
Abstract
Australian and New Zealand Journal of Psychiatry 2006; 40:777-782
While entrance to a university or other tertiary education institutions is a joyous time, it can be a stressful life event for some students. First-year students are particularly at-risk as they face a number of new stressors during the transitional period of starting a new life in university or college [1]. Previous studies suggest high rates of psychological morbidity, especially depression and anxiety, among university or college students in Asia and in countries all over the world [2–7]. For example, an increase in psychological disturbance was reported among students following the transition to university in the UK [8]. Similarly, a survey in 1999 by researchers in the US reported that 30% of college entrants felt overwhelmed by the transition to college life [1], and concerns about mental wellbeing of tertiary education students made headline news in the mass media [9]. Psychological distress may result in withdrawal from study as first-year students were found to be twice as likely to drop out as their counterparts in the second and third years [10]. Adlaf et al. [2] found a prominent inverse relationship between year of study and mental health in university students, those at greatest risk being first-year students.
Psychological morbidity in students represents a neglected public health problem [5], bearing major implication for campus health services and mental health policy-making [1, 4]. Understanding of this phenomenon is important at both the individual and the societal levels [11], in terms of impact on the person's educational attainment, future occupational achievement and quality of life. Epidemiological data are valuable in service planning and development. However, prevalence of depression, anxiety and stress in students in higher education is unknown in Hong Kong. Because most tertiary education students in Hong Kong have access to emails and the Internet for college notices and many other college-related information, we adopted a websurvey method to investigate the prevalence of mood and emotional disturbances among Hong Kong tertiary education students.
Method
There are 10 tertiary education institutes in Hong Kong, which include traditional universities and vocation-based training institutions (e.g. The Institute of Education, which trains teachers). All tertiary education students in Hong Kong are issued email accounts by their colleges or universities, and they are often expected to access the Internet for assignments and notices. We therefore conducted this selfadministered, cross-sectional web-based survey taking advantage of their universal computer and email access. All first-year students of the 10 institutions were invited to participate. The study was publicized by posters and flyers distributed during orientation activities at the beginning of the academic year in September 2003. The students were formally invited to participate by email via their university email address in October, the second month of their studies. The email provided an access link to the questionnaire website, which was passwordcontrolled. Students were given information on the purpose of the survey, with an emphasis on confidentiality and anonymity. Students who completed the survey were automatically entered into a prize draw. Prizes included MP3 players, digital cameras and book tokens. Two reminder emails were sent 1 week and 2 weeks, respectively, after the first invitation. No formal written informed consent was obtained. Consent was assumed if students completed the questionnaire. The study was approved by the local Institutional Review Board.
The self-administered questionnaire consisted of the following: a record of demographic details and the 42-item Depression Anxiety Stress Scales (DASS) [12, 13]. The depression scale assesses dysphoria, hopelessness, devaluation of life, self-deprecation, lack of interest or involvement, anhedonia and inertia. The anxiety scale assesses autonomic arousal, skeletal muscle effects, situational anxiety and subjective experience of anxious affect. The stress scale is sensitive to levels of chronic non-specific arousal. It assesses difficulty relaxing, nervous arousal, and being easily upset or agitated, irritable or over-reactive and impatient [13]. The DASS is a self-administered instrument with wellestablished psychometric properties in both clinical and community samples, and it has been shown to differentiate between the three states of depression, anxiety and stress [14–17]. All elements of the survey were available in both English and Chinese [18] and respondents could choose to respond in either language. Respondents were given immediate feedback on their depression, anxiety and stress scores, with brief advice on channels for seeking help. Moreover, the questionnaire website also provided links to websites that provide health education on emotional issues. The questionnaire website was closed after the study period (4 weeks).
Statistical analysis
Statistical analysis was conducted with the spss for Windows platform (SPSS Inc., Chicago, IL, US). T-tests were conducted to compare differences in DASS scores between different student groups. In cases where the variances were significantly different, a further t-test that did not assume equality of variances was conducted. Cohen's d, as a measure of effect size, was calculated to measure the magnitudes of differences in DASS scores between student groups.
Results
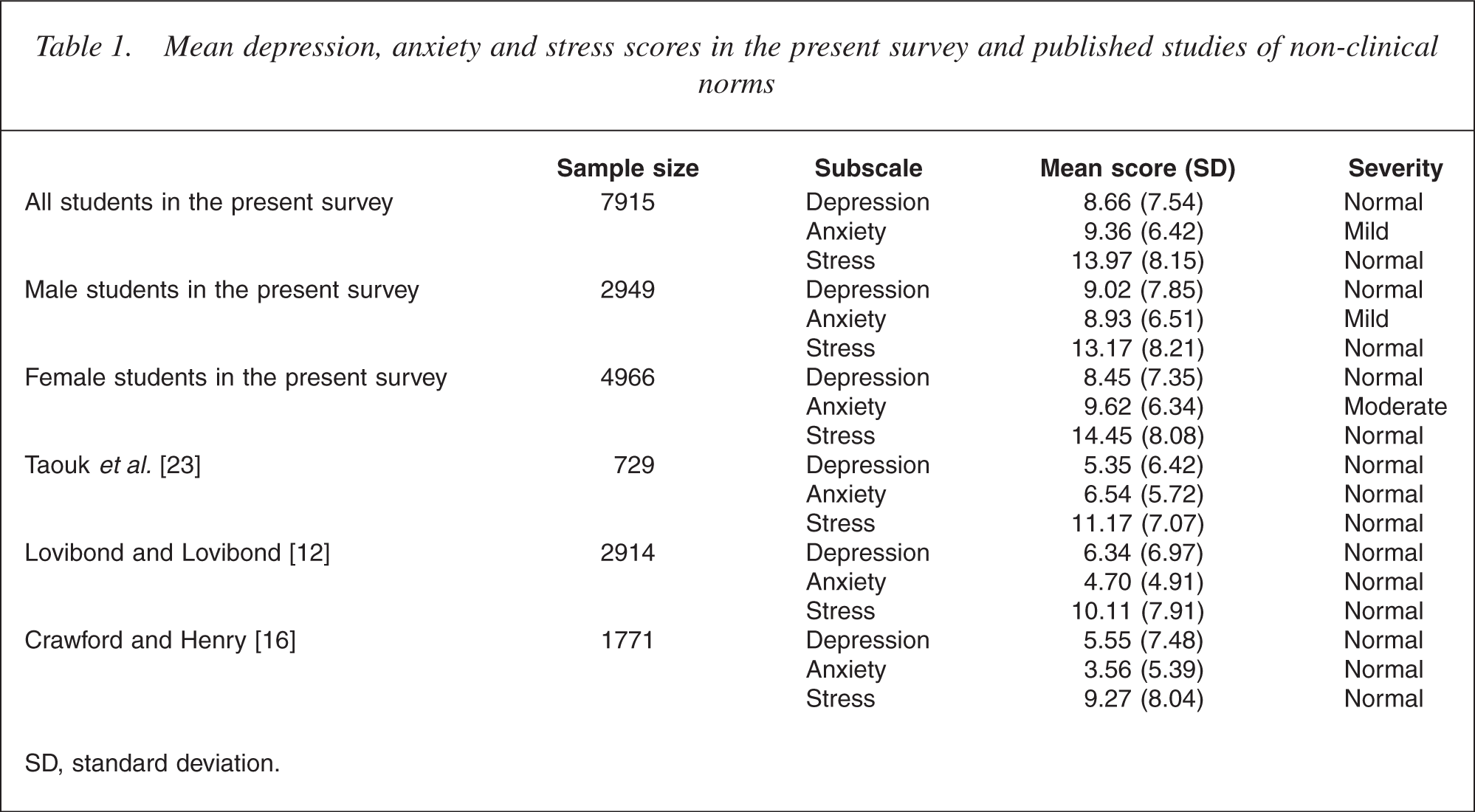
Out of a total of 28 773 first-year tertiary education institute students in Hong Kong, 7915 completed the questionnaire, representing a response rate of 27.5%. Sixty-three per cent of the respondents (n = 4966) were female. Ninety-nine per cent (n = 7841) of the respondents were single; 11.4% (n = 911) were aged 18 or below, while 86.4% (n = 6846) were aged 19-24. The majority of the students lived either with their parents and/or siblings (71.4%, n = 5650) or with roommates (26.3%, n = 2083), while 1.4% (n = 113) lived alone. Eleven per cent of the respondents (n = 850) reported having to see a doctor regularly for health problems, 1.4% (n = 112) have seen a psychiatrist before, and 8% (n = 643) reported a history of psychiatric contact in a family member. The mean depression, anxiety and stress scores in all students, male students and female students, respectively, are presented in Table 1, while Table 2 reports on the severity distribution of DASS scores based on score ranges from the DASS manual [12]. Female students had significantly higher anxiety (t = −4.61, df = 7,913, p < 0.0001, Cohen's d = 0.107) and stress (t = −6.79, df = 7,913, p < 0.0001, Cohen's d = 0.158) scores compared with male students, while male students had higher depression (t = 3.24, df = 7,913, p = 0.001, p = 0.001 if variances not assumed to be equal, Cohen's d = 0.075) scores.
Mean depression, anxiety and stress scores in the present survey and published studies of non-clinical norms
Severity distribution (%) of DASS scores among participants in the present survey
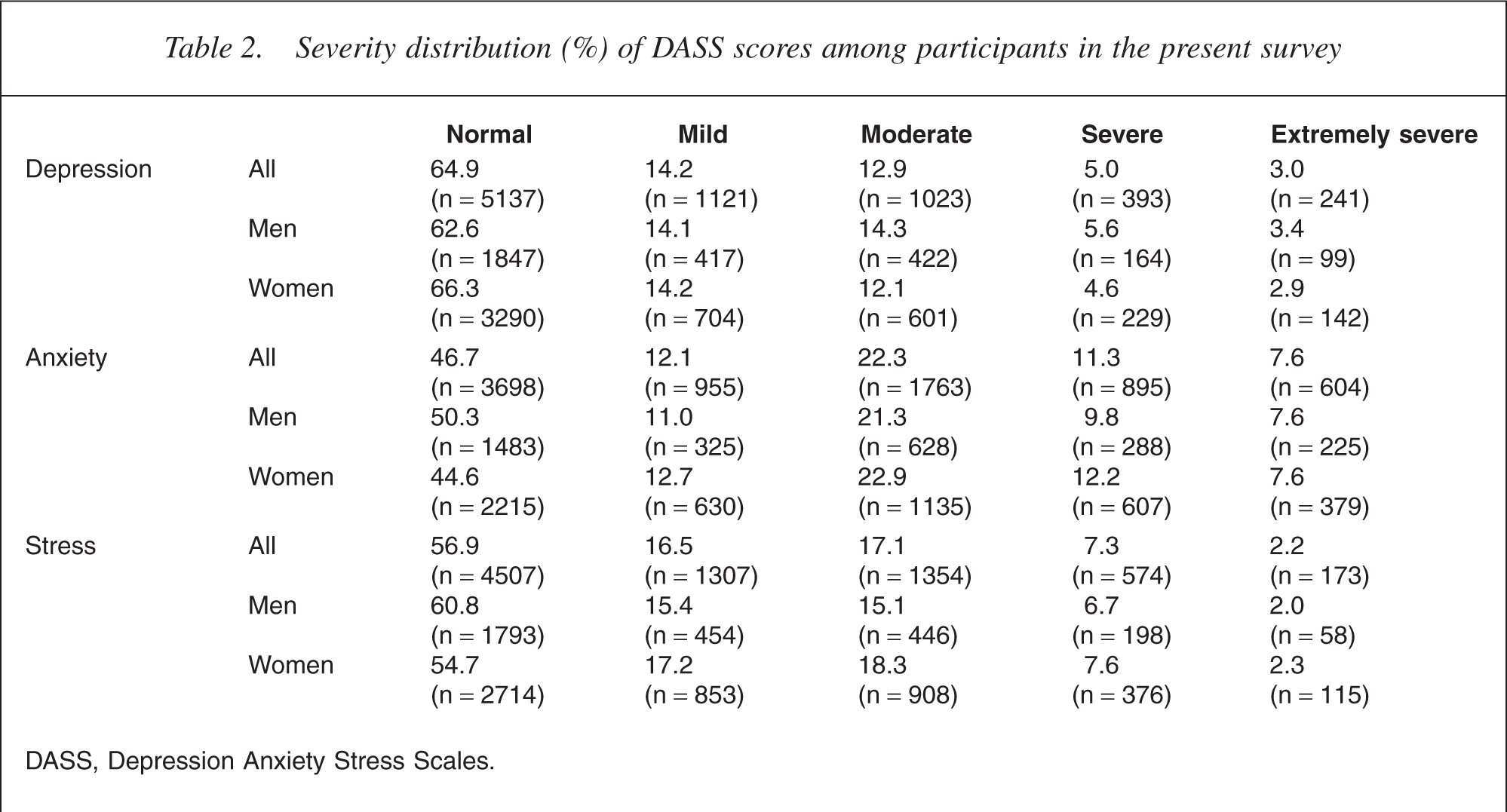
DASS, Depression Anxiety Stress Scales.
Table 3 shows that students with a history of general health problems or psychiatric problems and students with a family psychiatric history reported significantly higher depression, anxiety and stress scores.
Relationship between DASS scores and students' health or family psychiatric history
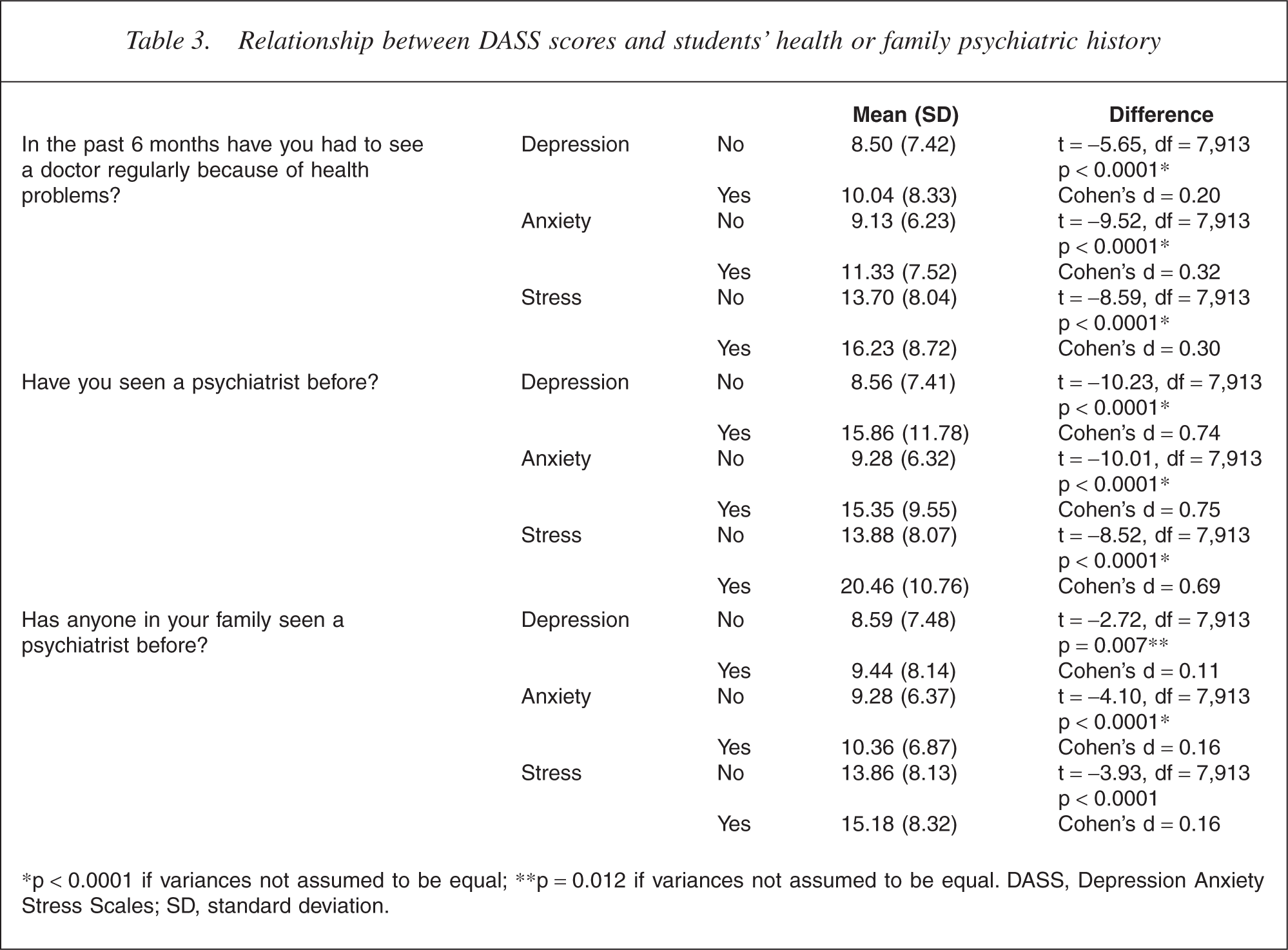
∗p < 0.0001 if variances not assumed to be equal; ∗∗p = 0.012 if variances not assumed to be equal. DASS, Depression Anxiety Stress Scales; SD, standard deviation.
Discussion
Use of web surveys
Web surveys are increasing in popularity because of a general increase in computer and Internet usage, particularly among college students. With the very rapid escalation in Internet usage and the rapid change in societal attitudes towards on-line surveys and other survey techniques [19], we expected web-based surveys to become a significant method in health research. Web surveys have been endorsed as an effective mode of collecting data from higher-education students, who have high rates of Internet use [20, 21]. Web surveys are less costly and more convenient (especially in terms of the ability to collect and analyse data rapidly) for researchers and present a more attractive multimedia platform and perhaps improved privacy to student respondents as most of our students have their own personal computers. Given the almost universal Internet access among Hong Kong students, our response rate of 27.5% was similar to reported response rates in national mail-out surveys [19]. Whether web-based surveys are superior to pencil and paper surveys in examining psychological morbidity requires further study, for example, by doing surveys using both methods to compare symptom reporting. It is, however, worth noting that previous studies on selfreported alcohol and illicit drug use in undergraduate students found that the web-survey method produced a significantly higher response rate than the mail-survey method and that the prevalence rates did not differ significantly between the two modes [20, 22], thus suggesting that web surveys can be a useful tool in conducting research on sensitive, mental health-related issues in students. Potential biases with web-based surveys are possible. Because the participants in our study were approached through their university-provided email addresses, the response rate in the present web-based survey may have been affected by students' concerns about computer security or their preference for other email accounts. Furthermore, acknowledging having an emotional problem is extremely difficult in the society of Hong Kong, and this may contribute to non-response in some students. In summary, judging from the significant number of responses in this study, web-based surveys deserve a careful examination as a method for mental health surveys in this age of information technology.
Depression, anxiety and stress levels
The present study found that our sample of first-year tertiary education students have higher mean DASS depression, anxiety and stress scores (Table 2) compared with previously published normative data [12,16], and with the scores of 729 local Chinese from the general population in Hong Kong [23]. This suggests that students in our sample suffered greater depression, anxiety and stress than international and local general population samples. Although the DASS is not a diagnostic instrument, it is worth noting the rates of depression, anxiety and stress symptoms of moderate severity or above as such symptom levels are likely to lead to some functional impairment and may require attention from health-care professionals. In the present study, the rates of depression, anxiety and stress symptoms of moderate severity or above were 20.9% (n = 1657), 41.2% (n = 3262) and 26.5% (n = 2101), respectively (Table 3). Previous studies that investigate mental distress in tertiary education students using other survey methods and rating scales found higher levels of mental symptoms in students when compared with age-matched controls [2, 5], thus supporting our hypothesis that being a student is associated with higher levels of psychological morbidity when compared with their peer group. Interpretation of our data is limited by the fact that our respondents could choose to respond either in English or in Chinese but we did not record which version they used, thus we were unable to examine if there are differences between respondents in these groups.
Previous data on gender difference in depression, anxiety and stress scores from DASS were inconclusive [12, 16, 23]. Our findings of female first-year students having significantly higher stress and anxiety scores and male first-year students having significantly higher depression scores are in keeping with results from published studies using different instruments in which higher psychological disturbance [7] and elevated psychological distress [2] were found among female undergraduates, and higher depression rates found among male undergraduates [24]. However, because low effect sizes were found, no clear conclusion could be drawn concerning gender difference.
Psychological morbidity in students
While the transition to adulthood represents a high risk period for the onset of depression generally [25], young people who enter tertiary education may face new social and intellectual challenges that may increase their risk of suffering depression, anxiety and stress. In Hong Kong, the economic downturn in recent years probably adds to the pressures of tertiary education students because their future and employment prospects are more uncertain than ever before. It would be interesting to further study how students' depression, anxiety and stress levels would change once they pass their initial adjustment period and as they face challenges in different years at tertiary education.
The high rates of depression, anxiety and stress among first-year tertiary education students have major implications. Not only will psychological morbidity have adverse effects on the student's educational attainment and quality of life, but family life and institutional life may be disrupted. Prolonged untreated depression, anxiety or stress may impact upon the functioning and productivity of the people who are affected, thus presenting a public health problem. Looking further to the future, Stewart-Brown et al. [5] pointed out that as tertiary education students are likely to become the future policymakers, managers, doctors and teachers of our community, their belief that high levels of stress and anxiety are normal and unavoidable is likely, through social policy, workplace practices, medical opinion and approaches to teaching, to have a disproportionate impact on the health and wellbeing of the pubic. To reduce psychological morbidity in this group, primary and secondary prevention measures are necessary to enhance psychological wellbeing of the student body in general and to identify high-risk students who may be in distress already or have a history/family history of mental health problems. Early intervention in high-risk groups may help to reduce morbidity and subsequent impairment. Attention has been focused on the development and provision of adequate and appropriate services to distressed students in a form that is accessible and acceptable to them [1, 4]. Efforts should also be made to demystify and destigmatize emotional disorders in order to facilitate early help-seeking.
Funding and support
We are grateful to Lundbeck Hong Kong for providing prizes for the prize draw. However, Lundbeck Hong Kong had no role in the study design, data collection, data analysis, data interpretation or writing of the report.
Footnotes
Acknowledgements
Thanks to Pak Sham for his help with the statistical analysis; O. C. Chan, Department of Psychiatry, University of Hong Kong, for technical support; and the Hong Kong Tertiary Institutions Health Care Working Group for their collaboration.