
Abstract
Mental illness is associated with a substantial level of disability in terms of personal distress and suffering and disruption in occupational and social functioning. Relapse and chronicity are common, with risk of ongoing morbidity and mortality [1]. The impact of the illness, however, extends beyond the individual sufferer to families in particular to parents as primary care givers. Families are often burdened with having to provide emotional, financial and social support and deal with the emotional, psychosocial and mental health problems arising from their family member's mental illness [2–5].
A common theme in family members, in particular parents, experience of having and caring for a child with a mental illness is that of loss and grief: grief for the loss of the person as known and for the loss of hopes, wishes and aspirations, grief for the disability caused by the illness and the disruption to the family and relationships. This grief is often prolonged, experienced over the course of the illness as the nature, impact and challenges of the illness unfolds and changes. It has been proposed that the very nature and course of mental illness along with its associated disability and life disruption serves as an ongoing source of loss and grief [2–4],[6–10].
Prolonged grief or bereavement has been associated with a variety of mental and physical health consequences, with the bereaved found to have an increased risk of psychological problems and poor physical health [11–13]. Prolonged grief may leave the bereaved susceptible to physical and emotional problems, an hypothesis consistent with the known interrelationship between emotional symptoms, stress and physical health [12], [14], [15]. An important but less researched question is whether the lowered psychological well-being and health status found amongst families whose relatives suffer from a mental illness [16–18] is related to grief.
The nature of familial bonds or relationships plays an important role in the family's emotional and psychological reaction and subsequent adjustment to having and caring for an ill family member. Research has indicated that attachment style may be related to emotion regulation, with secure attachment acting as a buffer against psychological problems and avoidant or anxious/ambivalent styles being potential risk factors for poor coping and maladjustment [19]. More specifically, prolonged or chronic grief has long been thought to result from ambivalent attachment [20], [21].
The first aim of this study was to examine the grief experience of parents of adult children with a mental illness. For the purposes of this study, grief was conceptualized as a cognitive, behavioural and emotional reaction to loss [4], [22], [23]. Dimensions considered to be representative of an individual grieving are a persistence of distress in thinking and talking about the loss and being upset by reminders of the loss [4]. It was anticipated that parents would report experiencing prolonged grief in relation to their child's illness as evidenced by cognitive intrusions, avoidance behaviour, difficulties adapting to and distress associated with reminders of the illness.
The study's second aim was to explore the relationship between parents' grief experience and their health and well-being. It was hypothesized that parents who reported experiencing high levels of grief would also demonstrate reduced psychological well-being and health status.
The third aim of this study was to explore the relationship between parental grief and parent-child attachment and affective relationship. It was hypothesized that parents who reported having a secure attachment relationship with their child would report experiencing a positive affective relationship with their child and lower levels of grief. Conversely a negative affective relationship between parent and child would be related to anxious/ ambivalent or avoidant attachment relationship and higher levels of grief.
Method
Participants
Participants were recruited from a variety of organizations throughout Australia that provide support services for sufferers of mental illness and/or for their families. These organizations either directly distributed information about the research or advertised the study in their newsletter.
The study had 71 participants, 62 mothers and 9 fathers all of whom had a child diagnosed with mental illness. The participants' ages ranged from 42 to 78 years (mean = 57.2 years, SD = 8.69). The participants' children were 52 sons and 19 daughters, whose ages ranged from 18 to 47 years (mean = 28.39, SD = 6.71). The majority of these children suffered from schizophrenia (n = 48); the remainder suffered from bipolar disorder (n = 10), and from schizo-affective disorder (n = 11), while two participants simply stated that their child had other mental illness. The years since initial diagnosis of mental illness ranged from 3 months to 28 years (mean = 6.98, SD = 5.62). Thirtynine percent of participant's children lived with them, 41% lived on their own, 9% with friends or relatives, 7% in group homes and 4% were currently in hospital.
Procedure
Respondents who expressed interest in participating in the study were sent a set of self-report questionnaires, together with an information sheet, a consent form and a stamped addressed envelope in which to return the questionnaires.
Measures
Grief
Grief was assessed using two measures that have been used in previous studies with this population. These measures have applicability to the current conceptualization of grief as involving cognitive intrusions, avoidance behaviour, difficulties adapting to the illness and distress.
The first grief measure used was the Impact of Event Scale (IES) [24]. The IES consists of two subscales, one measures intrusively experienced thoughts and feelings and the other measures consciously recognized avoidance of thoughts, feelings and situations related to a specific event. The IES has been used to measure grief in response to the loss of a child, amongst parents of children with intellectual disability and amongst those whose child has been diagnosed with schizophrenia [4], [22], [25], [26]. The IES has been found to discriminate between the bereaved and non-bereaved [27]. The IES has been reported to have good reliability (r = 0.86), with high levels of internal consistency reported for the subscales (intrusion α = 0.89, avoidance α = 0.82) [24], [27], [28]. The coefficient alphas obtained in the present study were comparable (total scale α = 0.89, intrusion α = 0.88 and avoidance α = 0.78).
The second grief measure employed was the current grief section of the Mental Illness Version of the Texas Inventory of Grief (MIV-TIG) [5]. The MIV-TIG assesses a family member's current levels of grieving in relation to the loss of a healthy young person and to losses related to expectations for the future for that person, which are evidenced by continuing emotional distress, preoccupation with the lost person and an inability to accept the loss. The MIV-TIG has been used in research with parents of children with schizophrenia and with family members of those with mental illness [2], [9]. The reliability of the MIV-TIG is reported to be excellent with an alpha of.92, and a split-half correlation of.89 [5]. The MIV-TIG had comparable reliability (α = 0.92) in the present study.
Health
Psychological and physical health were assessed using the SF 36® health survey which is a self-report, Likert scale examining a patient's perceived health. It consists of 11 questions answered in reference to the previous 4 week period and has been used extensively in population health surveys throughout Australia and both internal consistency and construct validity are reported to be strong [29].
Attachment
Due to the absence of a suitable pre-existing measure of attachment relationship between parent and adult child from a parent's perspective, a scale that was designed to assess attachment style in a romantic relationship, Attachment Style Measure [30] was modified for this study to make it more appropriate for the parent-adult child relationship. The modified items were (i) ‘I find it relatively easy to get close to him/her’; (ii) ‘I'm not very comfortable having to depend on him/her’; (iii) ‘I'm comfortable having him/her depend on me’; (iv) ‘I rarely worry about being abandoned by him/her’; (v) ‘I don't like him/her getting too close to me’; (vi) ‘I'm somewhat uncomfortable being too close to him/her’; (vii) ‘I find it difficult to trust him/her completely’; (viii) ‘I'm nervouswhenever he/she gets too close to me’; (ix) ‘He/she often wants me to be closer than I feel comfortable being’; (x) ‘He/she is often reluctant to get as close as I would like’; (xi) ‘I often worry that he/she doesn't really love me’; (xii) ‘I rarely worry about losing my relationship with him/her’; and (xiii) ‘I often want to be involved in his/her life and this desire sometimes pushes him/her away’.
Before testing the relationship between attachment style and other concepts the internal consistency and factor structure of this modified measure were investigated. An obliminal rotated principal factor analysis was conducted on the measure, with an inspection of the results showing 3 factors with eigenvalues greater than 1.00. The three-factor solution explained 62.1% of the total variance, with the factors accounting for 28.3%, 22.01%, and 11.79% of the variance, respectively. Items 3, 5, 6, 8, 9 were found to load on factor 1 (α = 0.80), items 1, 2, 7, 10 loaded on factor 2 (α = 0.74) and items 4, 11, 12, 13 loaded on factor 3 (α = 0.70). By removing item 3 the reliability of factor 1 was subsequently improved (α = 0.84). An examination of the items that loaded on these factors indicated that factor 1 consisted of items suggestive of an avoidant attachment style, factor 2 consisted of items indicative of an anxious/ambivalent attachment style, while the items in factor 3 suggested a secure attachment style. This factor structure was retained for all further analyses.
Affective relationship
In the absence of a suitable pre-existing measure a scale was designed for the present study to assess the emotional experiences within a parent-adult child relationship. The scale consisted of 14 positively toned and 14 negatively toned emotions. The positive emotions were excited, calm, elated, tender, needed, affectionate, joyful, happy, delighted, satisfied, content, wanted/cared for, loving and relaxed. The negative emotions were angry, rejected, fearful, remote, sad, hostile, indifferent, guilty, worried, alienated, disappointed, overwhelmed, irritated and disgusted. Participants were asked to indicate, on a 7-point Likert scale (1 = never to 7 = very often), how often they experienced each of these emotions in their relationship with their child. The positive and negative items were scored to create two subscales. Cronbach's alpha was 0.88 for both the positive and the negative subscales.
Results
Parental experience of grief
The means, standard deviations and correlations amongst the grief measures and years since diagnosis are presented in Table 1. The avoidance and intrusion scales on the IES were strongly correlated with one another and with the IES total score, and moderately correlated with the MIV-TIG grief scale (rs 0.30 to 0.55). Parents reported experiencing grief in relation to their child's illness as evidenced by intrusive thoughts and feelings and avoidance behaviour (IES) as well as difficulties adapting to and distress associated with reminders of the illness (MIV-TIG). Parental grief was found to be significantly inversely correlated with years since diagnosis. These findings lend support to the notion that mental illness in a child may present a source of grief for parents and that parental grief may reduce over time.
Means, standard deviations and matrix of correlations between grief and years since diagnosis
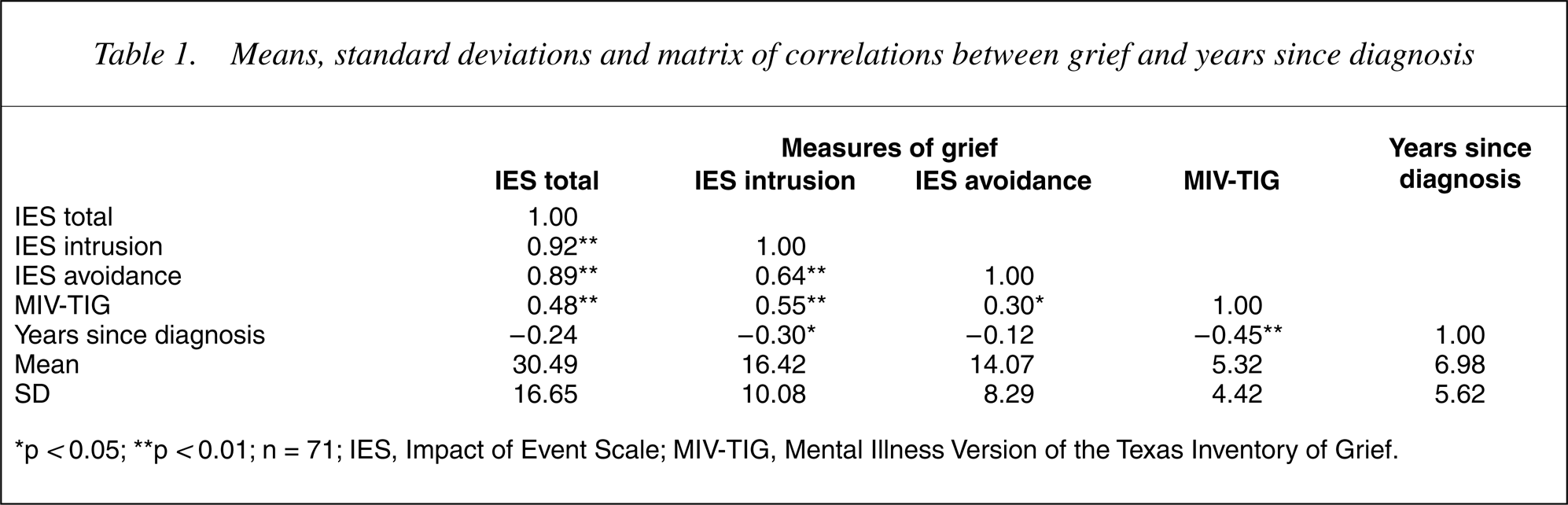
∗p < 0.05; ∗∗p < 0.01; n = 71; IES, Impact of Event Scale; MIV-TIG, Mental Illness Version of the Texas Inventory of Grief.
Despite the obvious limitations of a cross sectional study, in order to examine the question of whether parents of children with mental illness experience prolonged grief, participants were divided into five cohorts dependent upon years since diagnosis of mental illness. The first group comprised 9 parents for whom time since diagnosis was approximately 1 year (mean = 0.66 year, SD = 0.48 years), 11 parents whose child's diagnosis had occurred between 2–3 years (mean = 2.64 years, SD = 0.59 years), 19 parents for whom the diagnosis had been made between 4–5 years (mean = 4.66 years, SD = 0.58 years), 19 parents for whom the diagnosis had been made between 6–10 years earlier (mean = 8.21 years, SD = 1.55 years), and 13 parents for whom time since diagnosis was more than 10 years (mean = 16.62 years, SD = 4.57 years).
A series of one-way analyses of variance (ANOVAs) were conducted between these five groups and the grief measures in order to examine parental grief experience across the five cohorts. The trend across the groups (see Fig. 1) appears to show heightened grief in the first year post-diagnosis followed by a reduction in grief during the 3 years postdiagnosis and then an increase again in grief levels to the fifth year, proceeded by a gradual reduction in grief levels over time then after. Despite this obvious trend only parents who had a child recently diagnosed with mental illness (i.e. approximately 1 year) reported experiencing significantly more grief in particular intrusive thoughts and feelings (IES) than parents who have been caring for a child with a mental illness for more than 10 years (F4,66 = 3.32, p < 0.05). Significant differences were found between the groups on MIV-TIG grief scores (F4,66 = 5.12, p < 0.01). Post hoc testing (Tukey's critical distance p < 0.05) revealed that levels of parental grieving, as measured by the MIV-TIG, in the cohort of parents approximately 1 year post-diagnosis and cohort of parents 4–5 years post diagnosis were significantly differentiated from those at more than 10 years post diagnosis (see Fig. 1). Levels of grief reported by cohort of parents from the first year to 10 years post-diagnosis were not significantly differentiated from each other. These results need to be interpreted with caution due to small and unequal group sizes.
Mean grief scores of groups according to years since diagnosis. n = 71.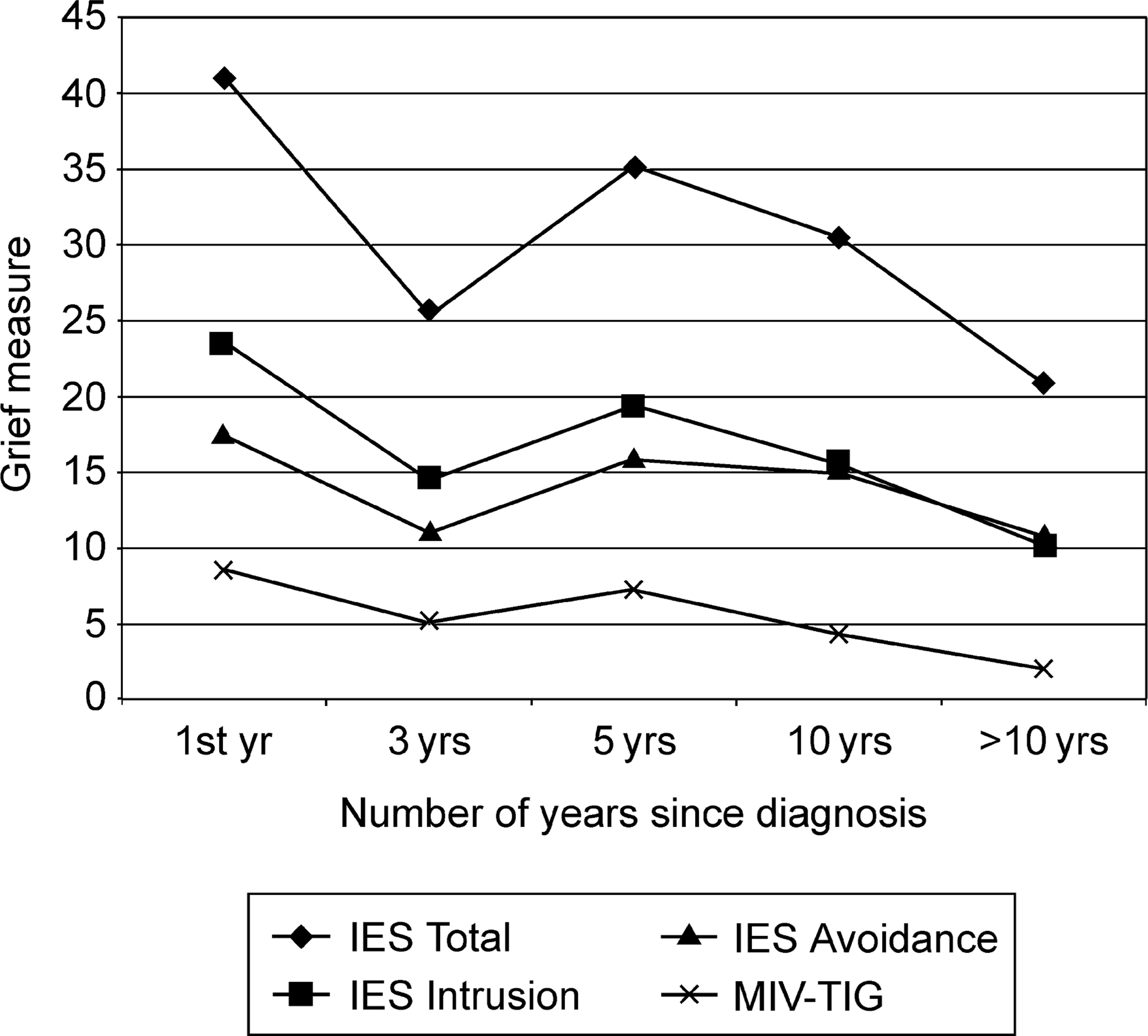
Parental grief and health and well-being
Correlational analyses were conducted to determine the relationship among parental grief and subjective health variables (see Table 2). The total health score, physical health summary score and psychological health summary scores were significantly inversely correlated with grief measures. A significant positive correlation was found between the concept of health transition and all grief measures, indicating that grief was associated with a deterioration in perceived health over the previous 12-month period. Significant inverse correlations were found between all other health concepts and all grief measures with the exception of physical functioning, which was inversely correlated only with MIV-TIG grief. These results indicate that parents who are experiencing grief in relation to their child's mental illness have reduced levels of health and well-being.
Correlations between grief and health measures
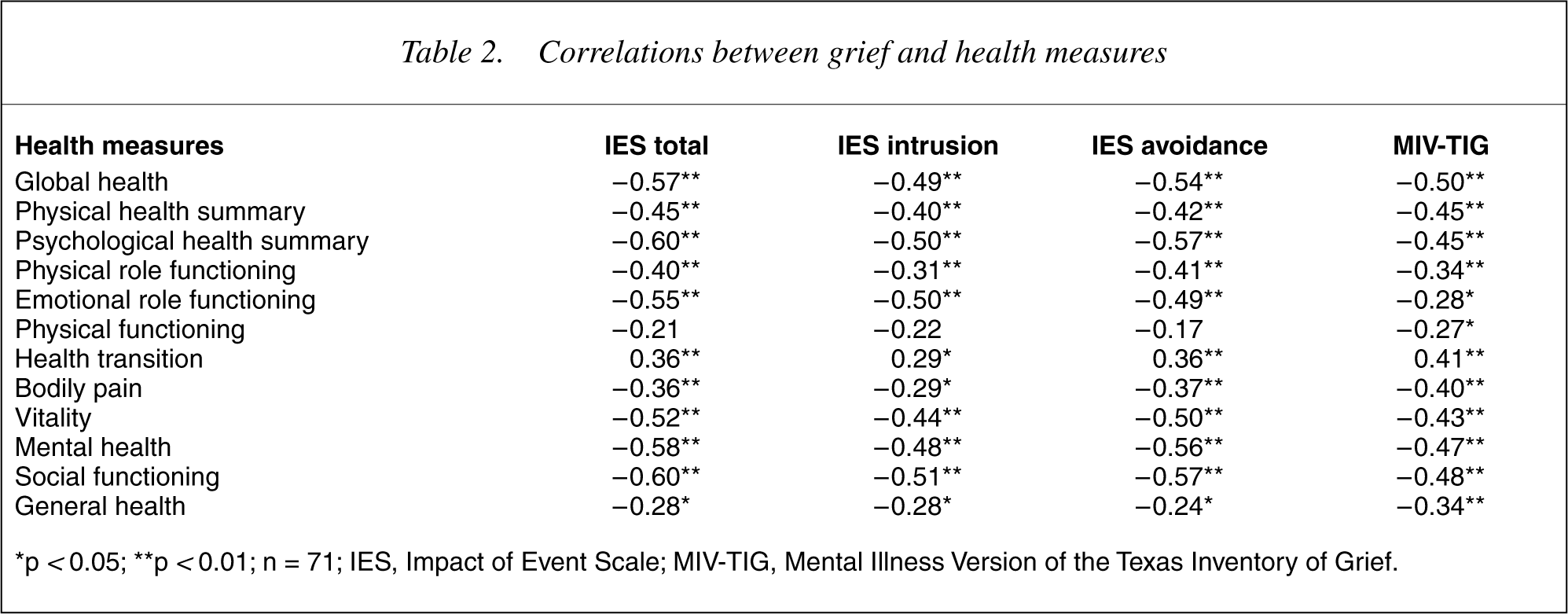
∗p < 0.05; ∗∗p < 0.01; n = 71; IES, Impact of Event Scale; MIV-TIG, Mental Illness Version of the Texas Inventory of Grief.
Parental grief, attachment and affective relationship
The correlations between grief and attachment and affective relationship are presented in Table 3. As hypothesized a secure attachment relationship between the parent and child was found to be related to lower levels of grief and a greater positive affective relationship. Conversely, an anxious/ambivalent attachment relationship was significantly related to greater grief and negative affect in the relationship. An avoidant parent-child attachment relationship was significantly correlated with the IES avoidant subscale, a grief measure of a tendency to avoid thoughts or feelings related to the child and his/her illness. It was not related to either an overly negative or positive affective relationship.
Correlations between grief, attachment and affective relationship
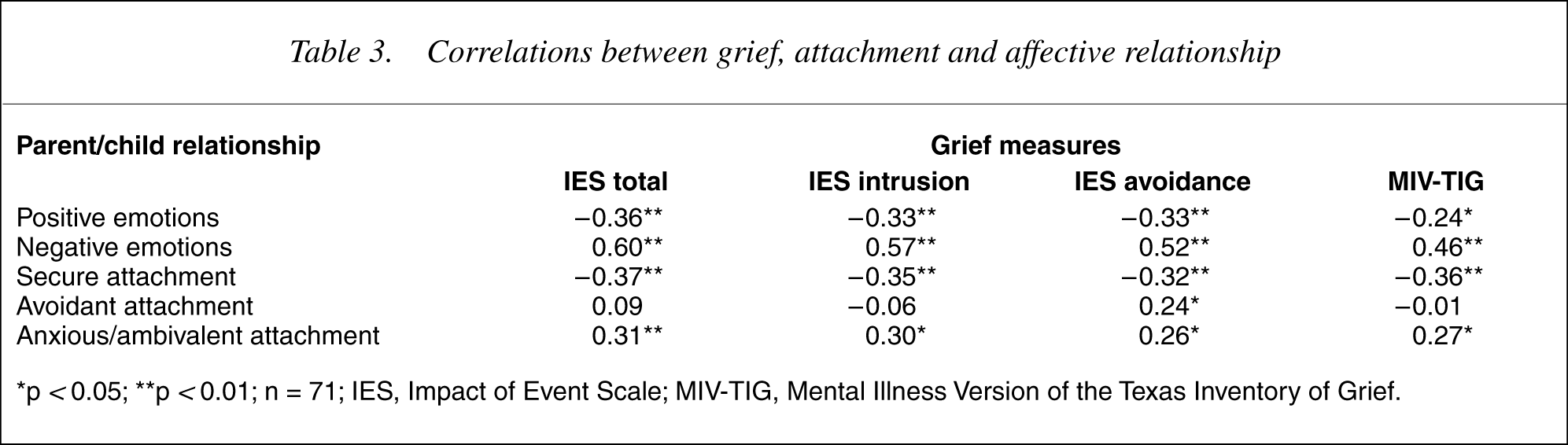
∗p < 0.05; ∗∗p <0.01; n = 71; IES, Impact of Event Scale; MIV-TIG, Mental Illness Version of the Texas Inventory of Grief.
Discussion
The onset of a mental illness is associated with a great deal of emotional distress and life disruption for the identified sufferer and the family. Grief appears to be a normal and adaptive response in family members to the myriad of perceived losses arising from the nature of the illness, the disability it causes and the negative impact it has on family processes and resources.
The present study extends previous work that has attempted to understand the nature and process of parental grief in response to having and caring for a child with a mental illness. The study demonstrated that parents of children with a mental illness do experience significant levels of grief, as characterized by continuing emotional distress, preoccupation with the ill child, difficulties adjusting to the loss, the experience of intrusive thoughts and feelings and active attempts to avoid thoughts and feelings relating to the child and his/her illness. Although a longitudinal study is best suited to examining parental grief and its change over the course of time, the findings appear to support a reduction in parental grief over time, but only in some aspects of grief and after an extended period. It is not only suggestive of prolonged grief but is supportive of the notion that parental grief may be different across the life course of the illness possibly reflecting the different challenges, issues and impacts of the illness as well as parental adjustment to having and caring for a child with an illness. Factors that make it difficult for caregivers to assimilate the totality of the loss thereby complicating and prolonging the task of grieving include the occurrence of unanticipated losses, the absence of a clear lost object for parents to mourn and no finality to their loss and the changing representation of the loss over time [4], [5], [7], [9], [10], [21], [31].
In previous independent research lowered psychological well-being and health status had been demonstrated in the bereaved and amongst families of suffers of mental illness. The later relationship was often associated with the burden of caregiving [18]. The findings of the current study lend support for the hypothesis that lowered psychological well-being found in parents of people with a mental illness may be related to the process of grieving. Parents who reported greater levels of grief also reported greater levels of emotional distress and lower levels of psychological well-being and health status.
Affectional bonds, in particular the parent-child attachment, play an important role in human development. The onset of a mental illness and subsequent difficulties in caring for an ill family member presents a major challenge for the family as it places a strain on family processes and resources. Ruptures in these relationships are likely to cause great emotional distress [32]. Parents who reported having secure affectional bonds reported experiencing greater positive affective relationship with their child and lower levels of grief. On the other hand parents who reported having an anxious ambivalent relationship with their child reported greater negative affective relationship and greater grief. These findings provide support for the proposition that a secure parent-child attachment may act as a buffer against psychological problems where as an anxious/ambivalent relationship may be lead to a greater risk of prolonged grief [20], [21], [33]. An avoidant parent-child attachment relationship, characterized by discomfort with being close, tendency to not seek love and support from others and to remain emotionally detached [30], [34], was found to be related to a tendency to avoid thoughts and feelings related to the child and his/her illness and to a detached affective relationship.
There are two general limitations to this study. Firstly the measures of attachment and affective relationship that were modified, or designed for this study, require further exploration in order to establish their reliability and validity. Secondly the generalisability of the results is limited, owing to the self-selected nature of the subjects who were predominantly self-help support group members, and as such may differ on key measurements of grief and adjustment. Recruitment of representative samples is a problem for researchers generally and particularly problematic in grief studies due to the sensitivity of the subjects under study [11].
The current study has a number of implications for future research and grief work with families. There is a clear need to undertake further research, in particular longitudinal research, into parental grief and adjustment. Research that assists in being able to define healthy versus unhealthy adjustment, identify factors that facilitate or hamper grief work as well as factors that are predictive of good versus poor adjustment is vital. Research into these processes will assist in being able to clarify if, when and how best to provide care for caregivers.
In conclusion, this study provides important insights into the grief experiences of parents following their child's diagnosis with mental illness. The significant relationship between parental grief and parental psychological well-being and health status has important implications for health professionals. Foremost amongst these are the need to validate the distress and grief of parents and to better understand how to provide interventions that promote grief work and reduce emotional distress and life disruption.
Footnotes
Acknowledgements
We thank the parents who shared their experiences with us and to the various organizations that supported the project, including Association of Relatives and Friends of the Mentally Ill, Mental Health Association NSW, The Schizophrenia Fellowship, Richmond Fellowship, ACT Carers Association, ACT Mental Health Branch and Southern Area Mental Health Service.