
Abstract
People with mental disorders, particularly with more serious mental illness, are substantially more likely to experience violent victimization than the general population [1–3]. For example, the one-year prevalence of violent victimization was found to be 16% in a recent UK study of community dwelling patients with psychosis [2], while a US study found the prevalence of different types of violent crime was 6–23 times higher among people with a serious mental illness than among the general population [4]. However, a history of victimization is often undetected by mental health workers and seldom influences treatment decisions [5, 6]. Furthermore, the rate of comorbid posttraumatic stress disorder (PTSD) secondary to victimization has been largely ignored as an important mediating factor of the detrimental effects of victimization. The aims of this study are to establish in an Australian population the lifetime prevalence of victimization, aggressive behaviour and PTSD in a cohort of hospitalized psychiatric patients and to measure the impact of victimization on the longitudinal course of their mental illness and associated disability.
Method
The study was conducted at the inpatient psychiatric unit of the Queen Elizabeth Hospital in Adelaide, South Australia for 12 months from May 2003. All patients admitted to the unit for longer than two full days during this time, irrespective of diagnosis, were eligible to participate in the study, unless they were unable to comprehend written or spoken English or were intellectually impaired. Patients who were admitted to and discharged from the closed unit were also excluded. As soon as the treating team assessed they were well enough to participate, patients were approached by a research assistant and after giving informed consent, they completed an interview and several questionnaires.
Instruments
The following instruments were administered:
The Traumatic Antecedents Questionnaire (TAQ) [7]. This 42-item structured instrument determines the respondent's experience of a range of traumatic events including physical and/or sexual victimization occurring during four designated epochs: early childhood (0–6), childhood (7–12), adolescence (13–18) or adulthood. The Posttraumatic Stress Disorder and Substance Abuse sections of the Composite International Diagnostic Interview [8]. The Past Feelings and Acts of Violence Scale (PFAV) [9], a brief (12-item) self-report scale designed to assess the presence of angry feelings and tendency to act violently. The Aggression Questionnaire (AQ) [10], a 29-item self-report questionnaire measuring four aspects of aggression: physical, verbal, anger and hostility. The internal consistency of the AQ is very good and it has good test–retest reliability. The Suicidality section of the Mini International Neuropsychiatric Interview [11]. Participants in the current study were rated as being at low, moderate or high risk of suicide. Sociodemographic data were gathered by self-report. Diagnosis was that recorded in the discharge summary. Measures of adverse course of illness included pension status, which was determined by self-report, and number of previous admissions which was derived from a statewide database of all psychiatric admissions.
Data analysis
Results were analysed using SPSS for Windows (SPSS Inc., Chicago, IL, US) [12]. Comparisons between patients who had and had not experienced victimization were made on a range of measures using either t-tests or chi-squared tests (χ2), presenting results, where appropriate, as relative risks (RR) with 95% confidence intervals (CI).
Results
Recruitment
Between May 2003 and April 2004, 623 patients were admitted to the Queen Elizabeth Hospital psychiatric unit. This inpatient unit has a high turnover of patients as a result of considerable pressure for admission from the community mental health teams of service. Of those, 207 (33.2%) were ineligible to participate owing to either brief admission, admission into the closed unit, inability to speak English or being deemed unsuitable for inclusion by their doctor because of the severity of their illness. Of the remaining 416 patients (66.8%) eligible to participate, 58 (13.9%) were discharged before they could be approached, 192 (46.2%) refused to participate while 166 (39.9%) consented. Of those who gave consent, 36 failed to complete the interview, leaving a final completion rate of 130 (31.3%) of those eligible. To ensure representativeness of the sample, participants were compared with non-participants regarding sex, age and length of stay. There were no significant differences between participants and non-participants with respect to age and sex; however, on average, the non-participants spent significantly less time (mean = 14.9 days, SD = 19.8) in hospital than the participants (mean = 23.5 days, SD = 24) (t(177) = −3.75, p < 0.001).
Demographic characteristics
The age of the 130 psychiatric inpatient participants ranged from 18 to 65 years with a mean age of 36.8 years (SD = 11.9). There were 69 (53.1%) men in the sample and 61 (46.9%) women. Fifty-three per cent were admitted voluntarily. The most frequent diagnosis was that of psychosis (40%), followed by depression (25%), bipolar disorder (17%) and adjustment disorder (15%). Twenty per cent of the sample had never been admitted to a psychiatric facility before, while 62% had two or more previous admissions. The majority of the participants were born in Australia (84%), and half currently lived on their own. Sixtyone per cent of the participants were currently receiving a pension, 85.4% were single or divorced, 65% had not completed high school education and 47% had no children. Some form of suicidal ideation was currently experienced by 81.5% of the sample and 62% were in the high-risk category.
Prevalence of victimization
According to the TAQ, a lifetime history of victimization was reported by 87.7% of patients. Eighty-four per cent of the participants had experienced physical assault and 56.9% had experienced sexual assault in their lifetime, while only 16 (12.3%) had never experienced any sort of victimization. Twenty-eight per cent of sexual assault victims and 31% of physical assault victims described the abuse as happening ‘often’ at some point in their life. Seventy-two (55.4%) participants had experienced both sexual and physical victimization, the majority of these (70.8%) beginning before the age of 18 years. Fifty-six per cent of victims did not have significant victimization experiences recorded in their case notes. While men in the sample were significantly more likely to experience physical victimization during childhood (χ2 = 7.5, RR = 2.8, CI = 1.3–5.9, p = 0.007) than women, women were more likely to experience lifetime sexual victimization (χ2 = 10.5, RR = 3.4, CI = 1.6–7.0, p = 0.001) and a combination of physical and sexual victimization (χ2 = 10.1, RR = 3.2, CI = 1.5–6.6, p = 0.002) than men (see Table 1). Of the 64 individuals experiencing sexual victimization before the age of 18 years, 23 (35.9%) were sub sequently sexually revictimized in adulthood. Twenty-one (91.3%) of those revictimized were female.
Victimization experience by gender
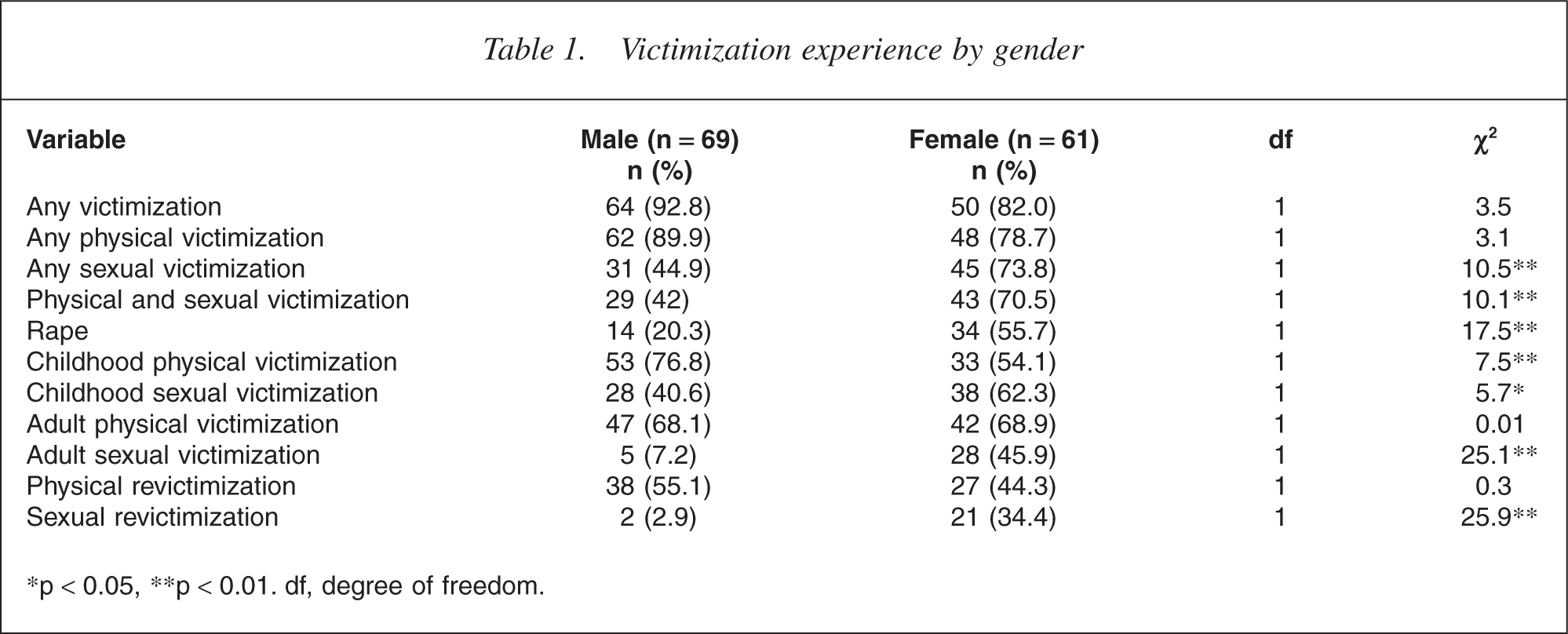
∗p < 0.05, ∗∗p < 0.01. df, degree of freedom.
A modest association was found between history of physical assault and lifetime drug and alcohol dependence or abuse, with those who had a lifetime substance abuse problem almost three times more likely to have been physically assaulted. On closer examination, however, there were no significant differences between those who had experienced physical victimization, either only as children or only as adults, and those who were not victimized in relation to drug abuse history. There was a higher-than-expected incidence of lifetime drug abuse or dependence among those who experienced physical assault during childhood and were revictimized during adulthood, compared with the rest of the sample (66.7% vs 36.9%, χ2 = 11.3, RR = 3.4, CI = 1.7–7.1, p = 0.001). There was a higher incidence of alcohol abuse among those who had experienced physical assault during adulthood (59.1% vs 34.1%, χ2 = 7, RR = 2.8, CI = 1.3–6.0, p = 0.009) compared with those who were not physically assaulted in adulthood.
Participants who had experienced any victimization had higher mean aggression scores as measured by the AQ (mean = 85.3, SD = 18.4) compared with those who had not experienced victimization (mean = 66.7, SD = 19.7) (t(128) = −3.8, p < 0.001, see Table 2). According to the PFAV, 66% of participants had committed at least one act of violence towards someone else in the past and 42% had assaulted members of their family. Twenty-two per cent of the sample had been arrested for violent acts in the past. Participants who had experienced victimization had higher mean violence scores as measured by the PFAV (mean = 6.5, SD = 4) compared with those who had not been victimized (mean = 3.8, SD = 4) (t(128) = 1.96, p = 0.026), and were more likely to be classified as violent according to PFAV criteria (χ2 = 6.4, RR = 4.8, CI = 1.3–17.8, p = 0.019). There was a significant difference in PFAV violence classification between those who had experienced physical violence during both childhood and adulthood and those who had never experienced physical assault (χ2 = 14.2, RR = 9.7, CI = 2.6–36.5, p = 0.001).
Demographic and clinical characteristics of the sample by victim status
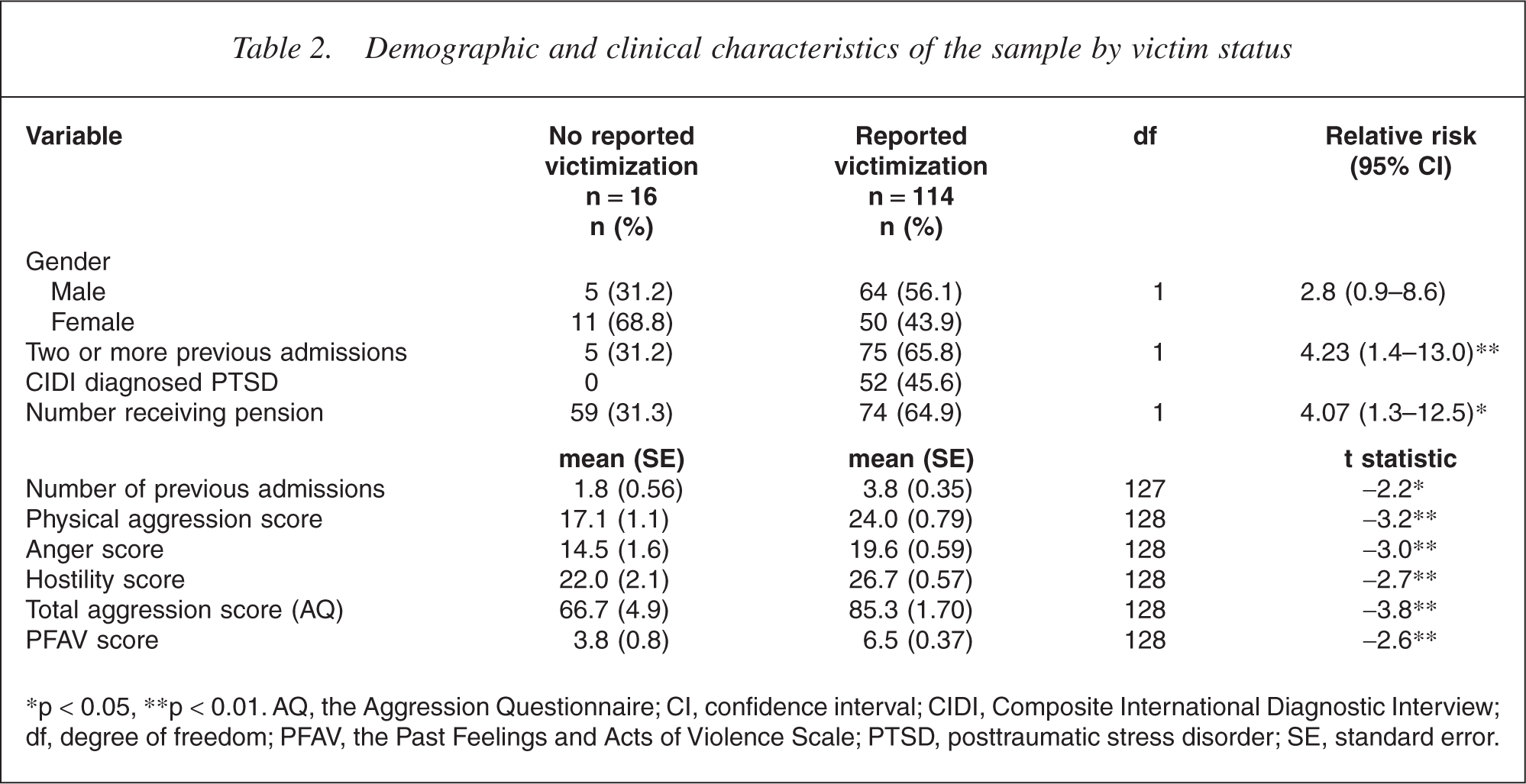
∗p < 0.05, ∗∗p < 0.01. AQ, the Aggression Questionnaire; CI, confidence interval; CIDI, Composite International Diagnostic Interview; df, degree of freedom; PFAV, the Past Feelings and Acts of Violence Scale; PTSD, posttraumatic stress disorder; SE, standard error.
Victimization and adverse outcome
Participants who had experienced any lifetime victimization were significantly more likely to be receiving the disability support pension (64.9% vs 31.3%, χ2 = 6.7, RR = 4.1, CI = 1.3–12.5, p = 0.014) and had, on average, more previous psychiatric admissions (mean = 3.8, SD = 3.6) compared with those who had not experienced victimization (mean = 1.8, SD = 2.2) (t(127) = −2.2, p = 0.032, see Table 2). Those who had experienced any childhood victimization were also more likely to be on the pension (χ2 = 6.7, RR = 3.6, p = 0.025) and had more previous psychiatric admissions (mean = 3.8, SD = 3.5) than those who were not victimized (mean = 1.8, SD = 2.2) (t(114) = −2.2, p = 0.029). Participants who had experienced lifetime sexual victimization were also significantly more likely to have been divorced (52.6% vs 26.4%, 2 = 8.8, RR = 3.1, CI = 1.4–6.6, p = 0.004).
Victimization and PTSD
According to the Composite International Diagnostic Interview, 52 (40%) participants had suffered from PTSD during their lifetime, with 36 (28%) reporting current symptoms. However, only seven (5.4%) patients were documented as having this diagnosis in their case notes. The incidence of lifetime PTSD was significantly higher than expected among the victimized group (46%, χ2 = 12.3, p < 0.001), and was highest among those who experienced sexual victimization often during a period of their life (85.7%, χ2 = 8.8, p = 0.003). Victims who had lifetime incidence of PTSD were more likely to be female (χ2 = 6, RR = 2.6, CI = 1.2–5.6, p = 0.015) and more likely to have made a suicide attempt in the past (χ2 = 8.9, RR = 3.6, CI = 1.5–8.4, p = 0.004) than victims who had never suffered from PTSD (see Table 3).
Characteristics of victims with and without PTSD (CIDI)
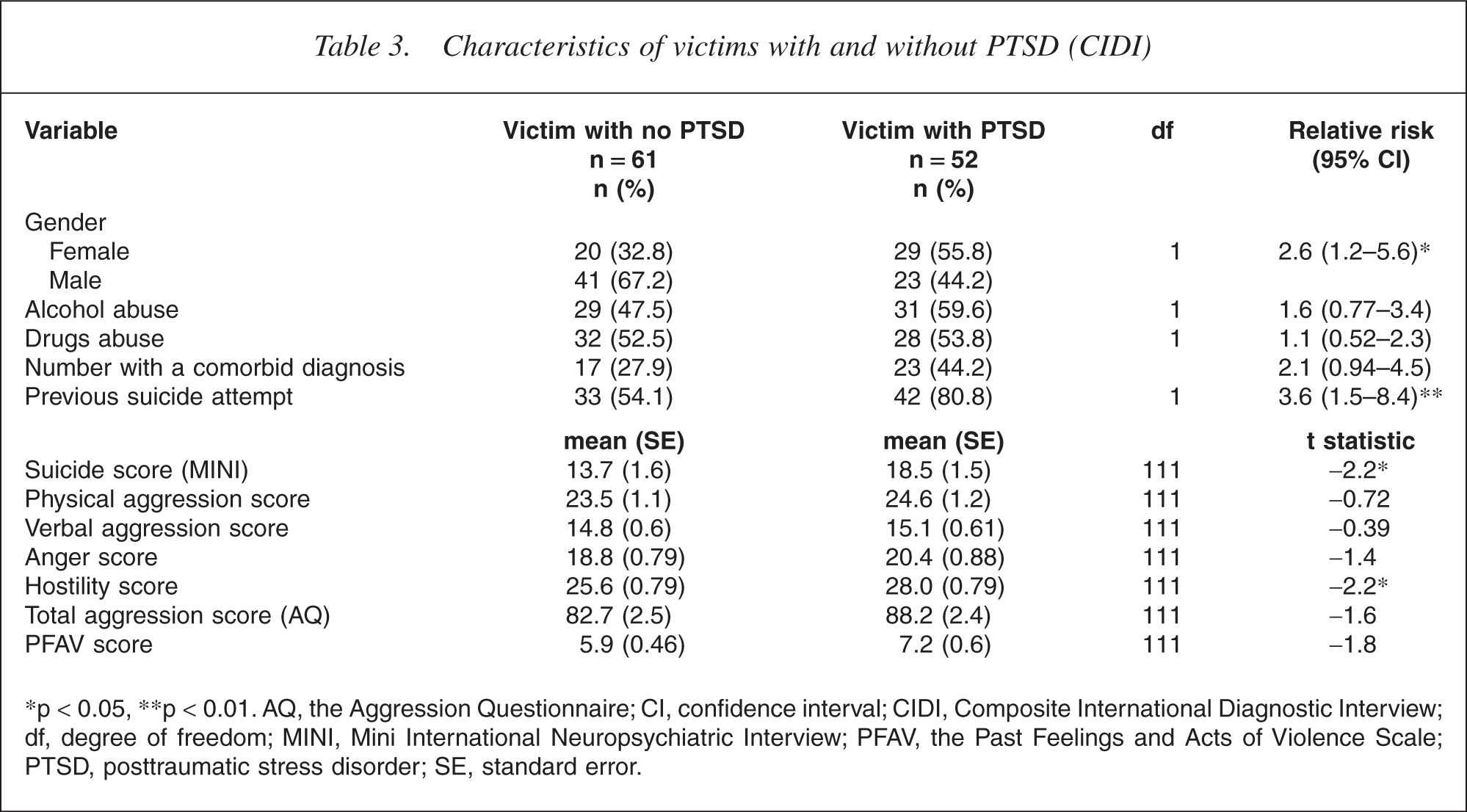
∗p < 0.05, ∗∗p < 0.01. AQ, the Aggression Questionnaire; CI, confidence interval; CIDI, Composite International Diagnostic Interview; df, degree of freedom; MINI, Mini International Neuropsychiatric Interview; PFAV, the Past Feelings and Acts of Violence Scale; PTSD, posttraumatic stress disorder; SE, standard error.
Discussion
This study provides further evidence for high lifetime rates of physical and/or sexual victimization in both men and women with psychiatric disorder, with more than half the cohort reporting histories of both sexual and physical victimization. Previous studies have reported similar high prevalence rates of victimization, and while some Australian studies have reported high lifetime prevalence of traumatic life events [5] and high rates of recent physical assault [13] among psychiatric inpatients, this is the first report of prevalence rates of lifetime sexual and physical victimization in psychiatric patients in an Australian population. Of note, more than half of those who were victimized did not have these significant events documented in their case notes, and while the study found high rates of PTSD in this population, this diagnosis was only rarely reported in the case notes.
Previous research has found a significant relationship between substance abuse and various types of lifetime victimization experiences among patients in treatment for substance abuse [14, 15] and psychiatric patients [16]. Heffernan et al. found that opiate use was more common among those reporting a history of childhood physical abuse in a sample of psychiatric inpatients [17]. The current study indicates that history of drug abuse was most common among those who had suffered physical assault in both childhood and adulthood and a history of alcohol abuse was most common among those who experienced any physical victimization in adulthood. The finding that a history of victimization, especially physical assault, was associated with significantly higher aggression and violence scores is consistent with previously published literature. Those who experienced physical victimization during both childhood and adulthood were most likely to engage in violent behaviour, providing support for the cumulative association between victimization and violence [18]. Among a mentally ill population, the experience of victimization rarely occurs in isolation, but rather is likely to co-occur with various experiences, such as substance abuse problems, poverty or psychosis. Previous research has found such experiences to be risk factors for violent behaviour, and it has been suggested that each factor can make an independent and accumulating contribution to violent behaviour [17]. However, as the sample size in the current study was insufficient to perform a multivariate analysis, the interrelationship between victimization, substance abuse and violence could not be investigated.
While the study was retrospective, there were significant associations between a lifetime history of victimization and two variables which indicate a less functional longitudinal natural history of illness, namely, number of previous admissions for psychiatric disorder and being in receipt of a disability pension. Previous research [19] has found an association between severity of mental illness and victimization among the mentally ill and it could therefore be argued that victimization experiences, rather than being a risk factor for poor outcomes such as multiple psychiatric admissions or receiving a pension, are merely another outcome of a more severe mental illness. However, the vast majority of victims in the current study first suffered victimization in childhood, before the onset of adult mental illness. And of note, the experience of childhood victimization was associated significantly with these poorer outcomes. Victimization experienced in childhood may possibly contribute to poorer outcomes in adulthood by increasing the risk of revictimization in adulthood or by increasing the risk of developing psychological symptoms and disorders [20]. The association between history of victimization and adverse outcome is of considerable interest as it highlights the adverse impact which victimization may have on the resilience of a person who has a mental illness. It may also have implications in terms of the economic cost to the community of providing ongoing health care to people with mental illness. The findings provide evidence that irrespective of how victimization is aetiologically related to mental illness, such experiences may have a deleterious effect on the longitudinal natural history of mental illness.
The high rates, both current and lifetime of PTSD as a consequence of victimization, were not routinely reported in the case notes as an important comorbidity in these patients. The interaction between PTSD and the patient's primary disorder has potential clinical implications that require further exploration, both as a risk factor to the onset of presenting psychosis and as a factor impacting on the prognosis. The presence of PTSD in a substantial number of those patients highlights their ongoing distress and preoccupation with the assault they have experienced. For example, victims with PTSD were more likely to have attempted suicide in the past and currently experienced more suicidal ideation than victims who did not suffer from PTSD. Further, the associated avoidance and numbing are likely to further the disability experienced by those patients.
Limitations of this study include the relatively low numbers of patients interviewed. Although the sample was representative of the majority of patients admitted to the psychiatric inpatient facility over a 12-month period, the most severely mentally ill patients were by necessity excluded from the study, and to that extent, it is unclear whether the victimization experiences of those who participated were representative of the rates of victimization in the broader patient population. While the reliability of self-report of victimization has been questioned in patients with psychiatric disorders, there is evidence to support the accuracy of these reports [21]. The TAQ which was utilized for determining lifetime history of victimization has the advantage of clearly defined epochs which assisted recollection of specific events. Measures of adverse outcome such as pension status were determined via self-report and verified from patient case notes, while numbers of previous psychiatric admissions were reliably determined from the statewide register.
In conclusion, this study highlights that psychiatric patients are not just perpetrators of violence but also very often the victims of such acts. The increased levels of aggression and hostility in patients with a history of victimization indicate that there is likely to be a complex interrelationship between a patient's potential for violence and their history of being a victim of assault. In an era where there is increased community care of severely ill patients, these findings require careful consideration, at the least they suggest those with mental illness are a highly vulnerable group to physical and sexual assault. Our findings suggest that violent social environments may mitigate against resolution of chronic psychiatric illness and may in fact lead to recidivism and the subsequent escalation of social and economic burdens. Future mental health reform policy needs to take account rates of crime and violence in community environments where patients are often placed.
Footnotes
Acknowledgements
This research was funded by the Criminology Research Council of Australia.