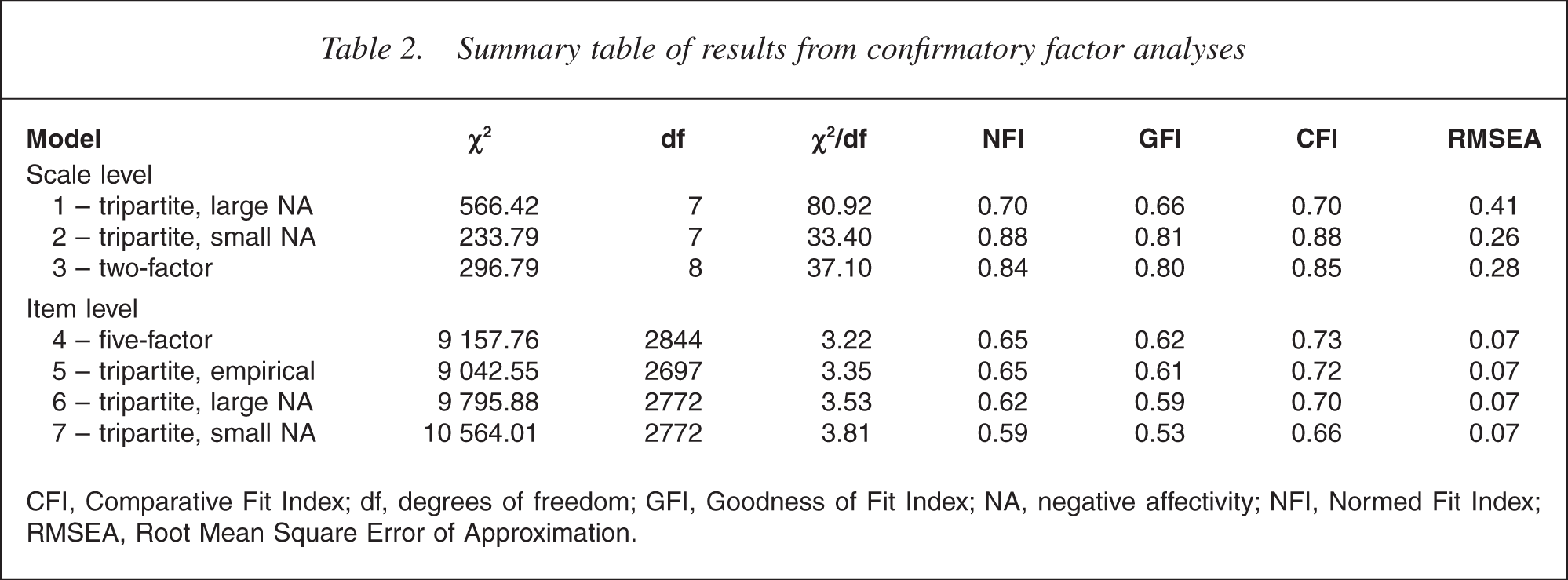
CFI, Comparative Fit Index; df, degrees of freedom; GFI, Goodness of Fit Index; NA, negative affectivity; NFI, Normed Fit Index; RMSEA, Root Mean Square Error of Approximation.
Model 2 – scale-level analysis, tripartite model, small NA factor
An alternative tripartite model was considered for Model 2. This was identical to Model 1, except that the MASQ-GDA and MASQ-GDD subscales were predicted to load onto the specific anxiety and depression factors rather than the non-specific NA factor (see Fig. 1). Model 2 also did not demonstrate adequate fit.
Model 3 – scale-level analysis, two-factor model
Burns and Eidelson advocated for a two-factor model where anxiety and depression were considered independent dimensions [14]. Their attempts to assess this excluded the MASQ-GDM subscale, as discussed earlier. Model 3 was a two-factor model, similar to that proposed by Burns and Eidelson, but incorporating loadings on both the anxiety and depression factors from the non-specific MASQ-GDM subscale (see Fig. 1). Unlike the analysis of Burns and Eidelson, however, this two-factor structure did not fit the current dataset (see Table 2).
Confirmatory factor analyses – item-level analyses
As has been discussed, the use of item-level or scale-level measured variables in confirmatory factor analyses can have a major impact on the results obtained [24]. A second series of confirmatory factor analyses were conducted using a similar procedure to that for Models 1–3, but using individual MASQ items as the measured variables. Each of the four item-level models is introduced and assessed below.
Model 4 – item-level analysis, five-factor model
The five-factor model tested (Model 4; see Table 2) was based on that published in the initial MASQ validation studies [10, 11]. In these studies, Watson et al. separated the items of the MASQ into five scales – AA, GDA, GDD, GDM and AD. The model initially tested here contained these five factors as latent variables, allowing factors to correlate freely. Correlations between items and error variances were held at zero, as were loadings of each item on scales other than its own. The first item to load on each factor had its loading set to 1 to allow for model identification (see Fig. 2).
Models 4–7: item-level analyses. NA, negative affectivity.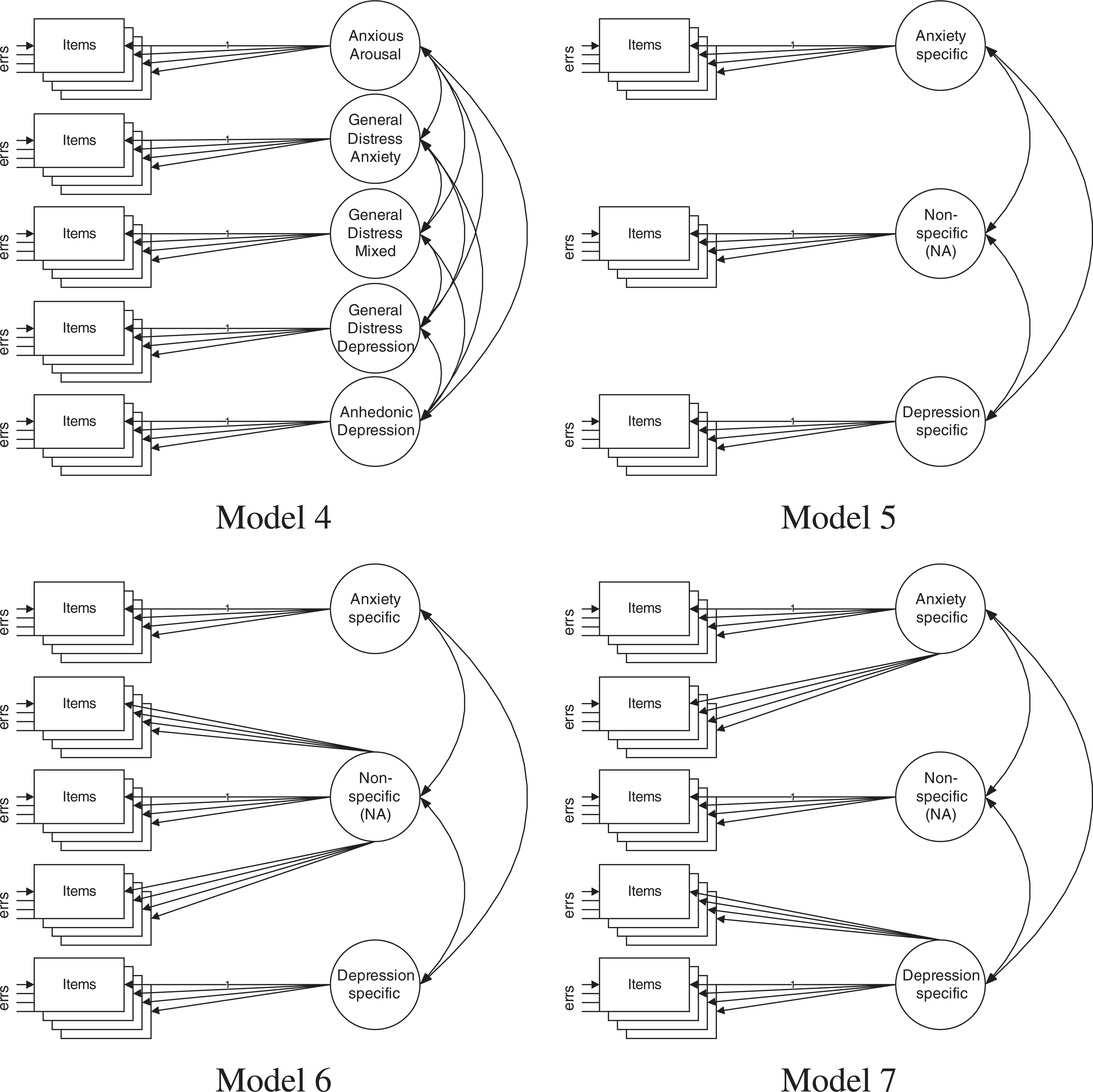
In the current clinical sample, the model did not adequately fit the dataset (see Table 2). The loadings of each of the items on their target factor were significant (with absolute standardized regression weights between 0.35 and 0.84, suggesting that no paths in the model were clear candidates for removal. While the intention had also been to examine the model for modifications that would enhance fit, AMOS returned a total of 92 potential additional new factor loadings that were expected to significantly improve the χ2 statistic. Within these loadings, 12 involved suggestions that items should be allowed to load on all five factors. Obviously, such modification would render the model unrecognizable in comparison with that used in the initial validation study. It was concluded at this point that the model was not close enough to fitting the five-factor model to warrant modification and retesting.
Model 5 – item-level analysis, tripartite model, empirically derived
The first three-factor model to be assessed at the item level (Model 5) was that derived empirically during the initial MASQ validation studies. After Watson et al. had constructed their instrument, they proceeded to conduct a factor analysis using the combined data from their large dataset, forcing a three-factor solution. For Model 5, each item was assumed to load on the factor onto which it had the highest loading in the validation sample [11], and was not permitted to load on other factors. The first loading on each factor was set to 1 to achieve model identification, and items and error variances were constrained to zero. Factors were permitted to correlate freely (see Fig. 2).
The empirically derived three-factor model from Watson et al. [11] was not replicated in the current dataset. Model 5 failed to fit the data (see Table 2). All items loaded significantly on their hypothesized underlying factor, with absolute loadings from 0.39 to 0.80, suggesting the removal of no paths between items and factors. A total of 48 new loadings were suggested on the basis of the modification indices returned by the analysis. Similarly to previously, model modification was not conducted because of the extremely poor fit of the model, the numerous suggestions for model change which would render the final product unrecognizable, and the fact that only one suggested additional loading exceeded a modification index of 20.
Model 6 – item-level analysis, tripartite model, large NA factor
The second tripartite model to be assessed at the item level (Model 6) used the scales provided from the initial validation studies of the MASQ. A three-factor model where the specific subscales of the MASQ each load on their own anxiety-specific or depression-specific factor, and where all items from all three General Distress scales are proposed to load on a single non-specific factor, was tested (see Fig. 2). The fit of the data to this tripartite model was poor, with inadequate scores on all of the measures of fit used (see Table 2).
Model 7 – item-level analysis, tripartite model, small NA factor
The next tripartite model to be tested was similar to the previously tested model, insofar as it was based on the five MASQ scales derived in the initial validation study. In contrast to the previous analysis, however, this analysis forced the MASQ-GDA subscale to load on the anxiety-specific factor (rather than the non-specific factor), while the description of the pattern in the participants' anxiety and depression MASQ-GDD subscale was required to load exclusively on the depres-symptomssion-specific factor. This left a smaller number of items from the MASQ-GDM scale to load on the hypothesized non-specific factor (Fig. 2).
When Model 7 was tested, it failed to adequately fit the current dataset. Indices of fit revealed poor fit of the model to the data provided (see Table 2) and suggested numerous (69) additional loading paths for the model. With such poor fit and extensive model modification suggestions, it was concluded that the tripartite model was not a successful description of the pattern in the participants' anxiety and depression symptoms.
Summary of confirmatory factor analytic results
The results of the confirmatory factor analyses for all seven of the tested models are presented in Table 2. Several things are noteworthy when the models are compared. First, none of the models tested, either using items or subscales as their unit of analysis, showed adequate fit to the data. Second, it is clear that models which used the subscale totals as their measured variables (Models 1–3) showed somewhat better fit than those which used items (Models 4–7).
Discussion
Our results showed that the pattern of correlations between the MASQ subscales did fit the expected pattern proposed by the tripartite model. It was expected that anx-iety-specific and depression-specific subscales would show the weakest correlations, while non-specific general distress scales would show stronger relationships. All subscales were correlated significantly. Importantly, the weakest correlation observed was between the two specific subscales (MASQ-AA and MASQ-AD), and this was substantially less than the typically observed correlations between anxiety and depression self-report inventories of 0.62–0.70. Previous authors (e.g. [10, 11]). have used such correlation tables as evidence in support of the tripartite model structure of the MASQ. It is suggested here that such evidence is insufficient in support of such a structure unless it is supported by more sophisticated statistical procedures such as confirmatory factor analysis.
The internal consistency of the MASQ-AD subscale was shown to be particularly poor in the current investigation. As discussed earlier, this subscale was constructed post-hoc from three factors that emerged from exploratory factor analysis [11]. It is suggested here that the poor internal consistency of this subscale is an artefact of the procedure used in building this subscale.
Attempts were made to fit seven different alternative solutions to the clinical dataset. Analyses using items and scales as the unit of analysis were conducted, with poor results in every case. The MASQ items are divided into five subscales based on the exploratory factor analyses conducted by the scale's authors. This structure was not supported by the current research using a anxious/ depressed clinical sample. The present study is the first attempt to replicate the item structure of the MASQ in a anxious/depressed sample using confirmatory factor analytic procedures at the item and scale level. The use of an anxious/depressed sample in the current study rather than a group with substance-use problems may have resulted in findings different to Watson et al. [11]. Similarly to Keogh and Reidy [12], it is concluded that the original factor structure of the MASQ is not as stable across different sample as initially suggested by Watson et al. and may be in need of considerable refinement.
Burns and Eidelson argued that the MASQ was better described in terms of a two-factor anxiety/depression structure [14]. Flaws in the statistical methods used to reach these conclusions have been discussed previously.
The current dataset did not support a two-factor model at either the item or scale level of analysis. The twofactor structure advocated by Burns and Eidelson stands in contrast to the consensus in the literature which supports a three-factor symptom structure over an anxiety versus depression distinction. The use of the complete MASQ in the present study, rather than excluding the MASQ-GDM items and scale, has likely contributed to our inability to identify a two-factor structure. The results here are presented as a more complete assessment of the adherence of the MASQ to a two-factor structure than those of Burns and Eidelson.
Three features of our study should be kept in mind while interpreting our results. The first of these is that confirmatory factor analysis is a particularly conservative test of the fit of our data to the tripartite model. While our MASQ data did not adhere to the strict models we assessed, this may be in part due to the stringent statistical criteria used to evaluate model fit. Readers should be mindful of the conservative criteria used to assess the MASQ latent structure when integrating our findings with previous MASQ research. Second, diagnosis was made on the basis of a clinical interview, rather than using a structured interview method such as the Structured Clinical Interview for Diagnosis. Furthermore, no data were available to assess interclinician diagnostic reliability. While all diagnoses were confirmed by a second senior clinician, the limitations to such a diagnostic method should be borne in mind. Third, for the anxiety samples used in this study, a heterogenous group of anxiety disorders were collapsed into a single group. There are known differences between the anxiety disorders in how each relates to a tripartite structure which have not been assessed in our research [4]. This is an important consideration in interpreting our findings.
The present study was conceived as an attempt to generalize the tripartite structure of the MASQ to an anxious/ depressed sample, but was unable to do so. Both itemand scale-level attempts to fit three-factor models were unsuccessful. Analyses where the NA factor was defined either broadly or narrowly also did not yield acceptable fit to the data. These results contrast with previous findings that have supported the tripartite structure in the MASQ, as well as in other instruments. The consistent difference between this study and previous research is the use of an anxious/depressed sample. There is little reason to suspect that the use of an Australian clinical sample would impact significantly on results. From these results, the utility of the MASQ as a measure of tripartite factors in an anxious or depressed population is questionable.
Other than the consistent failure to support the tripartite structure in the MASQ in the current sample, a number of other conclusions can be suggested from the analyses. First, there is little doubt that any assessment of the MASQ or future inventories must make use of multiple different statistical methods. In the present study, the pattern of correlation appeared to support a tripartite structure, but more sophisticated methods of analysis revealed that such a structure was weak. Future research into the tripartite model must endeavour to conduct a comprehensive assessment using a broad array of techniques including confirmatory factor analysis.
Although none of the models tested showed adequate fit to the sample data, there was substantial variation in how closely they approached good fit. As shown in Table 2, there is marked difference between the fit of some of the scale-level models and their item-level counterparts. This supports previous authors (e.g. [26]) who have highlighted the importance of investigating factor structure at the item and subscale level. The inability of the MASQ to fit either item- or subscale-level models is problematic.
Conclusions
In summary, the present study supported none of the tested models of the structure of the 90 MASQ items. The MASQ appears to be insufficiently stable across samples as a measure of tripartite model constructs. At this point, it is recommended that future researchers and clinicians using the MASQ remain mindful of the limitations in its psychometric properties.
Despite the weaknesses in the MASQ highlighted by this study, there remains a substantial body of research in support of a tripartite/integrated-hierarchical model of anxiety and depression symptoms. Failure of the MASQ in an anxious/depressed sample suggests the need for an alternative measure, derived using a more rigorous statistical methodology, for clinical use. The construction of such an instrument is currently underway by the authors of the present study.
Footnotes
Acknowledgements
The authors would like to thank Professor Murray Dyck for his valuable input on an earlier draft of this paper.