
Abstract
The mental health consumer movement has been instrumental in drawing the attention of mental health providers, researchers and policy-makers towards the concept of recovery from schizophrenia. Consumers are advocating that mental health services should be recovery-orientated [1–3] and, indeed, this notion is being incorporated internationally into mental health policy [4–7]. To achieve this, programmes based on a consumer-orientated model of recovery need to be developed, and a recovery measure based on such a consumer model is required to enable further research into the processes of recovery. Measures of symptoms, hospitalizations or functioning are based on a medical model of mental illness, and are often in conflict with the consumer definition of recovery. A consumer-orientated definition of recovery, psychological recovery, has been described as ‘the establishment of a fulfilling, meaningful life and a positive sense of identity founded on hopefulness and self-determination’ [8], p. 588]. This definition describes recovery from the psychological trauma of the illness rather than a cure or the absence of symptoms [9]. Andresen et al. [8] have advanced a model of recovery based on accounts of consumers' experiences. By thematically analysing a large number of personal accounts of recovery, four key component processes of recovery were identified: (i) finding and maintaining hope; (ii) the reestablishment of a positive identity; (iii) finding meaning in life; and (iv) taking responsibility for one's life. In addition to these individual accounts, a number of qualitative studies were examined which described stages or phases of the recovery process [10–14]. In consolidating the findings from five studies five stages of recovery were proposed, briefly:
Moratorium: A time of withdrawal characterized by a profound sense of loss and hopelessness. Awareness: Realization that all is not lost, and that a fulfilling life is possible. Preparation: Taking stock of strengths and weaknesses regarding recovery, and starting to work on developing recovery skills. Rebuilding: Actively working towards a positive identity, setting meaningful goals and taking control of one's life. Growth: Living a full and meaningful life, characterized by self-management of the illness, resilience and a positive sense of self.
The stage model of recovery, consisting of the four component processes and five stages, combines these findings in a model of the personal experience of psychological recovery. The stages are sequential, with the ‘Growth’ stage representing the outcome of the recovery process. The component processes represent the psychological state of the person as he or she progresses through the stages of recovery. Due to the highly personal nature of recovery, the model is purposely flexible in terms of the timeframe and the means by which the person moves through this process. That is, each individual finds his or her own sources of hope and ways of finding meaning and building a positive identity.
It is tempting to draw parallels between this model of recovery and Prochaska and DiClemente's Transtheoretical Model (TTM) of health behaviour change [e.g. 15,16], as on the surface the five stages sound similar. However, there are some important differences. Whereas the TTM addresses changes in specific health-related behaviours (such as alcohol abuse), the stage model of recovery is a holistic model which emphasizes the subjective psychological process of recovery from the devastating effects of being diagnosed with a serious mental illness. Specific behaviours are not emphasized. The stage model of recovery was developed from consumers' personal accounts of their experience, with no reference to the TTM. (For a detailed description of the process of developing the model, see Andresen et al. [8]).
Consumers stress the complex and non-linear nature of recovery, and hold that individuals in the highest level of recovery may still suffer a relapse of symptoms. This does not mean that they have returned to an earlier stage. Although set-backs or a recurrence of symptoms undoubtedly have an impact on a person's happiness, an important outcome of recovery is resilience. Resiliency is the process of coping with disruptions in a way that enhances protective factors [17]. The ability to manage a relapse of symptoms – even if this requires the use of hospital services – and a return to the previous state of wellbeing is central to recovery. As part of the normal growth process, the person may choose to reassess his or her lifestyle or goals and make adjustments as deemed necessary [e.g. 18–21].
When validated, the model could be utilized in further research into the promotion of recovery, the training of mental health professionals and the education of consumers and carers. However, in order to empirically validate the model, a measure that reflects the processes and stages is needed. We searched for existing measures of recovery, and as we could not find one concordant with the stage model, we developed a new measure. In this paper, we review the existing measures and describe the development of the stages of recovery instrument (STORI) and initial psychometric testing.
Existing measures of recovery
Computerized database searches using permutations of the terms recovery/measure/measurement/assessment and mental/schizophrenia/psychosis/psychiatric located only one measure of recovery with a related published article, the Recovery Assessment Scale (RAS) [22]. A compendium of the known published and unpublished measures of recovery was subsequently examined [23]. Eight measures included in the compendium were described as measures of recovery, with the remainder being measures of various recovery-related concepts.
To test the model, we looked for measures that met three criteria: (i) the measure must attempt to assess a concept of recovery based on qualitative work with consumers; (ii) development of a model or the measure and/ or testing must have been published in a peer-reviewed journal; and (iii) the measure must be self-rated and suitable for quantitative analysis. Of those that were described as measures of recovery, only two met these criteria: the RAS [22], and the Mental Health Recovery Measure (MHRM) [10, 23]. We examined these two mea sures to assess their suitability for testing the stage model of recovery.
The Recovery Assessment Scale (RAS)
Items for this scale were based on the narratives of four consumers, and were reviewed by a second group of 12 consumers. The RAS consists of 41 items and yields a single score of recovery. The scale was tested with 35 consumers with a diagnosis of a severe mental illness and returned acceptable test–retest reliability (r = 0.88) and internal consistency (〈 = 0.93). Concurrent validity was demonstrated with self-esteem and self-orientation to empowerment. The RAS correlated positively with social support and quality of life, and negatively with psychiatric symptoms and age. Corrigan et al. [24] later conducted a factor analysis that resulted in five factors totalling 24 items. The factors Personal Confidence and Hope, Willingness to ask for Help, Not Dominated by Symptoms; and Goal and Success Orientation are conceptually related to the component processes of the stage model of recovery. However, Ability to Rely on Others which includes items such as ‘I have people I can count on’ and ‘It is important to have a variety of friends’ represents interpersonal issues that assist recovery, rather than the personal experience of psychological recovery. Surprisingly, the factor analysis resulted in the omission of all items referring to self-management of symptoms which appeared to be an important theme in our review of the experiential literature. Although the RAS was not based on a theoretical or conceptual model of recovery the majority of items retained by the factor analysis reflect the definition of psychological recovery. However, the RAS does not attempt to identify stages of recovery, but is a continuous measure yielding a single recovery score.
The Mental Health Recovery Measure (MHRM)
Following interviews and focus groups with 18 consumers Young and Ensing [10] outlined a three-phase model of recovery consisting of six aspects: Phase I, Overcoming stuckness; Phase II, Discovering and fostering self-empowerment, Learning and self-redefinition, and Return to basic functioning; and Phase III, Striving to attain overall wellbeing and Striving to reach new potentials. The MHRM is a 41-item scale that comprises six subscales assessing these six aspects of recovery. Results of psychometric testing are contained in the Compendium and include coefficient alpha for the total scale (〈 = 0.91) and for the subscales (〈 = 0.55–0.83). The MHRM showed convergent validity with the Community Living Skills Scale [25] (r = 0.75) and a measure of empowerment (r = 0.52). Although the six subscales of the MHRM are conceptually related to the four component processes in the stage model of recovery, the measure contains value statements and behavioural items that are not consistent with the definition of psychological recovery for example, ‘I have less than three people I consider my friends’ and ‘I go out and do at least two activities every week’. Instructions allow for an overall score, as well as subscale scores. Although based on Young and Ensing's [10] three phases, the literature provided with the measure does not refer to the apparent sequential relationship between the three phases and the six subscales.
Although both measures reflect aspects of the component processes, and the MHRM is associated with phases of recovery, it was concluded that there was a need for a measure with its foundations in the consumer definition of recovery and based on the stage model of recovery that can be used to assess the component processes as they occur within the five stages of recovery.
Development of the Stages of Recovery Instrument (STORI)
Generation of items
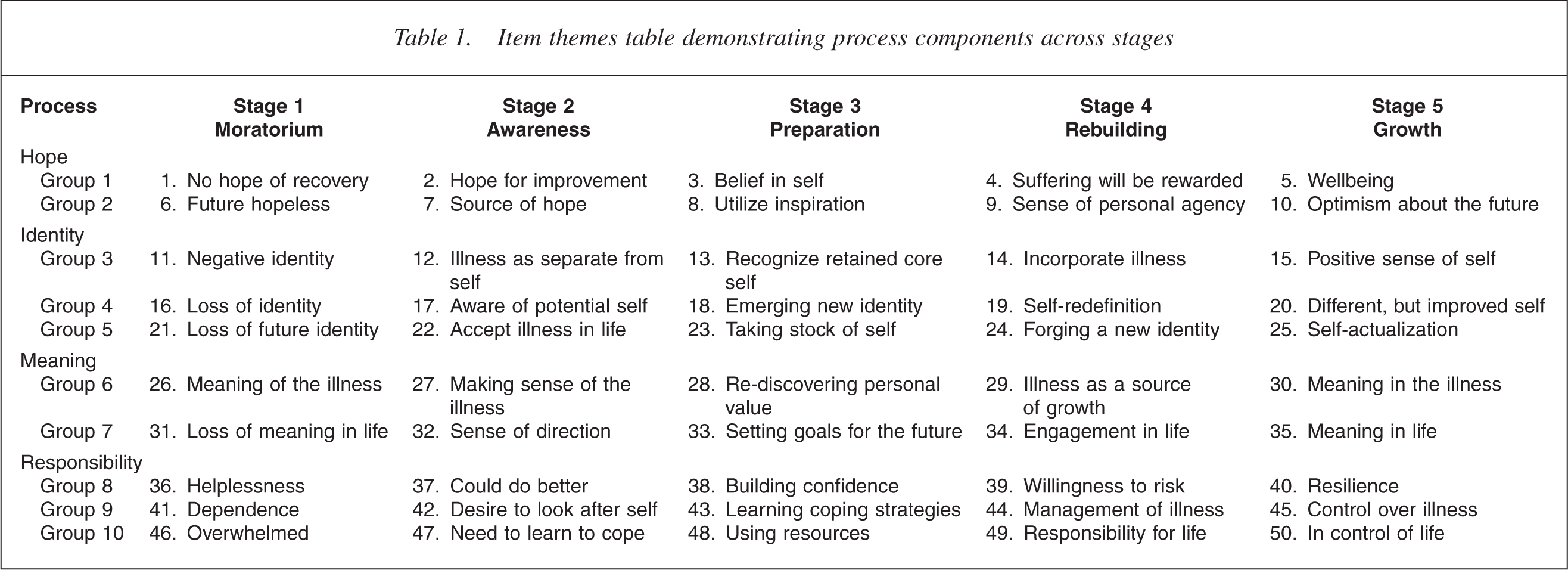
Using the stage model of recovery as a basis, the five studies which identified stages or phases of recovery 10– [14] were examined for concepts representing the four component processes: finding and maintaining hope reestablishment of a positive identity, finding meaning in life, and taking responsibility for one's life. In each study concepts relating to each process, if any, were identified for each stage. These concepts were then grouped under thematic subheadings. For example, for Stage 1, the process reestablishment of a positive identity was represented by three themes: loss of identity, negative sense of self and loss of positive future self. Ten themes were identified for each stage, and a number of items were generated to reflect each theme. The authors then agreed on 10 items to represent each of the five stages, resulting in a 50-item measure with five stage subscales. To compile the pilot measure, conceptually related items were presented in groups of five, comprising one item from each stage. This strategy was intended to encourage comparison of items from different stages, providing participants with some context when rating them. Participants were required to rate each item for ‘how much each statement is true of you now’ on a six-point scale ranging from ‘0’ = ‘Not true at all now’ to ‘5’ = ‘Completely true now’. This formed the draft version of STORI. The draft version of the STORI was piloted with six male and four female mental health consumer-researchers, ranging in age from 31 to 53 years. Six participants gave their diagnosis as schizophrenia, one as bipolar disorder, one as anxiety/depression and one as depression. Responses to the STORI provided quantitative data, and a feedback form and focus groups provided qualitative data.
Refinement of the STORI
Based on the results of the pilot, items were re-worded to stress that they represent current feelings or attitudes. For example, terms such as ‘I am Stage 1. I feel as though I don't know who I am any more. Stage 2. I have recently begun to recognize a part of me that is not affected by the illness. Stage 3. I am just starting to realize that I can still be a valuable person. Stage 4. I am learning new things about myself as I work towards recovery. Stage 5. I think that working to overcome the illness has made me a better person.
Table 1 shows the themes for the items and their groupings with numbers corresponding to the item number on the STORI. Finally, instructions were made more explicit regarding giving a lower rating to items that describe an experience already surpassed, and an example was included. The aim of the current research was to examine the validity of the STORI, first, as a measure of the recovery construct and second, as a measure of the stages of recovery as defined by the model.
Item themes table demonstrating process components across stages
Method
Participants
Approval for this research was obtained from the combined University of Wollongong and Illawarra Health Human Research Ethics Committee. Recruitment was conducted by the Neuroscience Institute of Schizophrenia and Allied Disorders (NISAD) that keeps the Schizophrenia Research Register, a database of people with schizophrenia who are interested in taking part in research. Recruitment to the Register is conducted via multimedia campaigns and through health and rehabilitation services [26]. Registrants' diagnoses are confirmed using a comprehensive structured assessment protocol. People on the Register were canvassed, and 104 agreed to participate by signing a return slip. This list of volunteers was then forwarded to the researchers. A package that included a description of the research, a consent form and a booklet of eight measures was mailed to each participant. A reply paid envelope was included, and participants were paid a nominal sum on return of the completed booklets. Ninety-four participants returned the completed booklets – a response rate of 90.38%.
Measures
The booklet contained the following measures:
Stages of Recovery Instrument (STORI): Fifty items, as described above, yielding five subscale scores of the stages of recovery. Recovery Assessment Scale (RAS) [22]: A continuous measure of recovery yielding a single score. This was chosen as a validity measure because it has published psychometric properties. Mental Health Inventory – five-item version (MHI-5) [27]: A short mental health screening test, utilizing those five items from the original Mental Health Inventory which best reproduce the results of the longer version. Psychological Well-Being Scales (PWB) [28]: Consists of six 7-item subscales: Autonomy, Environmental Mastery, Self Acceptance Positive Relationships, Personal Growth and Purpose in Life. Connor-Davidson Resilience Scale (CD-RISC) [29]: A 25-item measure of resilience. Adult State Hope Scale [30]: A six-item measure of Hope, consisting of Agency and Pathways subscales. Self-identified stage of recovery (SISR): Developed by the authors as a brief stage measure based on the stage model of recovery [8]. The SISR is single-item measure consisting of five statements each representing a stage of recovery. Respondents select the one statement that best describes his or her current experience of recovery. The SISR has been shown to correlate with the client-rated RAS (r = 0.45, p < 0.05) and Kessler-10 (r = −0.32, p < 0.05), and with the clinician-rated Health of a Nation Outcome Scales (r = −0.39, p < 0.05) [31]. The Kessler-10 is a 10-item self-report measure of psychological distress, assessing symptoms of depression and anxiety [32]. The Health of a Nation Outcome Scale [33] is a 12-item measure of severity of psychiatric symptoms. Both measures have been introduced as mandatory mental health outcome measures in New South Wales, Australia. Demographic information: Age, diagnosis, age at first diagnosis time since last hospitalization, length of stay, level of education occupation and accommodation circumstances.
Acceptable reliability and validity for the RAS, MHI-5, PWB, CDRISC and the Adult State Hope Scale have been reported in the relevant literature cited above.
Results
Demographics
Participants were 45 men and 49 women, ranging in age from 19 to 76 years (M = 44.13, SD = 12.59). Eighty-seven identified English as their first language. Fifty-one participants had been tested by NISAD. Of those, 45 were given a diagnosis of schizophrenia, and an additional 40 self-reported schizophrenia, a total of 85. Other diagnoses were schizoaffective disorder (n = 2), bipolar disorder (n = 1) and other psychotic disorders (n = 5). Data were missing for one participant. The duration of illness from first diagnosis ranged from less than 1 year to 45 years (M = 18.23, SD = 11.24). Time elapsed since last hospitalization ranged from less than 1 year to 38 years (M = 7.51, SD = 8.29) with seven participants reporting no inpatient treatment. Sixty-four reported living independently, 27 living with supportive family or in supported accommodation, one was in hospital, and two had missing data. Twenty-six reported a university education, and a further 33 had graduated from high school or had technical qualifications.
Data were analysed to establish (i) preliminary validation of the STORI as a measure of patient-orientated recovery; and (ii) preliminary validation of the STORI of a measure of the stages of recovery as defined by the model.
Validation of the STORI as a measure of recovery
Stage allocation
Stage of recovery (STORI stage) was determined based on each participant's highest mean score on the five stage subscales. When scores on two subscales were tied, the person was allocated to the higher stage. Using this method, 10 participants were allocated to a higher stage – seven of these were allocated to Stage 5. Forty-eight participants were allocated to Stage 5, 30 to Stage 4, five to Stage 3 two to Stage 2 and eight to Stage 1. To test the validity of stage allocation, STORI Stage and self-identified stage of recovery were compared. The SISR resulted in 32 people being allocated to Stage 5 34 to Stage 4, 13 to Stage 3, six to Stage 2 and seven to Stage 1. Data were checked for violations of normality, and although slightly skewed did not warrant the use of non-parametric tests. The two measures were correlated (r = 0.58, p < 0.01), and agreement as tested with Cohen's kappa was 0.27 (p < 0.001) with 50% agreement. Although the kappa was quite low, we proceeded with further exploration of the properties of the STORI.
There was no significant correlation of STORI stage with age, duration since diagnosis, length of last hospital stay or age at onset. There was, however, a correlation with time elapsed since last inpatient treatment (r = 0.22, p < 0.05). There was no significant difference in STORI stage between groups based on gender or country of birth. However, a significant difference was found between education levels with people who had a level of education at Associate Diploma or higher showing a higher level of recovery (Mann–Whitney U = 590.50, p < 0.05).
Concurrent validity of stage allocations
Pearson correlations between STORI stage and all other measures were highly significant and ranged from r = 0.52 (p < 0.01) with the RAS to r = 0.62 (p < 0.01) with the PWB total scale, indicating that overall scores on the STORI are a valid measure of the recovery construct.
Internal consistency of the stage subscale scores
Since the STORI is made up of five separate subscales, Cronbach's coefficient alpha was calculated for each one. All returned high alpha values (from 〈 = 0.88 [Stage 4] to 〈 = 0.94 [Stage 3]), demonstrating high reliability of the individual subscales.
Concurrent validity of subscale scores
A distinct pattern of correlations between the stage subscale scores and the other measures emerged (see Table 2). There was a strong negative correlation between the other variables and Stage 1 mean scores (r = −0.44 to −0.68, p < 0.01), correlations with Stage 2 were all negative but mostly non-significant, and there were no significant correlations with Stage 3. Conversely, there were strong positive correlations with Stage 5 scores (r = 0.53–0.79, p < 0.01), and Stage 4 scores tended to be positive, but weaker or non-significant. These results suggest that the intermediate subscales of the STORI are measuring stage-related variables not present in the other measures.
Correlations between STORI subscales and other variables
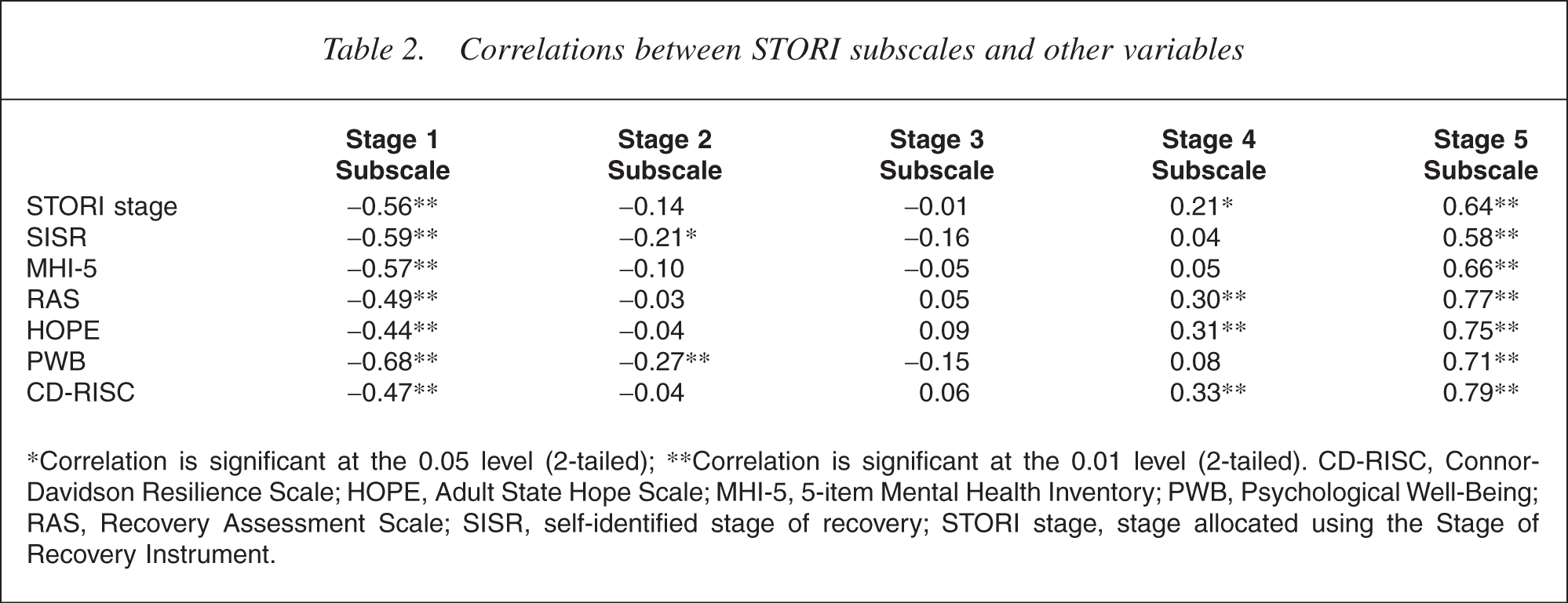
∗Correlation is significant at the 0.05 level (2-tailed); ∗∗Correlation is significant at the 0.01 level (2-tailed). CD-RISC, Connor-Davidson Resilience Scale; HOPE, Adult State Hope Scale; MHI-5, 5-item Mental Health Inventory; PWB, Psychological Well-Being; RAS, Recovery Assessment Scale; SISR, self-identified stage of recovery; STORI stage, stage allocated using the Stage of Recovery Instrument.
Validity of the stage subscales of the STORI
Construct validity of the five stage subscales
If the five stage subscales of the STORI are valid, then an ordinal relationship would be expected between the subscale scores. Pearson correlations between the five subscales are shown in Table 3. As expected adjacent stages correlate positively, the most distant stages correlate negatively while other relationships are weaker or non-significant. This pattern can be observed most clearly in Stages 1 and 5. The mean subscale scores increase as stage level increases, which reflects the finding that most respondents are in Stages 4 and 5 (See Table 3).
Means, standard deviations and intercorrelations of stage subscales
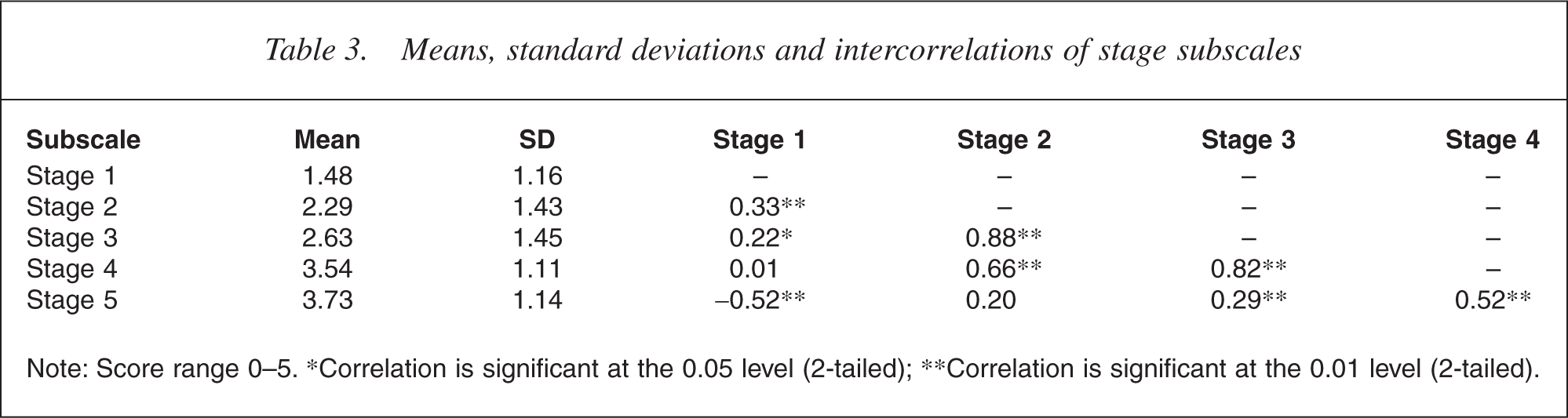
Note: Score range 0–5. ∗Correlation is significant at the 0.05 level (2-tailed); ∗∗Correlation is significant at the 0.01 level (2-tailed).
Structure of the measure
Hierarchical cluster analysis using Ward's Method was performed to determine whether the STORI items clustered into groups representing the stages of recovery. Based on the dendrogram, a three-cluster solution was the clearest result: Cluster 1 (10 items) consisted of all Stage 1 items. Cluster 2 (24 items) consisted of all Stage 2 items, all Stage 3 items plus four Stage 4 items. Cluster 3 (16 items) consisted of all Stage 5 items plus six Stage 4 items.
The Stage 4 items that loaded on Cluster 2 were items 9, 14, 24 and 49. Those loading on Cluster 3 were items 4, 19, 29, 34, 39 and 44 (see Table 1 for item themes). Coefficient alpha was calculated for each cluster, and indicated very high reliability (Cluster 1, 〈 = 0.88; Cluster 2, 〈 = 0.97 and Cluster 3, 〈 = 0.92). This analysis failed to produce the expected five clusters, indicating that the items do not discriminate sufficiently between stages.
Concurrent validity of the three clusters
Correlations of the clusters with STORI stage and the other measures (see Table 4) repeated the pattern of correlations shown by the mean stage scores. Cluster 1 had strong negative correlations with all other variables, while Cluster 3 showed strong positive correlations.
Correlations between the item clusters and the other variables
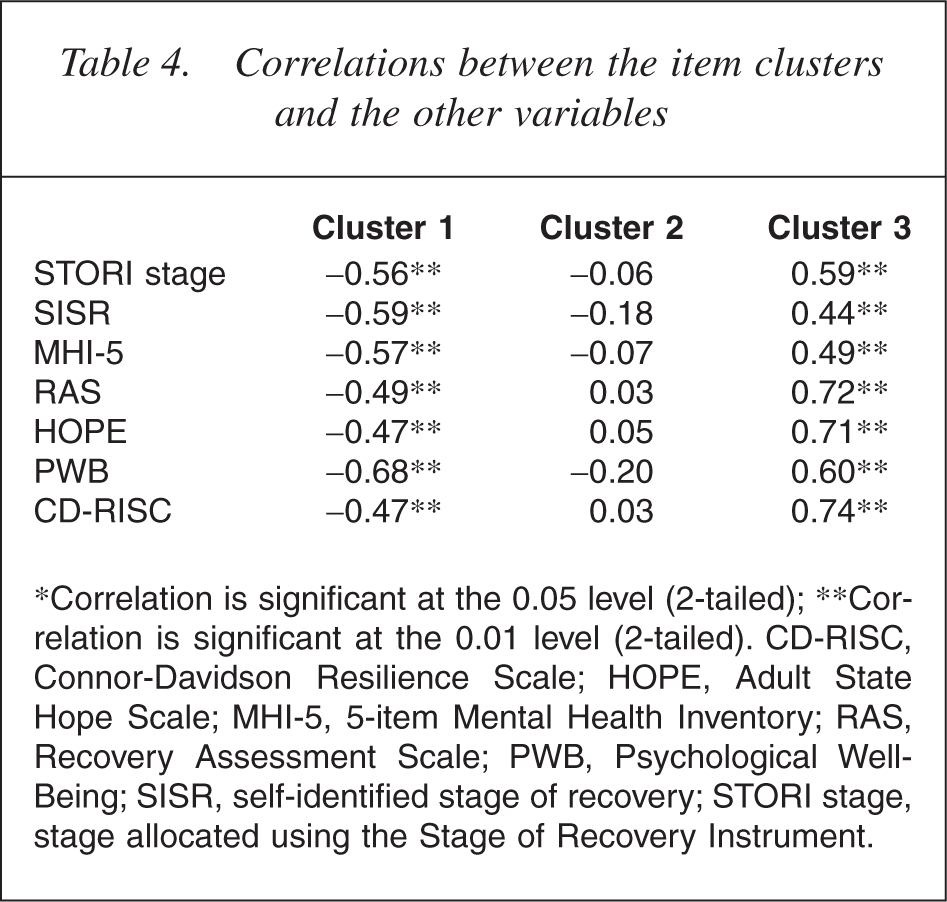
∗Correlation is significant at the 0.05 level (2-tailed); ∗∗Correlation is significant at the 0.01 level (2-tailed). CD-RISC, Connor-Davidson Resilience Scale; HOPE, Adult State Hope Scale; MHI-5, 5-item Mental Health Inventory; RAS, Recovery Assessment Scale; PWB, Psychological Well-Being; SISR, self-identified stage of recovery; STORI stage, stage allocated using the Stage of Recovery Instrument.
Cluster 2 correlations were in either direction, and always nonsignificant thus supporting the construct validity of three clusterbased stages.
Relationship between the three item clusters
Cluster 2 correlated positively with both Cluster 1 (r = 0.26, p < 0.05) and Cluster 3 (r = 0.42, p < 0.01), while Cluster 1 and 3 were negatively correlated (r = −0.40, p < 0.01). This pattern of correlations supports the ordinal nature of the clusters.
Discussion
In order to test the stage model of recovery [8], it is first necessary to develop and validate a measure that reflects the model. Positive correlations between STORIallocated stage and other recovery-related measures demonstrate its validity as a measure of the patient-orientated recovery construct. Individual stage subscales were found to be internally consistent, indicating that items within each subscale reliably measure the same construct. There was a distinctive pattern of correlations between the stage subscales and the other measures: Stage 1 had strong negative correlations with the other variables, Stage 2 had weak negative correlations, Stage 3 had non-significant correlations in both directions Stage 4 had weak positive correlations, and Stage 5 had strong positive correlations. Therefore, people who scored higher on the Stage 1 items, scored lower on the other measures of mental health, and those who scored higher on the Stage 5 items scored higher on the other measures, and so on. This supports the concept that the content of the intermediate stage subscales (Stages 2–4) is qualitatively different to the continuous measures of health, wellbeing and recovery, and offers preliminary support for the STORI as a measure of stages of psychological recovery.
In addition, this pattern of correlations supports the ordinal nature of the stage subscales, which was further indicated by the direction and magnitude of the intercorrelations between the individual subscales. That is, the most distal stages were highly negatively correlated with each other and adjacent stages were highly positively correlated, while the intermediate relationships were weaker, and in the expected directions. These results support the construct validity of the ordinal stages of the STORI. However, further analysis highlighted the complexity of the task of measuring recovery.
A cluster analysis of the STORI items produced only three stage-related clusters, instead of the expected five. This could indicate either of two things: recovery takes place in only three stages rather than five; or, there are five stages to recovery, but the STORI does not clearly discriminate between them. The five stages of the model are based on a synthesis of the findings of a number of independent qualitative studies that, although different in content, show parallels in their description of steps stages or phases in recovery. In synthesizing these findings it is possible that we determined an incorrect number of stages. However, there is another issue to be considered regarding psychological stage models in general. Using the Transtheoretical Model [e.g. [34] as an example, Smedslund [35] has argued that smoking cessation can be described as having only two behavioural stages: smoking and non-smoking. However, there are a series of internal processes that represent psychological stages in the change process, and these stages are defined by the researcher [35]. Smedslund explains that, although the stages may not be validated in research, this can be a fault of the instrument, or due to the inability of participants to distinguish between the stages as defined [35]. Similarly, our model describes changes in four psychological component processes over five logically sequential stages, resulting in the STORI being a complex measure. Although the stages were derived from qualitative research with patients, participants may be unable to discern the subtle differences between items. As well, people may be drawn to items that they have experienced, and readily endorse them even though they have now surpassed that stage. Therefore, the wording and presentation of the items need to be reviewed.
The complexity of the measure will also impact on discrimination between stages, as the competing elements of stage and component process may affect the outcome of the cluster analysis: it is possible that movement through the component processes of recovery does not occur in parallel across the stages. Although we attempted to generate items for each process that reflected the qualitative findings for each stage, it is possible that, say, the Stage 2 themes for hope occur before those for responsibility (refer to Table 1), creating an overlap in the measurement of the stages. Although the relationships between the stage subscales support the notion that recovery is a process that takes place in steps or stages, the cluster analysis indicates that the measure is not sufficiently sensitive to qualitative differences between the stages. The pattern of the component processes across the stages is therefore an important area for future research. Of course, the possibility that there are not five distinct stages to recovery is in need of further investigation. However, since the five-stage model of recovery has a sound basis in qualitative research, we believe that efforts should first be directed towards enhancing the power of the STORI to discriminate between the stages of the model. It could then be used in comprehensive testing of the five-stage model using prospective longitudinal methods and the inclusion of objective measures.
Our analyses were limited by the small numbers in the early stages of recovery. The sample consisted entirely of registered volunteers who are likely to be at a later stage of recovery [26]. Although there was variation in terms of age and duration of illness, the inclusion of participants from a clinical population should provide greater variability in the data.
In summary, the results provide preliminary empirical support for the STORI as a measure of the patient experience of recovery. However, in its present form it does not sufficiently discriminate between the five stages as defined by the model. Detailed item analysis and refinement of the STORI is in progress to address this problem. Once the STORI can capture the five stages as defined the five-stage model can be tested using prospective longitudinal methods. Recovery is a multidimensional and highly individual journey, which the stage model of recovery attempts to describe in a parsimonious model that nevertheless accommodates the individuality of the experience. The model has already proven valuable in clinical training, and may provide a useful heuristic for clinical work and a framework for research. A single relatively short measure capturing this complex construct would prove invaluable. The findings serve to highlight the complexity of the task of operationalizing recovery and validating the consumer-orientated model – the next important step in advancing recovery-orientated research and practice.
Footnotes
Acknowledgements
This work was supported by NISAD, utilizing infrastructure funding from NSW Health, and the Illawarra Institute for Mental Health. The research is an associated project of the National Mental Health and Medical Research Council Strategic Partnership Grant in Mental Health (#219327). The authors would like to thank the NISAD Schizophrenia Research Register, Australia, for assisting with the recruitment of participants. We would also like to thank Professor David Kavanagh and Professor Frank Deane for their comments on the manuscript.