
Abstract
People with a mental illness are among the most vulnerable in our community, and families affected by parental mental illness are more likely to experience social isolation, financial hardship and marital discord [1]. Parental mental health places children at a significantly greater risk of having lower social, psychological and physical health compared with children from families not affected by parental mental illness [2] with longterm effects including social and occupational dysfunction [3]. In addition, it has been estimated that between 25% and 50% of children whose parent has a mental illness will experience some level of psychiatric disorder, compared with 10–20% of other children [4].
A number of studies have identified the needs of children whose parents have a mental illness [5–7] particularly associated with the parent being hospitalized [7]. Additionally, normal attachment behaviours such as love, security and nurturing [8, 9] might be disrupted because of a parent's delusional [10] or depressed behaviour [11] leading to short and long-term interpersonal difficulties [12]. Such children are often referred to as ‘hidden children’ [6] because mental health professionals are often unaware that their patients are parents. As adult mental health workers are a point of intervention for parents with a mental illness, an opportunity exists for these workers to identify issues for children whose parent has a mental illness, and to address parenting responsibilities. The barriers that adult mental health workers face, in discussing parenting issues with adult patients as well as working with their children, was consequently sought in this study.
Service delivery to families where a parent has a mental illness is often problematic. Many agencies traditionally take a categorical approach to patients, with a tendency to focus on either the child (e.g. in terms of child protection) or the adult (e.g. for his or her mental health needs or parenting capacity). Nicholson et al. [13] report that programs or treatment settings may not allow adults with children to participate, for example, residential programs or emergency shelters. However, Wang and Goldschimdt [14] found that psychiatric patients wanted family-focused interventions rather than focusing solely on themselves as the identified patient.
As well as organizational barriers, many human and health agency workers do not have the skills, knowledge and knowledge to identify, refer and/or intervene appropriately with different family members. Bibou-Nakou [15] illustrated this problem with Greek teachers whoacknowledged that supporting children whose parents had a mental illness were part of their responsibilities, but at the same time reported inadequate skills to do so. Similarly, the difficulty for many child protection workers is that they are not adequately trained in the area of mental health. Risley-Curtiss et al. [16] argue that while research in the assessment and treatment of serious mental illness has expanded and changed in the last 10 years, much of this research is published in the mental health literature, and is not readily accessible to child protection workers.
As well as a skills and knowledge deficit, Ackerson [17] contends that many human and health agency workers focus on the problems, rather than the capacities of parents with a mental illness. Nicholson et al. [13] points out that organizational responses tend to be only available when parents or children have a diagnosable problem or after abuse and/or neglect has been identified. Consequently, while children of parents with a mental illness are at risk of developing various problems, preventative based interventions are not often implemented.
Overall, there appears to be a substantial lack of evidence-based research regarding the organizational knowledge, skills and resources required for working with families affected by parental mental illness. The Australian Infant, Child, Adolescent and Family Mental Health Association highlighted the need ‘for improvement in mental health agencies in the identifying and responding…’ to children in such circumstances [18], p.44] and specifically the need to identify the barriers for adult mental health workers when working in this area.
Several studies [19–23] have sought to identify the barriers for mental health staff when working with families affected by parental mental illness. Dean and Macmillan [21] found organizational structure and role constraints to be significant barriers. Similarly, Grunbaum and Gammeltoft [22] found issues regarding service ideologies and professional role boundaries to be problematic. Byrne et al. [20] highlighted barriers associated with poor communication between agencies and a shortage of appropriate community resources. A lack in knowledge and skills has also been identified, particularly as they pertain to judging parenting capacity, working with children and to the causal factors and issues of mental health prognosis [19, 21].
Barriers have also been identified within patients and families. Bibou-Nakou [19], in focus group interviews with 18 workers, found that a child's age was considered to be a major obstacle for talking to children about their parent's mental illness, although she suggests that this assumption may be based on inadequate knowledge regarding child development. Additionally, workers' perception that family members were not willing or able to discuss a parent's mental illness proved an impediment for some [21]. However, Nicholson [23] points out that Parents with mental illnesses express concern that if they disclose their parenting status or, more important, problems with parenting, treatment providers will file reports with child protective services, thereby increasing the probability that they will lose their children (p.357).
The need to identify the barriers to working effectively with families affected by parental mental illness is important, particularly for adult mental health workers [18]. However, the relative importance of barriers and the differences in barriers between adult mental health workers and other mental health professionals has not been previously investigated. Such knowledge has important administrative and training implications. Consequently, there were three aims to this study. The first aim was to identify the core barriers that impede adult mental health and other workers from working with patients about parenting and their children. Based on previous studies [19–23], it was hypothesized that organizational and role constraints, a lack of skills, knowledge and resources, ineffective liaison between agencies and issues within families themselves would be identified as core barriers for workers. The second and third aims were to have workers rate the importance of these barriers and to compare barriers for adult mental health workers with other workers. Owing to the original nature of these research aims hypotheses are not proposed.
Method
The research involved two data collection phases; the first, qualitative phase involved collecting verbatim responses from participants regarding barriers and the second, quantitative study involved participants responding to scaled, questionnaire items based on the qualitative barriers identified at phase one. This study was part of a larger evaluation project that examined the knowledge, skills and activities (e.g. referrals) of mental health and welfare workers.
Participants
The initial qualitative phase of this study included 60 (42 women and 11 men) (some workers wished to remain anonymous hence identifying characteristics were not provided [i.e. seven did not indicate gender]). mental health and welfare worker participants. Thirty-two (27 women and 5 men) participants responded to the second quantitative component of the study, including 20 adult mental health workers (e.g. adult inpatient psychiatric services, adult mental health services) and 12 other mental health professionals who provide general psychological and/or welfare activities with adults, children or families such as support to families, outreach services, community health activities, services to children with mental health problems or general support to those with mental health problems (e.g. child and adolescent mental health services, community health agencies).
All participants signed informed consent forms and responded using reply paid envelopes. Of the initial 60 respondents (at phase one), 52 consented to participate at time two, of which 26 responded to a mailed questionnaire. In addition, six further participants completed the second phase questionnaire only. Participation in the study was voluntary and anonymous to trainers and steering committee members.
Instruments
Participants responded to the question ‘For those of you that you For those of you that
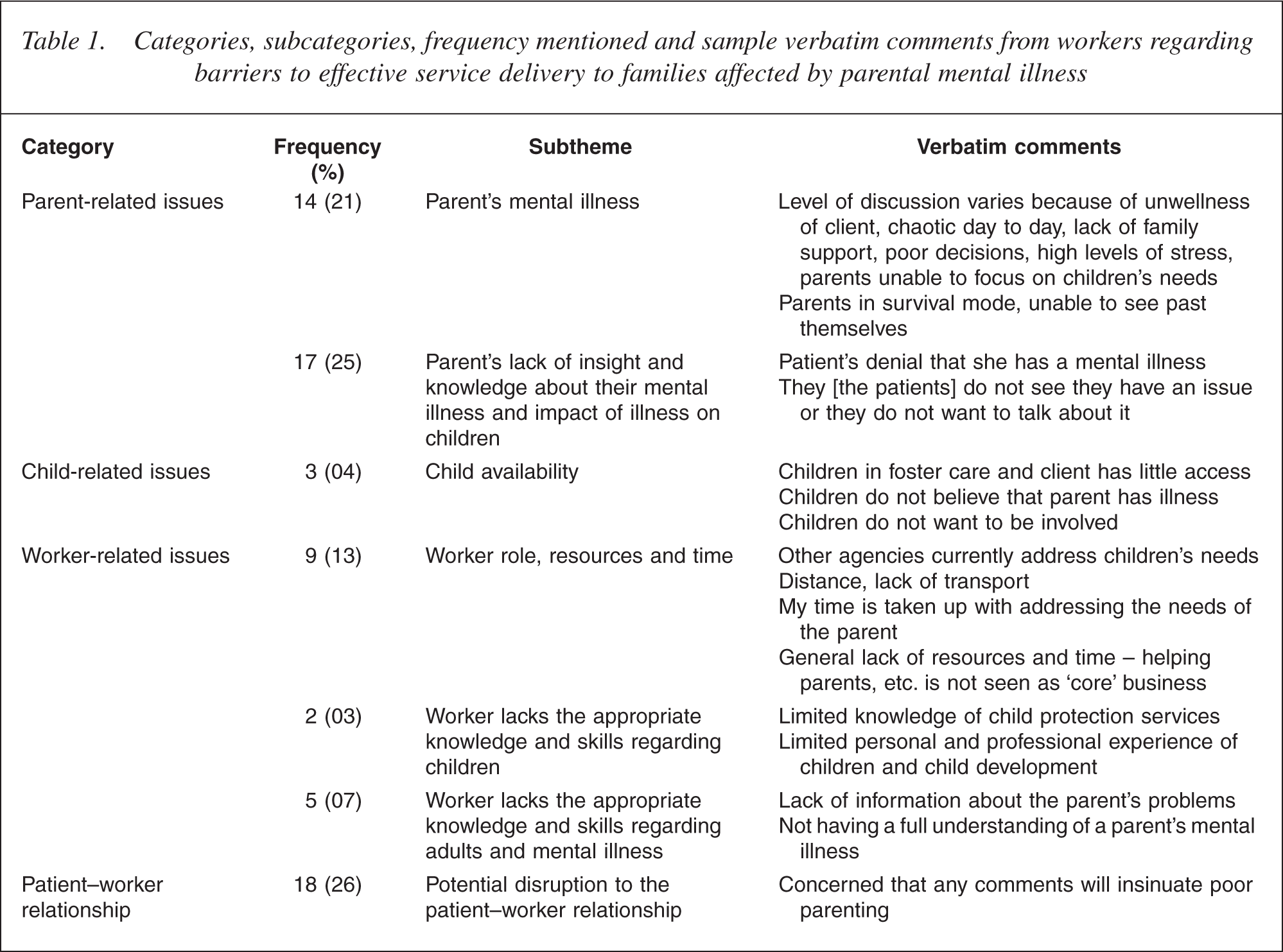
Categories, subcategories, frequency mentioned and sample verbatim comments from workers regarding barriers to effective service delivery to families affected by parental mental illness
Totals and Worker type means and standard deviations (SD) for barriers to talking to patients about mental illness, parenting and children
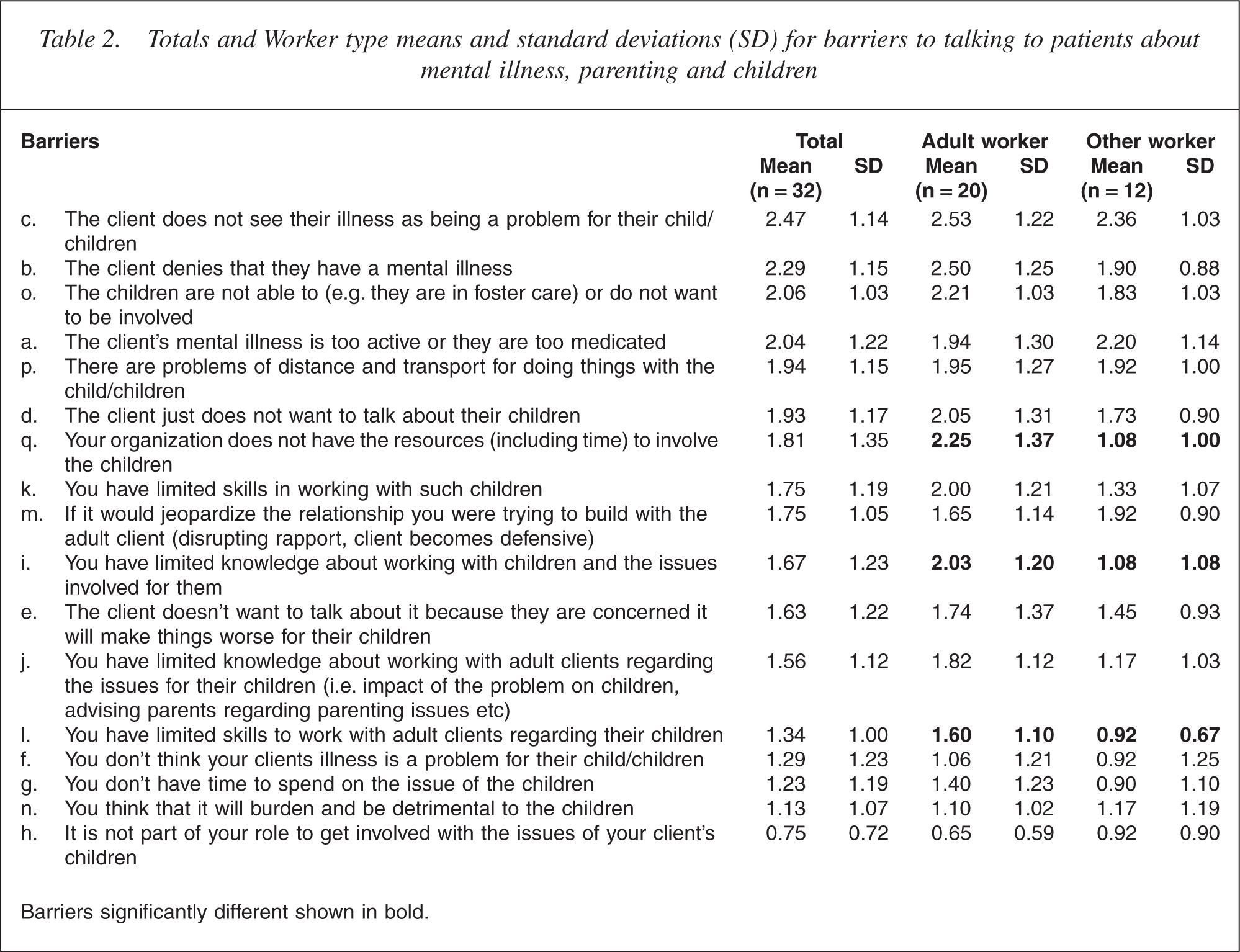
Barriers significantly different shown in bold.
Participants responded as not applicable (n/a) or on a 5-point scale from strongly disagree (0), disagree (1), neither agree or disagree (2), agree (3) or strongly agree (4). The items are shown in Table 2.
Procedure
Data were collected using two, opportunistic approaches. The first approach involved voluntary participation of workers prior to attendance at a ‘Getting There Together’ training program (the training program involves professional development that aims to increase the routine identification, engagement and referral of children whose parents have a mental illness by adult mental health clinicians and community welfare workers). The second was when researchers and steering committee members (see Acknowledgements) asked workers in the community to voluntarily respond to the first qualitative phase and to the second quantitative phase of the study, 6 months later. Ethics approval was gained from Charles Sturt University and Eastern Health Region ethics committee (Human Services and Health Victoria).
Results
Themes were identified from the first qualitative phase by the two researchers independently, who then pooled shared categories, noting key differences and reaching an overall consensus. The themes were then further validated by a third researcher independent to the study, who went through these categories and questionnaires to ensure that categories accurately reflected workers' responses. Workers highlighted four key barriers to effective service delivery for families affected by parental mental illness. The first barrier involved issues to do within the mentally ill parent, such as his or her general state of sickness, preoccupation or lack of insight and knowledge about his or her mental illness and the impact of the illness on the child/children. The second barrier related to the degree of access that the worker had to the child as well as what workers considered to be an unwillingness of the child to be involved. The third barrier was related to worker issues and included: worker role, resources and time (on several occasions verbatim comments are summarized or combined to illustrate the points), a lack of appropriate knowledge and skills regarding children and a lack of appropriate knowledge and skills regarding adults and mental illness. The final barrier was related to the patient–worker relationship with participants reporting a potential disruption (or loss of rapport) to the patient–worker relationship if they raised the issue of parenting and mental illness.
In order to compare the barriers in terms of relative importance Means and Confidence Intervals for the 17 barriers was calculated. It was decided to illustrate the relative importance of the barriers in this way for several reasons. The scores can be viewed and compared graphically, readers can determine the relative spread of scores across the participants (i.e. the interval in which 95% of scores fall) for each barrier, and finally significant differences (for the purposes here it was not thought necessary to undertake t-tests to compare each of the barriers with each other. In addition, such an approach would increase the likelihood of family wise error) can be determined (i.e. where Confidence Intervals do not overlap; for a detail exposition of the approach see [24]). These are shown in Fig. 1.
Comparison of means and confidence intervals for the 17 barriers identified by workers (legend for barriers/items is shown in Table 2).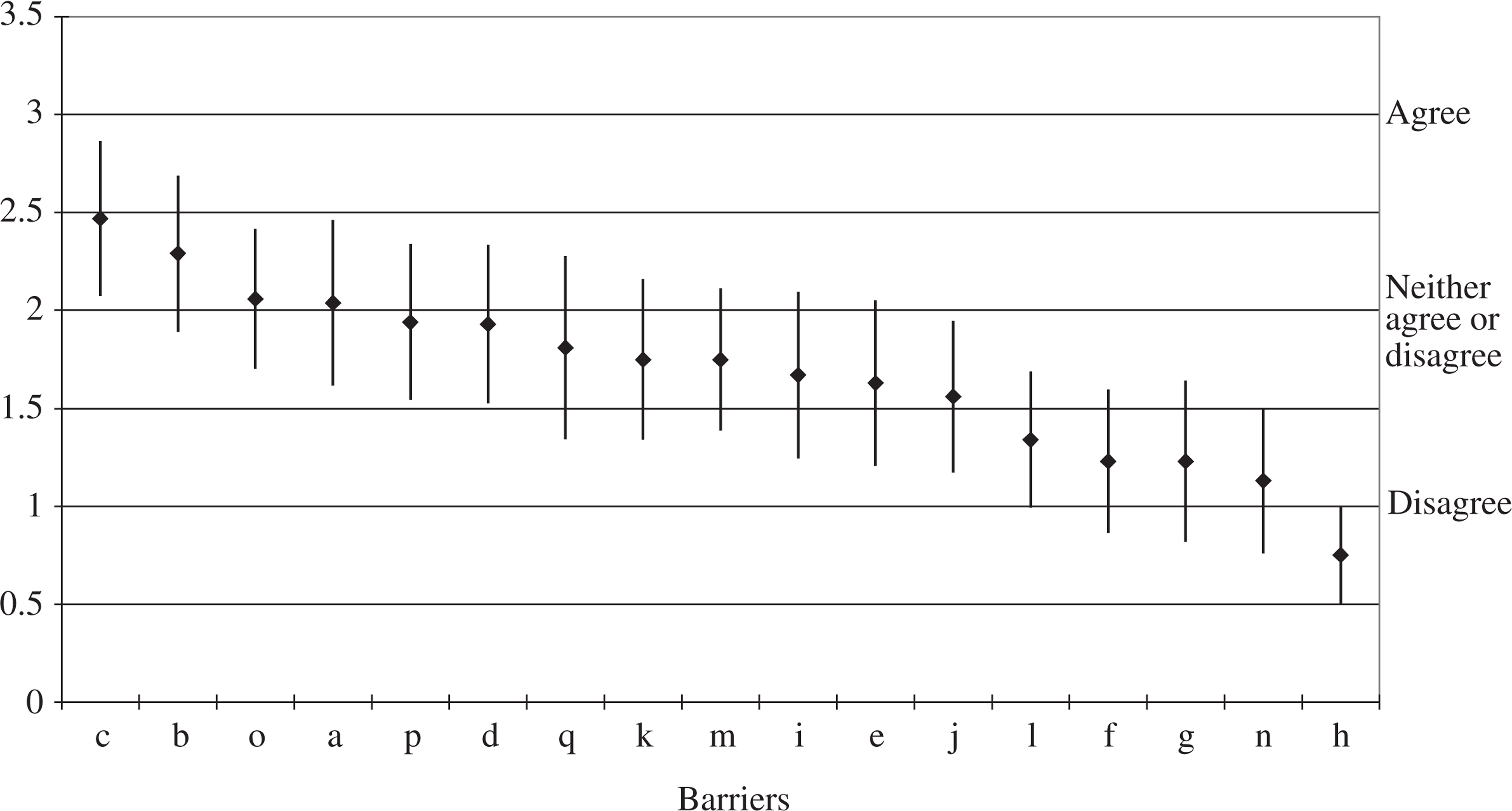
Four groups of responses could be classified when participants were asked to rate barriers. The highest group of items (participants' level of agreement with) were related to the degree of illness and denial that there is an illness (i.e. items c, b). The second group were rated as ‘neither agree nor disagree’ but somewhat ranging down to slightly disagree in relation to a broad range of issues such as accessibility to the child (e.g. distance and transport; items p, o), lack of resources (q), lack of knowledge and skills (k, j, i) and issues to do with patient rapport (m). A third group with means ranging around ‘disagree’ included skills (l), creating a burden on the children (n), not being a problem to the child (f) and issues of time (g). The final and most disagreed with statement (and significantly different to the 12 other barriers) was in relation to not being part of my role to be involved with the child (h). It should also be noted here that confidence interval for this barrier was relatively small indicating similar views across the participants in the study.
Independent t-tests were then undertaken to compare responses from adult mental health professionals with other workers. For three barriers the adult mental health workers responded more agreeably than the other workers. These included items ‘q. Your organization does not have the resources (including time) to involve the children’ t(30) = 2.56 p = 0.02, ‘i. You have limited knowledge about working with children and the issues involved for them’ t(30) = 2.23 p = 0.03 and ‘l. You have limited skills to work with adult clients regarding their children’ t(30) = 2.19 p = 0.04. Also notable given the significant findings regarding knowledge and skill levels of workers (i.e. i and l) was the higher agreement by adult workers on the two other skill and knowledge items ‘k. You have limited skills in working with such children’ and ‘j. You have limited knowledge about working with adult clients regarding the issues for their children (i.e. impact of the problem on children, advising parents regarding parenting issues, etc.)’. Scores for both items were consistent with the scores on i and l above indicating that adult workers have less knowledge and skills in working with parents and their children.
Discussion
Four categories of barriers were identified for workers when responding to patients about parenting and mental illness and to working with children. The first barrier involved the parent's sickness, preoccupation and lack of insight about the mental illness and its subsequent impact on their child/children. The second barrier related to the child in terms of accessibility as well as the workers' perception of the child's unwillingness to engage in discussions regarding his or her parent's mental health. The third group of barriers related to the worker and included a lack of resources and time, not being part of the worker's role (to work with children and/or discuss parenting issues) and a lack of appropriate knowledge and skills regarding children and as well adults and mental illness. These findings support previous research into the barriers of effective service delivery for families affected by parental mental illness [19–23].
While not highlighted by other studies, participants reported a barrier relating to the patient–worker relationship. Workers in the present study considered discussing parenting and child-related issues might result in a disruption to the patient–worker relationship. This finding extends previous research by highlighting the importance of rapport when working with parents who have a mental illness.
Participants in the present study rated the barriers they face working with patients about mental illness, parenting, and to working with children themselves. The most significant barrier for workers is their perception that patients do not recognize their mental health as being a problem for their children and patients denying they have a mental illness at all. Parent's reluctance to associate children with parental mental illness might be due to their fears about the involvement of child protective services [23]. However, it is our contention, that while patients might be reluctant to discuss parenting issues or the impact of their mental illness on their children, workers still need to develop the skills to work sensitively with patients around this issue. Even though some patients might exhibit problematic parenting behaviours, many are open to interventions that enhance their parenting capacity and sense of maternal self-competence [11]. Generally, mothers are more likely to be effective when given the opportunity to take on responsibilities [25] and many consider parenting to be just as important as employment [26] and a valued role in their lives [27]. As it has been argued that the demands and rewards of the care-taking role enhance a mother's motivation to remain in treatment [28], it appears important for adult mental health workers to incorporate a patient's parenting responsibilities into his or her treatment plan. Workers concern about losing rapport and their perception that patients are reluctant to discuss parental mental health issues, demonstrates that workers are struggling to sensitively raise the topic of parental mental, both points which have implications for training and ongoing professional development.
Other notable barriers for workers were related to accessing children (because of transport or being in alternative care). Organizational constraints, including time and resources, were also barriers for effectively working with such families. Finally, it should be noted that there was overall disagreement with the statement ‘It is not part of your role to get involved with the issues of your client's children’. All workers, including adult mental health workers, indicated that it was important to focus on parenting and their patients' child/children as part of their professional role, even though barriers were identified in working effectively with the patient on parenting matters and issues involving his or her children.
There were clear differences between adult mental health workers and other workers in the types of barriers. In comparison to other workers, adult mental health workers reported that their organizations did not have the resources, including time, to involve children. Even though adult mental health workers recognized that the issues involved for the children of their patients were a part of their role, in comparison to other workers, inadequate time and resources were significant barriers. It has been estimated that between 29% and 35% of adult mental health service patients are female with dependent children under the age of 18 years [18]. Thus, while a significant proportion of their patients are parents, adult mental health worker nonetheless identified limited resources and time as significant barriers to working on parenting and child-related issues. Such a finding has important policy implications in terms of time and resource allocation.
Also, in comparison to other workers, adult mental health workers reported limited skills to working with children and when working with adult patients on issues regarding their children (i.e. impact of the problem on the child, advising parents on parenting issues). This is an important finding as it illustrates clear knowledge and skill deficits for this group of critical workers, with direct implications for future training and education development.
Training for adult mental health workers might be considered from two general foci, the first pertaining to the parenting responsibilities of their patient, and second, focusing on the child/children of the parent (patient) with the mental illness. The following summarizes these deficit areas, drawing upon previous research [19–23] and highlighting potential training implications. In terms of knowledge and skill deficits in working with patients who are the parent; assessing for parenting capacity, providing parenting advice and having knowledge regarding the impact of a parent's mental health on family and child functioning would seem to be very important for mental health professionals. Training should focus upon assessing and judging parenting capacity, providing parenting advice and the ability to discuss with patients the impact of a parent's mental illness on his or her children, in an empathic manner. Regarding the children; knowledge and skills in working with children, about child development and the likely impact of the parent's illness at various age and developmental stages are important. Training would then focus upon how to work with children, including how to talk to, and engage with children and include information about child development and the impact of a parent's mental illness on children's development. Finally, such training should aim to enhance workers' skill in providing age-appropriate education to children, about parental mental illness.
Summary, limitations and conclusion
The main barriers for mental health professionals when working with adult patients about their parenting as well as working with their patient's children, was workers' perception that patients did not see their illness as a problem for their children and that patients did not think they had a mental health problem. Significantly, while adult mental health workers acknowledged that a part of their role did involve addressing the issues of the children of their patients and discussing with patients their parenting responsibilities, they reported limited time and resources as well as inadequate knowledge and skill for working with children and with patients about parenting issues.
However, there are also a number of limitations to this study. Most notable is the opportunistic sampling used. Future research would profit from a random sampling of state or an Australia-wide sample of targeted groups of mental health professionals. A further limitation was the failure to measure the level of experience and the amount of time the groups of workers spent working with children. Such an approach would help clarify the amount of time and focus that adult mental health practitioners spend upon family-related matters in their treatment of patients compared to other groups of workers (e.g. child and adolescent professionals). In addition, future studies could consider the specific training needs of other workers, such as general practitioners and child protection workers, who are also in regular contact with families affected by parental mental illness.
Although having some notable limitations, this study has identified the core barriers that impede adult mental health and other workers from working with patients with a mental illness about their parenting and children. More importantly, the study provides valuable information for adult mental health policy-makers, administrators and educators about resource, knowledge and skill shortages among their workers.
Footnotes
Acknowledgements
This paper would not have been possible without the support and input from agencies from the Eastern Health VicChamps program in Melbourne and the Supporting Kids program in the North-east of Victoria, Australia. We would particularly like to thank Melinda Goodyear, Rebecca Alchin, Peter Brann, Rose Cuff, Sheryl Follett, Kirsten Green, Ellen Sharp and Helen Mildred. This research was part of the evaluation of the VicChamps and Supporting Kids projects and was funded by beyondblue: the national depression initiative, Mental Health Branch of the Victorian Department of Human Services and Victorian Health Promotion Foundation (VicHealth). We also thank the mental health professionals who gave their time and knowledge.