
Abstract
Objective:
Caring for someone with serious mental illness such as schizophrenia or bipolar disorder can result in considerable consequences for the caregiver. Carers often experience a range of negative emotions, impacts upon their physical and mental health, as well as financial strain. Resultant from these impacts, carers utilise medical services at a higher rate than their non-caregiving counterparts. Further, these consequences of caregiving can also impact upon the patient, resulting in an increase in psychopathology and relapse. Although the notion of burden has been studied for approximately 60 years, many flaws and inadequacies remain; most notably, a lack of agreement on the definition of the construct along with the poor psychometric properties of the burden assessment instruments.
Method:
This article reviews and evaluates the measures of burden of care that have been utilised with carers of people with a serious mental illness. A systematic search was conducted and all articles that had measured burden of care in schizophrenia or bipolar disorder in the database PUBMED were reviewed to ascertain the measure utilised.
Results:
Ten different measures were subsequently identified and eight were reviewed; two were excluded on the basis that they had only been utilised once.
Conclusions:
It was apparent that many of the measures lacked a strong theoretical basis and sound psychometric properties. Further, some of the measures lacked utility, feasibility and specificity. The article concludes with recommendations for future research.
Introduction
As a result of de-institutionalisation over the last 60 years, the vast majority of care for people with a serious mental illness (SMI), specifically schizophrenia spectrum disorders and bipolar disorder, now resides with informal caregivers (Harvey et al., 2008). This move to a community-based care model for people with SMI has practically formalised the role of informal caregivers in providing care to this population (Awad and Voruganti, 2008). These informal caregivers, families, partners and friends make an important and vital contribution to the care of people with SMI (Schulze and Rossler, 2005). However, unfortunately, this role of caregiving can have a detrimental impact upon their lives and well-being.
The nature of caring for someone with SMI, specifically schizophrenia or bipolar disorder, can result in considerable consequences for the caregiver (Van Wijngaarden et al., 2000). The study of the consequences that are resultant from caring for people with SMI began following the advent of de-institutionalisation (Awad and Voruganti, 2008). This impact of caregiving has been conceptualised as family burden.
However, Schene et al. (1994) ascertain that the term ‘family burden’ is a misnomer as burden is generally evaluated through the primary caregiver as opposed to the family unit. Thus, the terms ‘burden of care’ and ‘family burden’ have been used synonymously. The term burden collectively refers to the social, psychological, behavioural, functional, medical and economic consequences of caregiving (Awad and Voruganti, 2008). Burden in this article is conceptualised as the aforementioned broad consequences of providing care to an individual and not in accordance with the World Health Organization’s global burden of disease disability-adjusted life year index (World Health Organization, 2008).
The construct of caregiver burden has been widely investigated in numerous populations, not just in carers of people with SMI (Gallagher et al., 2008; McCann et al., 2012; Pinquart and Sorensen, 2011; Wagner et al., 2011). Specifically, the gerontological literature has been reporting the burden associated with the care of a person with Alzheimer’s disease or dementia for decades (Pinquart and Sorensen, 2011), with these two diseases often being included in the category of SMI.
The consequences of caregiving or burden of care has also been found to impact upon parents of children with a physical or intellectual disability (Gallagher et al., 2008; McCann et al., 2012). Further caregiver burden has also been found to be evident in the spouses of patients being treated for cancer (Wagner et al., 2011). Thus, the impact of caregiving is not limited to carers of individuals with SMI – specifically schizophrenia and bipolar disorder (Gallagher et al., 2008; McCann et al., 2012; Pinquart and Sorensen, 2011; Van Wijngaarden et al., 2000; Wagner et al., 2011).
Schizophrenia and bipolar spectrum disorders are serious and debilitating mental disorders with considerable psychosocial consequences and high rates of mortality (Capuano et al., 2002; Merikangas et al., 2007). Schizophrenia spectrum disorders afflict approximately 1% of the population worldwide (Capuano et al., 2002). Similarly, bipolar spectrum disorders have a comparable prevalence rate, with bipolar I and bipolar II having a prevalence rate of 0.8% and 1.1%, respectively (Merikangas et al., 2007). However, Zimmerman et al. (2011) recently contended that current prevalence rates are underestimated due to diagnostic issues. People with schizophrenia and bipolar disorder require considerable amounts of care and support, and also exhibit challenging behaviours at times. These factors can significantly impact upon the level of burden felt by caregivers and their families (Awad and Voruganti, 2008; Harvey et al., 2008; Schulze and Rossler, 2005).
Historically, the concept of burden of care has been postulated to be comprised of two distinctive components: objective burden and subjective burden (Hoenig and Hamilton, 1966). The notion of objective burden pertains to the concrete effects of providing care to a loved one; for instance, the financial repercussions and the effects upon the carers’ health (Hoenig and Hamilton, 1966). The other theorised component of burden, subjective burden, concerns the perceived burden of care experienced by carers (Hoenig and Hamilton, 1966). That is, the burden of care is commonly conceptualised as a multi-faceted construct that is measured through a number of domains.
Although the construct of burden has been scrutinised for approximately the last 60 years since de-institutionalisation; flaws and inadequacies remain (Awad and Voruganti, 2008; Schulze and Rossler, 2005). Most notably there is not an agreed upon definition or an established robust measure of the construct (Awad and Voruganti, 2008; Schulze and Rossler, 2005), with researchers theoretically defining (if they offer a theoretical definition) and operationalising burden differently. Further, the majority of the measures that exist to measure burden lack psychometric rigour, with a surprising number not even being subjected to exploratory factor-analytic procedures (Harvey et al., 2008; Madianos et al., 2004; Schulze and Rossler, 2005).
Few researchers have postulated the theoretical foundations of the burden construct. Moreover, recently, even the use of the term ‘burden’ has been questioned as researchers and theorists begin to realise that caregiving not only has negative consequences, as implied by the notion of burden, but that caregiving can also result in positive outcomes and emotions for the carer (Moller et al., 2009; Szmukler et al., 1996; Tarricone et al., 2006; Treasure et al., 2001).
Researchers who have proposed theoretical models of caregiving have moved away from the notion of burden or the negative experience of caregiving alone and embraced a holistic view of the experience of caregiving. As highlighted above, they have incorporated the positive experiences as well as the negative experiences of providing care to someone with a SMI (Moller et al., 2009; Szmukler et al., 1996; Tarricone et al., 2006; Treasure et al., 2001).
These cognitive models of caregiving are based upon a cognitive appraisal framework. Szmukler and colleagues (1996) proposed that the experience of caregiving results from an interaction between an appraisal of stressors: the ill person’s illness severity, the ill person’s behaviours and level of disability, as well as factors in the carer’s internal and external world. These appraisals of stressors interact with the carer’s coping strategies, engendering the carer’s experience of caregiving (Szmukler et al., 1996; Treasure et al., 2001).
Similarly, Kuipers and Onwumere (2010) recently formulated a model of caregiving in psychosis based upon cognitive appraisals. The model postulates that the dyad’s original relationship and the carer’s appraisals (of the individual’s behaviour and illness) affect the carer’s behaviour towards the individual being cared for. This relationship is mediated by the cognitive and affective reactions of the caregiver. However, the focus of this review remains on the measurement of burden – the negative objective and subjective consequences of providing care to someone with a SMI.
In an early review of burden of care, Schene and colleagues (1994) concluded that although interest in the field had grown in the 10 years that their review spanned, they feared the field would become fragmented owing to the utilisation of too many measures. This would be to the detriment of a few standard instruments measuring burden of care in SMI which could facilitate comparison across studies. They urged researchers to develop and validate measures that could be utilised in both research and clinical practice.
Similarly, a later review by Schene and colleagues (2001) identified 20 measures that were being utilised. They concluded that the field required standardised instruments to aid in the further development of knowledge in the area. Schulze and Rossler (2005) conducted a review of the literature investigating the measures that were used to assess burden of care in SMI between 2004 and 2005: it was apparent that there were more than 20 different measures being utilised.
However, Schulze and Rossler (2005) included dementia and Alzheimer’s disease in their operational definition of SMI. They found that two-thirds of the studies conducted within that period investigated caregiver burden in dementia and Alzheimer’s disease; thus displaying the dearth of knowledge that exists in relation to the measurement of burden of care in SMI operationalised as schizophrenia and bipolar disorder.
Furthermore, it can be argued that burden of care is both qualitatively and quantitatively different between the demented disorders and the serious mental illnesses of schizophrenia and bipolar disorder (Magliano et al., 2005; Moller et al., 2009; Nehra et al., 2005). One conspicuous issue pertains to the longevity of care required for the latter mental illnesses, which typically develop in late adolescence or early adulthood and generally require lifelong care (Magliano et al., 2005; Nehra et al., 2005). This temporal effect would have a further cumulative impact upon the burden of care for this population. These mental illnesses are quite distinctive so it may not be appropriate to measure burden of care with the same instruments – as the carers are experiencing different issues.
Recently, Harvey and colleagues (2008) conducted a review of instruments used to assess outcomes in carers of people with mental illness, finding over 200 instruments for measuring different outcome variables (burden, well-being, quality of life, etc.). From their review they ascertained that measures exist to measure the most fundamental carer outcomes; however, all of the measures required further work and validation.
It is apparent from the review articles discussed that the measurement of caregiver burden in SMI requires further evolution (Harvey et al., 2008; Schene et al., 1994, 2001; Schulze and Rossler, 2005). Notably, similar conclusions were made by the early and most recent review articles – pertaining to the measurement of burden of care. Further, Schulze and Rossler’s review included the demented disorders in their operational definition of SMI, while Harvey and colleagues’ review focused on carer outcomes in general and not specifically upon burden of care in SMI. Therefore, the primary aim of this article is to review the instruments that have been utilised to measure burden of care in carers of people with SMI (limiting SMI to schizophrenia and bipolar spectrum disorders). The focus of this review will be upon how the construct of burden is conceptually defined and operationalised in each of the measures to ascertain a clearer conceptual definition of the burden construct. Further, the psychometric properties of each of the instruments will be assessed through reviewing: specificity (how specific they are to an SMI caregiver population); utility (how useful they are in research and clinical practice); and feasibility (how practical they are). This will provide a broad qualitative review of the instruments that are currently being utilised to assess burden of care in SMI and will assist researchers and practitioners alike in determining the appropriate instrument for measuring this important construct, while also assisting with the further development and refinement of the construct.
Methodology
A systematic search of the electronic database PUBMED Central was conducted in order to locate a representative sample of research that has measured burden of care in caregivers of people with SMI (schizophrenia and bipolar disorder). Only one database was utilised as the aim of the search was to obtain a sample of literature measuring burden of care in SMI with previously published and utilised quantitative measures of burden of care.
Figure 1 depicts the search procedure. From the original 325 articles located, 274 were excluded as they did not utilise a quantitative measure of burden of care. The methodology of the remaining 51 articles was further evaluated and articles that utilised scales not available in English or full text versions were excluded. The instrument used to measure burden in the remaining 34 articles, which spanned the years 1992–2011, was recorded.
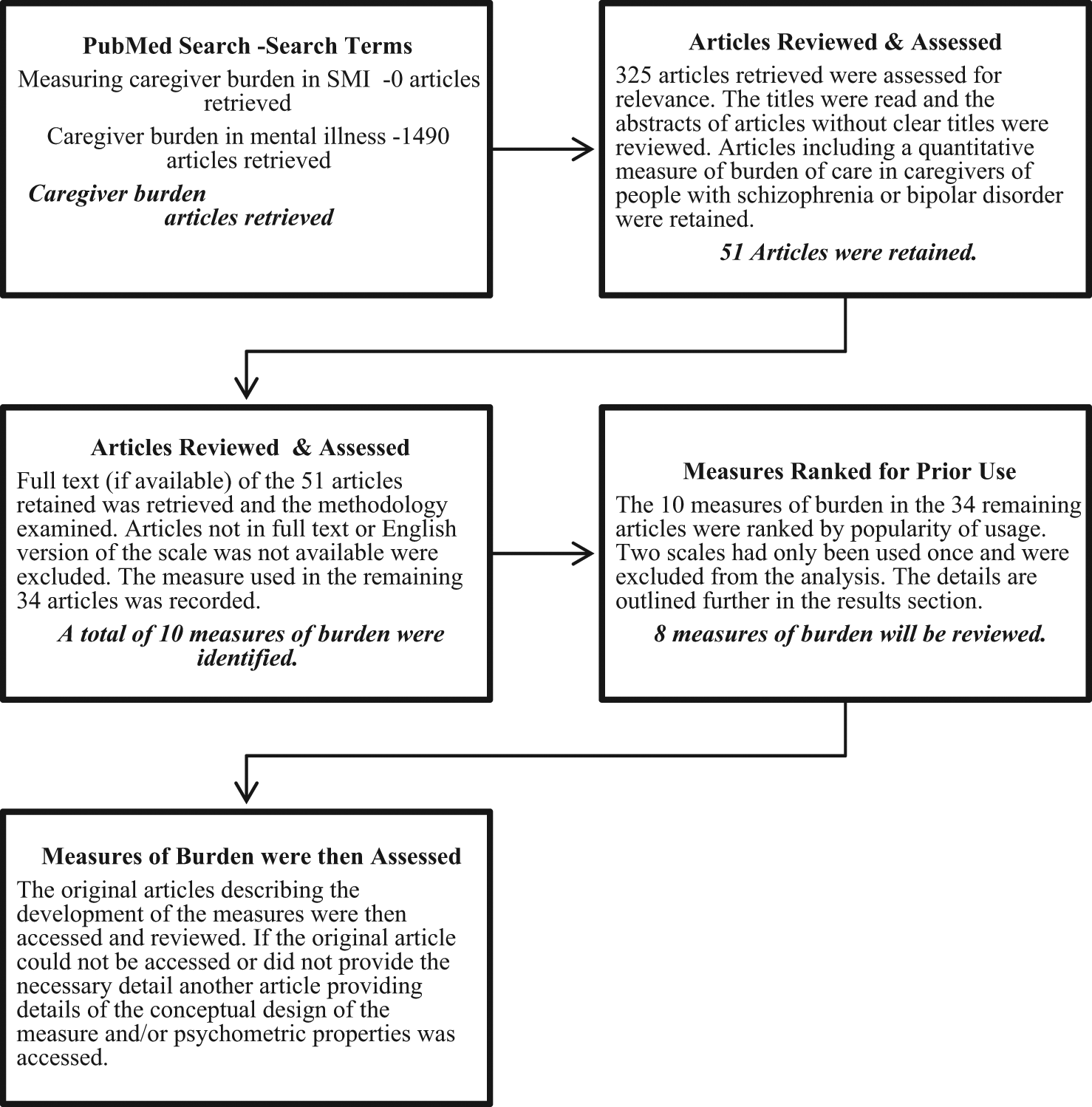
Overview of the search procedure.
Results
The aforementioned search strategy yielded a total of 34 articles that assessed burden of care in SMI. From these articles it was found that 10 different measures of burden were utilised (two measures were excluded; see below). Table 1 lists the 10 measures of burden of care in chronological order of development; the scales that will be reviewed appear in bold font.
Measures of burden of care.
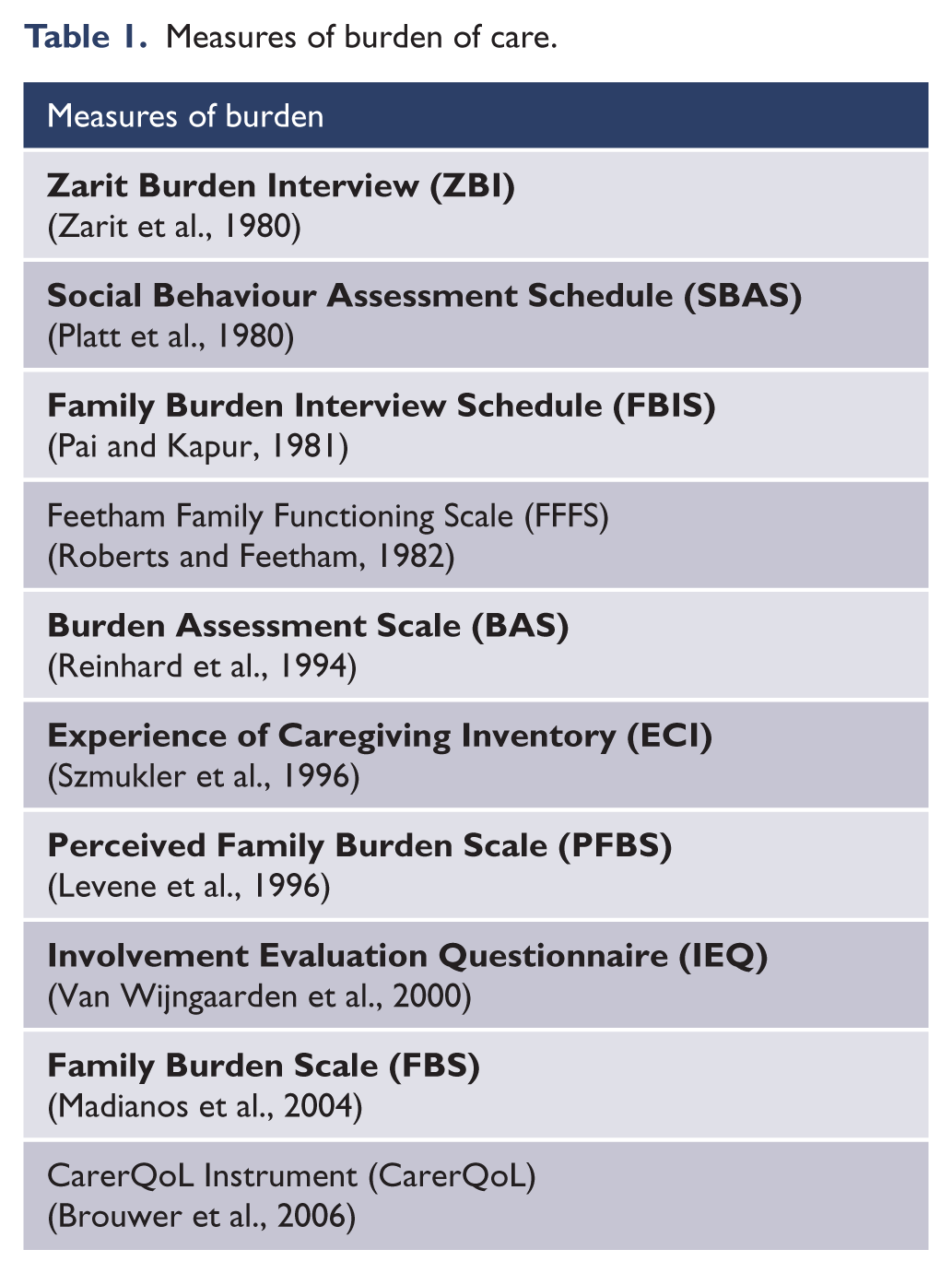
Figure 2 displays the proportion of use of each of the measures that will be reviewed from the remaining 32 articles. Note that the reduction from 34 occurred owing to two scales (Brouwer et al., 2006; Roberts and Feetham, 1982) being excluded as they were only used once in the sample of articles identified. The Zarit Burden Interview (ZBI) has been used the most followed by the Experience of Caregiving Inventory (ECI), Burden Assessment Scale (BAS) and Family Burden Interview Schedule (FBIS), with the remaining four being utilised less frequently. The number of times each scale was utilised is listed in Table 2.
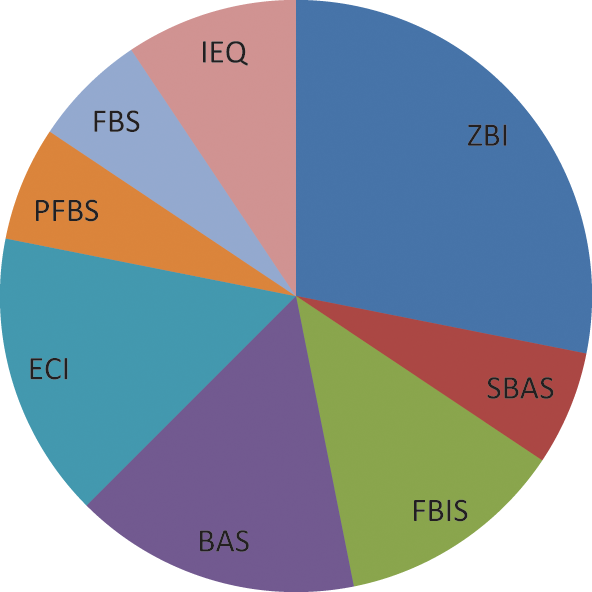
Use of burden of care measures.
Frequency of use of measures of burden of care.
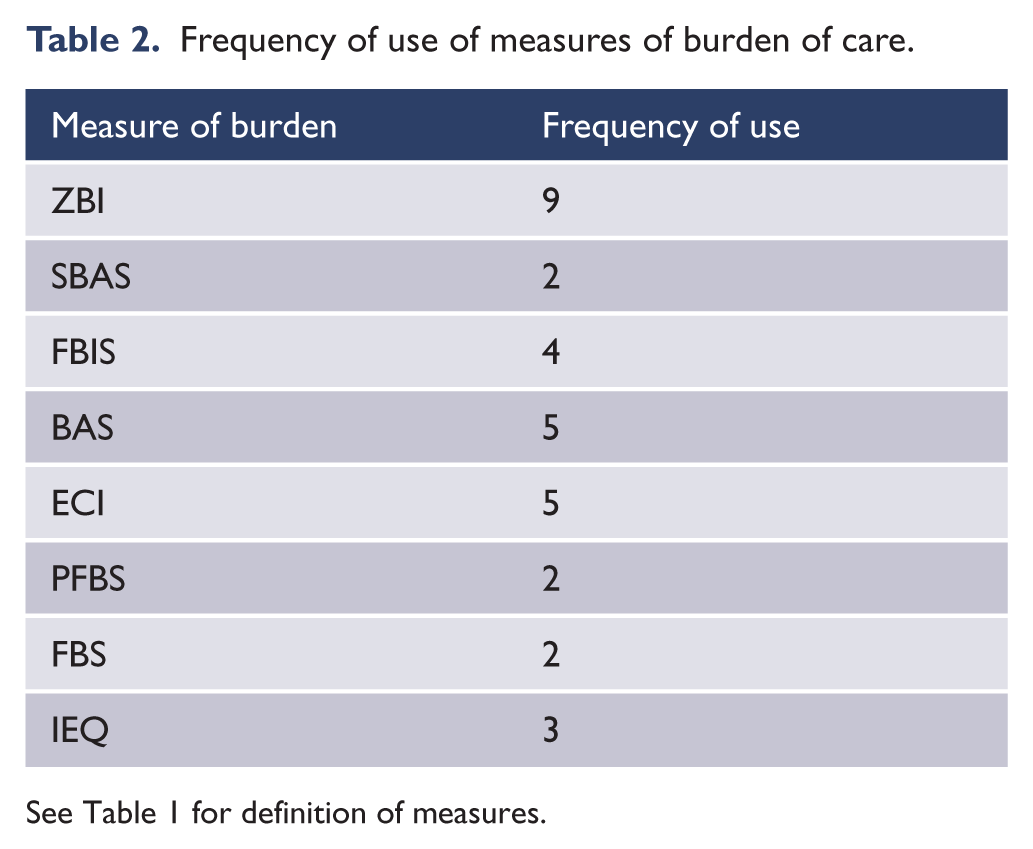
See Table 1 for definition of measures.
The majority of the articles reviewed assessed burden of care in schizophrenia (22/32 articles), while a mix of affective and psychotic disorders (not specified) was the next highest category (five of the 32 articles). Next was bipolar and first-episode psychosis (three and two of 32 articles, respectively).
Table 3 summarises the characteristics and properties of the measures that are reviewed below. Each of the measures will be reviewed with a focus upon the definition of burden, how it is operationalised, as well as the population in which the measure was designed to assess burden. This review will facilitate information pertaining to the specificity, utility and feasibility of each of the measures of burden of care for use in research and clinical practice.
Summary of burden measures.
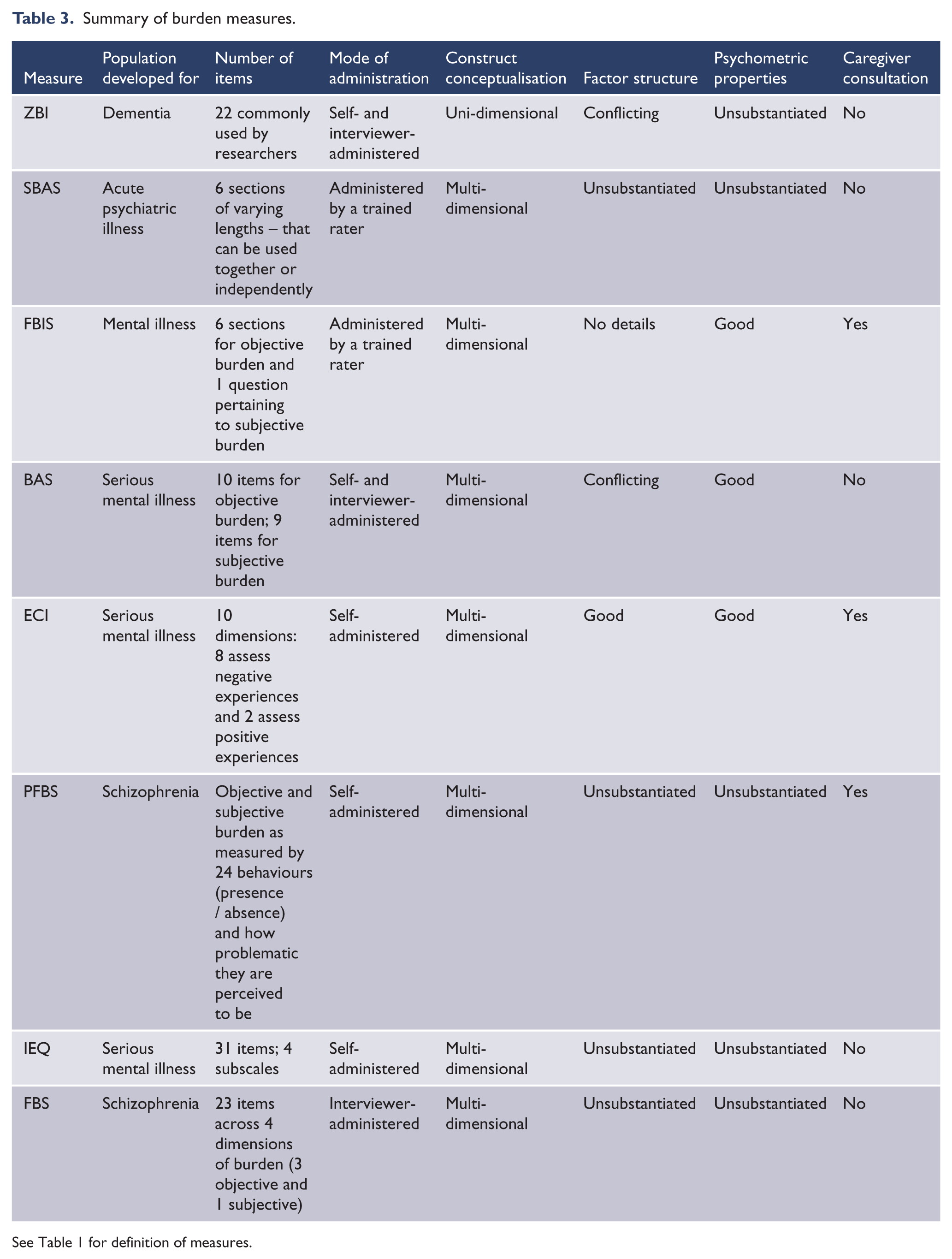
See Table 1 for definition of measures.
Zarit Burden Interview (ZBI)
The ZBI, developed by Zarit, Reever and Bach-Peterson (1980) was originally developed to test the burden of care for people caring for an individual with dementia. The ZBI was originally a 29-item self-report inventory which is administered via an interview with the primary caregiver; later, Zarit, Todd and Zarit (1986) reduced the ZBI to 20 items. Commonly in contemporary research, the ZBI is comprised of 22 items and is self-administered or administered via interview (Knight et al., 2000; Schreiner et al., 2006). The ZBI is one of the most commonly utilised measures of caregiver burden (Knight et al., 2000; Schreiner et al., 2006).
The ZBI was developed from clinical experience and prior empirical research (Szmukler et al., 1996; Zarit et al., 1986). The ZBI defines burden as ‘the extent to which caregivers perceived their emotional or physical health, social life, and financial status as suffering as a result of caring for their relative’ (Zarit et al., 1986: 261). Although the burden of care is generally conceptualised as a multi-dimensional construct, the ZBI measures burden as a uni-dimensional concept (Knight et al., 2000; Schreiner et al., 2006). The ZBI provides a global score of caregiver subjective burden, with higher scores indicating greater subjective burden of care (Knight et al., 2000; Schreiner et al., 2006).
The ZBI has been reported to have high levels of internal consistency, which is generally indicative of a uni-dimensional construct (Knight et al., 2000). However, results pertaining to the factor-analytic structure of the ZBI are conflicting, with both two- and three-factor structures being reported in prior literature; details of the analyses were not reported (Hassinger, 1986; Whitlach et al., 1991). More recently, Knight et al. (2000) identified three subscales of the ZBI through both exploratory and confirmatory factor-analytic techniques. They termed these subscales as being anger/embarrassment and the patient’s dependency and self-criticism. This inconsistency in the results of factor-analytic studies, coupled with the global score of caregiver burden the ZBI generates, consequentially results in the construct validity of burden as measured by the ZBI as being questionable. Further, Harvey and colleagues (2008), in a recent review, demonstrated that the ZBI has been utilised extensively, more than any other measure of burden. However, there are not enough data available to accurately assess the fundamental psychometric properties (reliability and validity) of the inventory.
Social Behaviour Assessment Schedule (SBAS)
The SBAS was developed by Platt and colleagues (1980) as there was no single measure at the time that assessed a patient’s disturbed behaviour and a patient’s social (or role) performance as well as the impact upon the household and the primary caregivers. Further, it was constructed to assess change over time as a result of an independent variable (e.g. treatment program, relapse etc.). Platt and colleagues (1980: 45) reported that ‘the schedule is particularly appropriate for the assessment of the burden of acute psychiatric illness’.
The SBAS is comprised of six sections with three sections (2, 3 and 4) forming the core of the SBAS and three sections (1, 5 and 6) providing background and contextual information to interpret the results within the milieu of the family. Each of the six sections can be used independently, depending upon the research agenda. SBAS can only be administered via interview by a trained rater and takes approximately 45–75 minutes to complete (Platt et al., 1980).
The three sections (2, 3 and 4) that comprise the core of the SBAS are a patient’s disturbing behaviours, a patient’s social (or role) performance, and adverse effects on others, respectively (Platt et al., 1980).
Section 2 (a patient’s disturbing behaviours) is composed of 22 of the most inconvenient and disrupting behaviours evident in people with SMI (Platt et al., 1980). Each of the behaviours is rated objectively for the frequency of occurrence and subjectively for how distressing the carer rates the behaviour and how long it has been occurring for.
Section 3 (a patient’s social performance) assesses the patient’s instrumental behaviours. Namely, domestic role performance, parental role performance, spare time activities, carer–patient relationship, sexual relationship, work and/or study, along with an additional measure indicative of higher performance: a patient’s participation in decision making (Platt et al., 1980).
This measure does not take into account gender, age or culture in determining role performance. Rather, the interpreter of the results decides whether or not role functioning is impaired based upon the above demographic variables (Platt et al., 1980). This section is rated on four scales: objective role participation, change in participation from ‘best ever’ role functioning, distress of carer due to patient’s impairment in role functioning and, finally, the onset of change in role functioning (Platt et al., 1980).
Section 4 measures the adverse effects on others around the patient – specifically the objective consequences of the problems caused by the patient for the caregiver and household, and how much distress they attribute to each. This section specifically measures the impact on school-aged children, the impact on the primary caregiver and the household, and relationships within the household. There is also an additional measure of the disruption of the life of others (Platt et al., 1980). Each of the subsections is measured on four scales, namely: objectively for occurrence, resulting distress, onset of the problem/issue, and how related the issue is to the patient (patient relatedness).
Sections 1, 5 and 6 address the background or context pertaining to the aforementioned measures. Section 1 assesses the background and demographic variables. Section 5 assesses concurrent events – any significant events that have affected the family unit or member of the family (e.g. health problems, financial issues, legal matters, etc.). Lastly, section 6 ascertains the support the carer receives and their living situation. See Platt et al. (1980) for more detail.
The SBAS provides the following summary scores: the patient’s disturbed behaviour and distress from the patient’s disturbed behaviour, the patient’s social performance and distress from the patient’s social performance, a well as objective burden and distress resulting from this burden (Platt et al., 1980).
Platt and colleagues (1980) only reported the preliminary psychometric properties of the SBAS; these preliminary statistics were not comprehensive (i.e. covering a range of reliability and validity indices) and they were based upon a very small sample. Recently, Harvey and colleagues (2008), in a review of the literature, found that there were inadequate data to verify the reliability and validity of the SBAS. Further, the instrument lacks feasibility and interpretation of the results is subjective as opposed to being standardised.
Family Burden Interview Schedule (FBIS)
The FBIS was developed by Pai and Kapur (1981) in India as no such measure had been devised to assess the burden on families in non-westernised countries, where the authors felt burden may be distinct owing to considerably different economic and cultural conditions.
The FBIS was constructed through consultation with caregivers of mentally ill individuals. First, unstructured interviews were conducted to ascertain the nature of burden; with particular emphasis on concrete or objective indicators of burden. The results were then analysed by the authors. Second, another series of interviews were conducted, which were analysed by an expert panel of six. The analyses were then compared and triangulated. The resulting categories were found to be comparable, although differing names were assigned (Pai and Kapur, 1981).
The FBIS measures six categories of family burden, namely: financial, effect on family routine, effect on family leisure, effect on family interaction, effect on physical health of other family members, and the effect on mental health of other family members. The focus of this inventory is upon objective burden. However, subjective burden is also measured but by only one item: ‘How much would you say you have suffered owing to the patient’s illness – severely, a little, or not at all?’ (Pai and Kapur, 1981; Schene et al., 1994). The scale generates scores on each of the aforementioned categories of burden.
The FBIS takes approximately 25 minutes to complete and needs to be administered by a trainer rater via an interview (Schene et al., 1994). Pai and Kapur (1981) originally reported good inter-rater reliability and validated the measure through correlating measures of objective burden with the measure of subjective burden. Further, Schene et al. (1994) stated that the psychometric properties of the FBIS are well established and that the FBIS is sensitive to change over time.
Burden Assessment Scale (BAS)
The BAS was developed by Reinhard and colleagues (1994) to assess family or caregiver burden in those caring for someone with a SMI. The scale is designed to assess both objective and subjective consequences of caregiving to someone with a SMI, whilst excluding the variance associated with the relative’s disruptive behaviours or the carer’s caregiving activities, as theoretically the authors consider the latter to be predictive of burden rather than a component of the burden construct. The authors consulted with family members of individuals with a SMI to review the scale for clarity; carers were not consulted about item generation and content.
The scale is comprised of 19 items: 10 assessing objective burden and nine measuring subjective burden. The objective burden items pertain to the observable effects of caregiving upon the family or the carer. For example, financial difficulties, disruptions in the household, the impact upon personal activities and role. Subjective burden refers to the family’s or caregiver’s feelings, attitudes and emotions regarding the role of caregiving, such as worry, shame, guilt and resentment (Reinhard et al., 1994; Schene et al., 1994).
According to Reinhard and colleagues (1994), the BAS has a stable factor structure as it is composed of five structures. Two of which measure objective burden (disrupted activities and basic social functioning) and three of which pertain to subjective burden (personal distress, time perspective and guilt). However, Ivarsson et al. (2004), when testing the construct validity of the Swedish version of the BAS, found a three-factor solution: feelings of worry and guilt, activity limitations, and social strain. The authors contend that this may have resulted from translation of the BAS, cultural differences or the homogeneity of their sample.
The BAS can be either self-administered or administered via interview, with both forms of administration displaying sound psychometric properties (Reinhard et al., 1994; Schene et al., 1994). Further, the BAS is brief and not time-consuming, and is also sensitive to change over time (Reinhard et al., 1994).
Experience of Caregiving Inventory (ECI)
The ECI was developed by Szmukler and colleagues (1996) with the aim of producing a self-report measure of caregiving that was satisfactory to carers and covered a diverse range of caregiving experiences. Further, the measure also needed to exemplify good construct and face validity. The ECI is a measure of the caregiving experience for people caring for someone with a SMI as opposed to a measure of burden as the ECI includes both positive and negative measures of caregiving (Joyce et al., 2000; Tarricone et al., 2006). However, the ECI has previously been utilised as a proxy measure of burden as it defines the areas of difficulty that carers face (Treasure et al., 2001).
Theoretically, the ECI is based upon a stress-appraisal coping framework (Szmukler et al., 1996).The ECI is essentially a measure of appraisal for carers of people with SMI (Joyce et al., 2000; Tarricone et al., 2006). The ECI was developed in consultation with caregivers of people with a schizophrenia spectrum disorder, with the 66 items being derived from caregivers’ responses (Szmukler et al., 1996). Subsequently these items were tested with another group of carers (Szmukler et al., 1996).
The ECI is composed of 10 dimensions: eight of which assess the negative experiences of caregiving and two of which evaluate the positive experience of caregiving. Difficult behaviours, negative symptoms, stigma, problems with services, effects on family, need for back-up, dependency and loss comprise the negative domains, while rewarding personal experiences and good aspects of the relationship with the patient form the positive dimensions (Joyce et al., 2000).
The ECI has been reported to have good psychometric properties, with Harvey et al. (2008) reporting the inventory to have both good reliability and validity. Joyce et al. (2000) found good construct validity for the scale, with the negative domains of the ECI predicting carer morbidity. Further, it has also been reported that the ECI is well accepted by carers (Harvey et al., 2008).
Perceived Family Burden Scale (PFBS)
The PFBS was developed by Levene et al. (1996) to measure the behaviours of patients with schizophrenia, as opposed to their symptoms, in a bid to delineate the objective and subjective facets of family burden. The authors utilised the input and insight of carers of people with schizophrenia throughout the development of the PFBS, with carers also contributing to the item content and rating whether the generated behaviours were problematic.
The scale consists of 24 behaviours, for which the carer indicates presence or absence in the patient in the previous month; this is the objective component of burden. The carer then rates how problematic each of the specified behaviours is to them personally; this is the subjective component of burden.
The PFBS has a two-factor structure that the authors termed ‘active’ and ‘passive’ based upon the behaviours subsumed under each of the factors. The active factor contained six behaviours, namely: talking loudly, yelling, using abusive language, threatening violence, throwing things and blaming others. The passive factor incorporates the following behaviours: looking sad, moping, hardly talking, staying in bed, looking messy, laughing frequently and abusing drugs. The remaining 11 behaviours cross-loaded on both factors. The PFBS is a self-report scale that is valid and reliable according to the authors. Further, the Chinese version of the PFBS has also been shown to have high internal consistency and test–retest reliability (Tsang et al., 2005). However, they concede that further validation should occur, especially with regard to principal components analysis. This would be recommended, especially with regard to the number of items that cross-load on both factors as almost half the behavioural items in the scale exhibit this relationship.
Involvement Evaluation Questionnaire (IEQ)
Development of the IEQ began in 1987 as there were no Dutch instruments that measured the consequences of caregiving (Van Wijngaarden et al., 2000). Schene et al. (1994) had conducted a large review of the literature and generated an item pool containing those items currently in use for measuring the consequences of caregiving (Van Wijngaarden et al., 2000). Experts were then interviewed and subsequent items were then developed. Draft versions were piloted and items that were not sensitive to change over time were removed as the authors conceived sensitivity to change to be a fundamental attribute of a good quality measure of caregiving consequences (Van Wijngaarden et al., 2000).
The IEQ is a 31-item self-report measure comprised of items that pertain to ‘the encouragement and care that the caregiver has to give to the patient, to personal problems between patient and caregiver, and to the caregiver’s worries, coping and subjective burden’ (Van Wijngaarden et al., 2000: s22).
The scale is composed of four main subscales, namely: tension, supervision, worrying and urging. Tension refers to stressful environment and interpersonal interactions between the patient and the other relatives. Supervision pertains to the tasks the carer has to undertake for the patient. Worrying is indicative of anxious cognitions regarding the patient. Finally, urging relates to attempting to motivate or getting the patient to comply with certain behavioural requests. The scores on all the subscales can be interpreted individually as well as being summed to produce an overall estimate of consequences of caregiving upon the carer. The IEQ also contains an additional four items not included in the subscales which assess the impact upon the carer’s role and his or her coping ability (Van Wijngaarden et al., 2000).
The IEQ is routinely extended in research with additional modules (see Van Wijngaarden et al.; 2000); however, it can be utilised independently. It is self-administered and takes approximately 10 minutes to complete. The IEQ is suitable for both research and clinical purposes (Van Wijngaarden et al., 2000).
Van Wijngaarden and colleagues (2000) report that the IEQ displayed adequate internal consistency across five sites and international translations. However, some sites (London and Verona) showed lower than satisfactory alpha levels on two of the scales: supervision and urging, respectively. The authors justify their conclusion with regard to internal consistency as being satisfactory, despite the alpha levels obtained for the two aforementioned subscales, as they subjected the data to principal component analysis and similar factor structures were evident across sites (Van Wijngaarden et al., 2000). Conversely, though, the authors did not report the results of the factor analysis nor the factor structure that was evident (Van Wijngaarden et al., 2000).
Family Burden Scale (FBS)
Madianos and colleagues (2004) constructed the FBS in order to overcome some of the previous methodological flaws they felt were inherent in the burden literature. Namely, they conceptualised the time frame of 1 month that is commonly utilised in other measures as too brief, and that burden instruments need to be developed and tested in a clinically homogeneous sample. Further, the vast majority of previous instruments have not been subjected to factor-analytic procedures to clarify their factor structure (Madianos et al., 2004; Schene et al., 1994). In a review of 21 instruments measuring burden conducted by Schene et al. (1994), it was evident that only five inventories had been subjected to factor-analytic procedures. Therefore, Madianos and colleagues (2004) constructed the FBS in a bid to overcome the aforementioned flaws. The FBS was developed specifically for measuring burden in caregivers of people with a schizophrenia spectrum disorder.
A scale of 45 open-ended questions pertaining to burden of care was piloted through interviews with family members of people with schizophrenia. This process refined the scale to 35 items; item reduction techniques were then carried out, resulting in a scale of 28 items. The FBS covers a period of the prior 6 months, is administered via an interview and takes approximately 28 minutes to complete (Madianos et al., 2004).
The FBS was then tested with a sample of caregivers living with people with a schizophrenic spectrum disorder. The results were subjected to factor-analytic procedures; after factor analysis 23 items remained. Burden, as measured by the FBS, is composed of four dimensions, three of which assess objective burden, namely: impact on daily activities/social life, aggressiveness and economic burden. Subjective burden is measured by one factor: impact on health (Madianos et al., 2004).
Madianos and colleagues (2004) reported the FBS factors to have acceptable levels of reliability; however, the subjective dimension (impact on health) alpha level was slightly below 0.70, which is commonly reported as the reliability cut-off (Nunnally, 1978). The FBS also demonstrated good concurrent validity, displaying significant correlations with measures of patient psychopathology, family environment and caregiver health (Madianos et al., 2004).
Discussion
The results of the above review highlight the disparity that exists in the field of caregiver burden research; especially in relation to carers of people with a SMI. This finding is similar to the conclusions drawn by prior reviews of the measurement of burden of care in SMI (Harvey et al., 2008; Schene et al., 1994, 2001; Schulze and Rossler, 2005). Further, it is evident that many of the instruments utilised to assess burden have differing conceptual definitions, poor psychometric properties, and limited specificity, utility and feasibility.
Theoretical definitions of the burden construct
Many of the measures reviewed have not evolved from a strong theoretical basis and display differing views as to the nature of the burden construct. This finding is comparable with that of Schene and colleagues’ (1994) conclusion that although researchers essentially agree with regard to the dimensions of the burden construct (objective and subjective burden), there is little consensus pertaining to the definition of burden and how it is best operationalised and measured (Schene et al., 1994). Similarly, a more recent review by Schulze and Rossler (2005) asserted that the construct required improved theoretical clarity to further the quality of research in the area.
This lack of conceptual clarity is evident in, for example; the FBIS and the FBS, which are particularly focused upon the objective notion of burden, with less attention being given to the subjective component of the construct (Madianos et al., 2004; Pai and Kapur, 1981), with the FBIS utilising only one item to assess subjective burden and the FBS having one scale confined to the impact on the health of the caregiver to measure subjective burden (Madianos et al., 2004).
Further, some of the measures are focused upon the behaviour of the person being cared for to ascertain the burden felt by the carer, with the PFBS and the SBAS being behaviourally based – the former being solely based upon the behaviours of the patient (Levene et al., 1996; Platt et al., 1980). However, others conceptualise the consequences of caregiving to be distinct from the behaviours exhibited by the patient. Reinhard and colleagues (1994) sought to eliminate the variance associated with challenging behaviours as they theorised that such behaviours were predictive of burden rather than constituting part of the construct.
Furthermore, researchers within the sphere of caregiver burden even questioned whether the construct should be termed as such due to the inherent negative conations that arise from the terminology (Awad and Voruganti, 2008; Szmukler et al., 1996), with some researchers contending that more neutral terminology should be adopted. This is evident in the work of Szmukler and colleagues (1996) who use the term ‘caregiver experience’ rather than ‘family burden’ and ‘burden of care’. This change in terminology is meant to demarcate that caregiving can have both positive and negative consequences (Awad and Voruganti, 2008; Szmukler et al., 1996).
However, this brings into question the very core of the empirical field: the rationale for investigating the construct of burden to begin with? Why as researchers are we interested in this area? What pragmatic utility does the construct hold?
Theoretically, the imperative behind investigating the construct of burden is facilitating the understanding of the negative impacts of informal caregiving upon the family and the primary caregivers. This knowledge can assist with negating such impacts through the provision of interventions, support and assistance. Carers of people with a SMI incur financial problems, role impairments, poor family relationships and stigma (Awad and Voruganti, 2008; Ohaeri, 2003). As a result they suffer from reduced well-being (Webb et al., 1998). Moreover, and perhaps most notably, carers of people with SMI have poor physical and mental health; this is reflected in increased visits to the doctor, emergency department consultations and even hospitalisations (Awad and Voruganti, 2008; Moller et al., 2009; Schene et al., 1998; Van Wijngaarden et al., 2000; Webb et al., 1998).
Although it is evident that the field is conceptually fragmented with differing views and modes of operationalising the burden construct, some commonalities remain: the majority of measures included assessments of financial hardships, impacts upon the role functioning of the carer and effects on the carer’s physical and mental health.
Psychometric properties of the burden measures
From our review, it seems that a number of the measures evaluated lack sound and well-established psychometric properties, with burden, as assessed by the ZBI, theoretically purported to be a uni-dimensional construct. However, studies have indicated an inconsistent factor structure (Hassinger, 1986; Knight et al., 2000; Whitlach et al., 1991). Furthermore, there are inadequate data to assess the psychometric properties of the SBAS (Harvey et al., 2008). The authors of the PFBS and IEQ, although reporting favourable psychometric properties, contend that their instruments require further validation (Levene et al., 1996; Van Wijngaarden et al., 2000). The findings of this review with regard to the psychometric properties of burden measures are comparable with previous reviews (Harvey et al., 2008; Schene et al., 1994, 2001; Schulze and Rossler, 2005). Recently, Harvey and colleagues (2008) concluded that all measures of caregiver outcomes, not just measures pertaining to burden of care in SMI, required further development and validation.
The FBIS and ECI have been reported as demonstrating good psychometric properties (Harvey et al., 2008; Joyce et al., 2000; Pai and Kapur, 1981; Schene et al., 1994). Further, the BAS has also been reported to have good psychometric properties, although differing factor structures have been identified in different languages (Ivarsson et al., 2004; Schene et al., 1994). The FBS displays adequate psychometric properties, although the reliability of one of the domains is slightly less than recommended. Thus, only half of the measures reviewed demonstrated adequate psychometric properties, none of the measures have well-established psychometric properties, and the other measures exhibit inadequate psychometric properties or require further validation.
Specificity of the burden measures
All of the measures reviewed were specific to measuring burden of caregiving in carers of people with a psychiatric illness. However, as outlined in the ‘Introduction’, psychiatric or severe mental illness was not limited to schizophrenia and bipolar disorder. The ZBI was specifically developed to assess burden in carers of people with dementia and Alzheimer’s disease (Zarit et al., 1980).
However, three of the measures were developed to assess burden in carers of people with schizophrenia, namely the FBIS, PFBS and FBS (Levene et al., 1996; Madianos et al., 2004; Pai and Kapur, 1981). None of the measures was specifically developed to assess burden of caregiving for carers caring for a person with bipolar disorder. Therefore, the instruments outlined above need to be assessed for use in capturing burden in this population. Alternatively, an instrument that is specific and sensitive to the consequences of caregiving in both schizophrenia and bipolar disorder needs to be developed.
Utility and feasibility of the burden measures
Even though there are a range of instruments to measure burden of caregiving, some of the measures reviewed lack utility and feasibility. That is, they are not capable of informing clinical practice to assist carers, they are too time-consuming or require specially trained interviewers for administration.
Specifically, the ZBI exhibits low utility as it provides a global score of burden as opposed to subscale scores of the domains of the construct (Zarit et al., 1980); it allows targeted interventions to be planned and implemented in order to relieve the relevant aspects of burden of care exhibited. The PFBS also has limited utility in addressing carer burden due to the conceptual design of the instrument being limited to the challenging behaviours exhibited by patients (Levene et al., 1996).
The remainder of the reviewed scales demonstrate better utility for research and practice as they report subscale scores of the domains of burden conceptualised in each. Conversely, though, some exhibit better utility than others; for instance, the PFBS only indicates which behaviours the carer finds most problematic (Levene et al., 1996), whereas the IEQ indicates scores on the four domains the authors conceptualise as the burden construct: tension, supervision, worrying and urging (Van Wijngaarden et al., 2000). The inclusion of domain scores facilitates intervention and can also be utilised to test the effectiveness of interventions and psychopharmacological treatments in research.
Related to clinical utility is the method through which the instruments were developed and their acceptability to carers. The majority of instruments utilised carers in the development process; however, this was to differing extents (ranging from pilot testing, the evaluation of instruments for clarity, to item generation). Only the PFBS utilised carers in the generation of item content (Levene et al., 1996). In a recent review of carer outcome measures in mental health, it was evident that only the ECI and IEQ were deemed as acceptable to carers out of the burden of care instruments they reviewed (Harvey et al., 2008).
With regard to feasibility, three (FBS, SBAS and FBIS) of the eight measures reviewed require a trained interviewer to administer the schedule (Madianos et al., 2004; Pai and Kapur, 1981; Platt et al., 1980). This limits the feasibility of the instrument for research purposes. Furthermore, the SBAS is very time-consuming to complete, rendering its use not suitable for clinical practice. In addition, the other interview schedules, although requiring significantly less time than the SBAS to complete, still require a moderate amount of time, which is also inappropriate for clinical practice. The other five scales exhibit better feasibility for use in research and clinical practice as they are self-administered questionnaires that are less time-consuming to complete.
Conclusion
It is evident from the above discussion that there are numerous inadequacies in the reviewed burden assessment tools ranging from the conceptual definition of the construct through to the acceptability of the measures to carers. Furthermore, the mere abundance of measures also impedes the development of a better understanding of the construct, with the field lacking a well-established measure allowing for comparison between research endeavours. These findings are in accordance with early reviews pertaining to burden of caregiving in SMI (Harvey et al., 2008; Schene et al., 1994, 2001; Schulze and Rossler, 2005), displaying that the field is in considerable need of further development.
It is recommended that one of the existing burden instruments be routinely adopted in research to facilitate comparison, with the IEQ and ECI being the superior choices based upon this review. Alternatively, researchers should seek to collaborate and develop a new instrument that overcomes all of the inadequacies that are apparent in the current assessment tools. This collaboration should involve caregivers as central informants on the nature of the burden of care construct. In addition, carers should be directly involved in the development and generation of items, which should subsequently be exposed to rigourous psychometric testing. Such development could begin with a consultation process with carers of people with a SMI using items from the ECI and IEQ as these measures are deemed the most acceptable to carers. This process would facilitate a clearer conceptualisation of the construct as well as an extension of the construct if deemed necessary by the carers.
It is critical that a psychometrically sound, theoretically based, utilitarian, pragmatic measure exists to measure a construct that has significant impacts upon the carer’s health, well-being and quality of life. In addition, burden is also known to affect other significant variables that impinge upon the illness outcomes of the patient with a SMI, such as expressed emotion (Brown et al., 1972; Hooley, 2007).
Although this review contributes to the understanding of burden of care in SMI, several limitations should be noted. Most notably, only one database (PUBMED Central) was utilised as the basis of this qualitative review; however, the authors believe that a representative sample of research measuring burden of care in SMI was obtained. Furthermore, this review could not report on the same indices across all of the measures as the necessary information was not available in the literature. Moreover, the aim of this review was to provide a broad qualitative review of the instruments to assist with burden of care research, and thus a future review could specifically report on the psychometric properties of the burden of care measures.
In addition, this review only assessed instruments and articles written in English and as caregiving is a social phenomenon it takes place within a cultural context which may be distinct in different parts of the world. Future research should conduct reviews in different languages in order to facilitate cross-cultural comparison.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.