
Abstract
Background:
Children of parents with mental illness face a number of adversities, potentially contributing to poor health.
Aim:
The aim of this study was to quantify the association between maternal severe mental illness and children’s hospital admissions.
Method:
Record linkage cohort study of 467,945 children born in Western Australia between 1 January 1980 and 31 December 2001. Follow-up was from age 28 days until fifth birthday. Linked registers captured information on potential confounders. Rate ratios and adjusted rate ratios measured relative change in the numbers of admissions and total days of stay, while rate differences measured absolute change in outcomes. Cause-specific increases were calculated for ICD-9 chapters and for ‘potentially preventable’ conditions.
Results:
After adjusting for potential confounders, children of mothers with severe mental illness had a 46% relative increased rate in hospital admissions (95% confidence interval = [38%, 54%]) and an absolute increase in 0.69 extra days in hospital per child, per year (95% confidence interval = [0.67, 0.70]). The relative increase in admissions was greatest in the child’s first year of life (adjusted rate ratio = 1.76, 95% confidence interval = [1.64, 1.88]; rate difference = 0.32, 95% confidence interval = [0.30, 0.34]). Rates of admissions were increased for a range of causes, particularly injuries, infections and respiratory disease, and for conditions classified as ‘potentially preventable’.
Conclusion:
Children of mothers with severe mental illness have a substantial excess in hospital use compared to children of well mothers. This vulnerable group should be targeted with interventions to avert preventable morbidity and premature mortality in later life.
Introduction
Children whose mothers have a severe mental illness (SMI), such as schizophrenia, represent a sizable population of vulnerable children (Abel et al., 2019; Pierce et al., 2020). Not only are they more likely to live in poverty (Abel et al., 2019; Pierce et al., 2020) but recent evidence also shows they are at heightened risk of a range of adverse health outcomes, including exposure to serious obstetric complications (Jablensky et al., 2005), premature mortality (Di Prinzio et al., 2020; Webb et al., 2006), neuropsychiatric and neurodevelopmental problems (Di Prinzio et al., 2018) and greater risk of physical illness (Nevriana et al., 2020; Pierce et al., 2019).
We know these children often live in families subject to multiple deprivation (Pierce et al., 2020); therefore, access to healthcare, including preventive interventions, is likely to be an important piece of the puzzle linking parental mental illness to observed poorer health in their children. However, little information exists about whether or how these children use healthcare systems. Such information is important: (1) because excess healthcare utilisation implies greater underlying morbidity in this group; (2) if policymakers and service providers are to optimise the cost-effectiveness of their services, they need to maximise access by planning for and targeting them to those most in need. Poor physical health may lead to poorer quality of life and hinder a child’s development; significant differences in health utilisation in this population represent a potentially important marker of their health and well-being warranting further investigation.
Existing studies have focussed on maternal depression (Guttmann et al., 2004; Lyngsøe et al., 2018; Sills et al., 2007; Ververs et al., 2009). One recent registry study from Denmark (Ranning et al., 2019) compared the incidence of admissions for somatic morbidity from birth up to age 30 years for 47,000 people exposed to parental schizophrenia or affective disorders and 1.7 million controls. They reported increased hospital admissions in offspring for almost all categories of physical disorder studied, with the exception of cancer.
We undertook the first study in Australia of healthcare utilisation among children of mothers with SMI using the Western Australian high-risk e-Cohort (Morgan et al., 2011). We focused our analysis on the first 5 years of life (excluding the already-investigated perinatal period), thus providing information during a crucial period of development. Our primary hypothesis was that the children of mothers with SMI would have an excess number of hospital admissions and days spent in hospital compared to the children of mothers with no history of mental health contact. We investigated absolute and relative differences in hospital admissions and explored whether any excesses varied by sex or by age; we also examined specifically which illnesses contributed to any excess.
Methods
Data
This retrospective cohort study was drawn from 467,945 children in the Western Australian high-risk e-Cohort (Morgan et al., 2011). This cohort covers children born in Western Australia between 1 January 1980 and 31 December 2001, recorded in the Midwives Notification System (MNS; Gee and Dawes, 1994). This dataset includes mandatory, prospectively collected data on all infants born in Western Australia, not restricted to live births. Mothers with SMI were identified through linkage, in December 2002, to the Hospital Morbidity Data Collection and Mental Health Information System. These cover all public and private inpatient hospital admissions, and public outpatient and ambulatory care contacts with mental health services across the State, dating back to July 1966. Comparison children were those of mothers with no mental illness on the Hospital Morbidity Data Collection and Mental Health Information System. Children with mothers with mental illnesses other than SMI were not available for this linkage.
Child hospital admissions up to 31 December 2006 were determined from the Hospital Morbidity Data Collection linked to the MNS. Linkage was carried out by the Data Linkage Branch of the Western Australian Department of Health. Further details on the high-risk e-Cohort are available in Morgan et al. (2011).
The cohort for this analysis excluded children who were above the age of 5 years when their mother was diagnosed with an SMI (N = 7156) and children stillborn or who died in the neonatal period (N = 5056). The analysis cohort therefore consisted of 455,713 children. Children were followed-up from 28 days until death or their fifth birthday (whichever occurred earlier).
Exposure
Exposure to maternal SMI was defined using an iterative algorithm based on the most recent diagnosis in psychiatric records to determine the presence of an the presence of an SMI code according to the International Classification of Disease 9th edition (ICD-9; World Health Orgainzation, 1977). Diagnoses were identified using ICD-9 categories for schizophrenia (ICD-9: 295), bipolar disorder (296.0, 296.2–296.5), unipolar major depression (296.1, 296.6, 296.8, 296.9), paranoid states (297 – all) and other nonorganic psychoses (298 – all). ICD-8 and ICD-10 equivalents used in a small number of records were mapped to ICD-9. The concurrent validity of register diagnoses of schizophrenia and affective psychoses based on the algorithm used has been evaluated against an independent sample assessed using a semi-structured diagnostic interview (Castle et al., 2006) with sensitivity of 0.92 and specificity of 0.88 for schizophrenia and 0.80 and 0.90, respectively, for affective psychoses (Jablensky et al., 2005).
Children were defined as exposed to maternal SMI from the date of their mother’s first relevant recorded diagnosis up to age 5 years and unexposed prior to this date. Children born to a mother with no psychiatric contact history were consistently defined as unexposed.
Outcome
There were two measures of healthcare utilisation: (1) the rate of child admissions to inpatient care, per child per year and (2) the number of days the child spent in inpatient care, expressed as the rate of days per child per year.
We also explored the primary diagnosis associated with inpatient admissions. These were classified according to ICD-9 chapters, excluding congenital anomalies and diseases originating in the perinatal period as these have been covered in previous analysis (Di Prinzio et al., 2020). We included a separate category of ‘potentially preventable’ conditions, using the definition provided by the Australian Institute of Health and Welfare (2018): potentially preventable conditions include the following: (1) Chronic conditions – these conditions may be preventable not only through lifestyle change but can also be managed effectively through timely care (usually non-hospital) to prevent deterioration and hospitalisation; (2) Acute conditions – these conditions may not be preventable but theoretically would not result in hospitalisation if timely and adequate care (usually non-hospital) was received and (3) Vaccine-preventable conditions – these conditions may be preventable through vaccination.
Covariates
Data on maternal age and marital status, and sex and birth order of the child were extracted from the Midwives Notification of Births. Data were collected on Indigenous status (Aboriginal or Torres Strait Islander descent) in any of the data sources available in the e-Cohort. Socio-economic status (SES) at birth was determined using an area-level measure derived by the Australian Bureau of Statistics (2008). Urbanicity of the mother’s residence at the time of the child’s birth was determined based on a census-derived area-level measure (Australian Bureau of Statistics, 2006). Maternal and paternal place of birth and paternal age at child’s birth were extracted from birth registration records. A binary variable, father unknown, indicating whether the name of the child’s father was registered on the child’s birth record, was included. Paternal psychiatric morbidity was ascertained through mental health inpatient admissions and ambulatory/outpatient contacts.
Statistical analysis
Counts and percentages were used to describe demographic characteristics of the cohort. Unadjusted Poisson regression analyses modelled associations between exposure to maternal SMI and (1) rates of hospital admissions and (2) rates of total days admitted, for a child between ages 28 days and 5 years and separately for each year of follow-up. Unadjusted absolute rate differences (RDs) and relative rate ratios (RRs) were determined. Adjusted rate ratios (aRR) were then calculated by adjusting for the potential confounders of sex, order of birth, child Indigenous status, paternal mental health status, urbanicity, area-level socio-economic indicator, maternal marital status, maternal and paternal age at the time of child’s birth, maternal and paternal place of birth.
Only children alive at the beginning of an age group were included in analysis for that period. Children with a missing covariate were retained in analyses by including ‘missing’ categories for relevant variables. Levels of missing data were low and were not considered to introduce any bias. Standard errors were adjusted to account for clustering between maternal sibships using the sandwich estimator. Analyses were carried out using Stata v13.
This study was approved by the Western Australian Department of Health Human Research Ethics Committee (2011/75) and the University of Western Australia Human Research Ethics Committee (RA/4/1/1322).
Results
Cohort characteristics
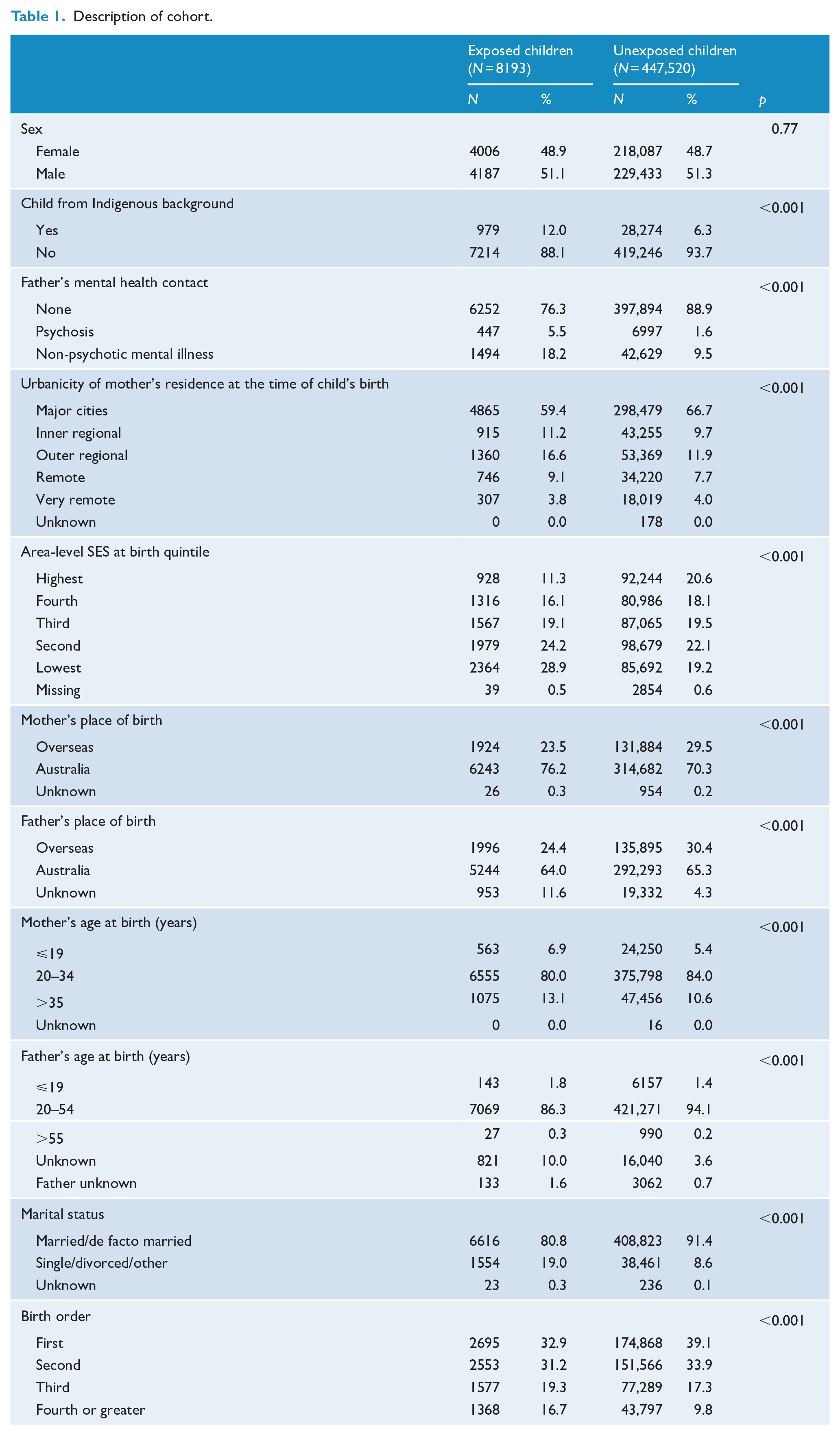
Demographic characteristics of the children appear in Table 1. Overall, 1.8% (8193/455,713) of children were exposed to maternal SMI up to age 5 years. Compared to unexposed children, exposed children were more likely to be from an Indigenous background (12% vs 6%), to have older siblings (67% vs 61%) and to live outside of major cities (41% vs 33%). Exposed children were more likely to have a father who had a mental illness (24% vs 11%), to have a mother who was unpartnered (21% vs 9%) and a mother or father who was younger than 20 years at birth (7% vs 5% for mothers, 2% vs 1% for fathers).
Description of cohort.
Admissions to hospital
Children with maternal SMI had a 70% greater relative rate of admissions compared to unexposed children (95% confidence interval [CI] = [61%, 80%]; Table 2). Once this was adjusted for potential confounders, the increase was 44% (95% CI = [37%, 53%]). In absolute terms, there were 0.13 more admissions per child, per year among those with maternal SMI compared to those without (95% CI = [0.13, 0.15]).
Rate of hospital admissions per year of exposed (N = 8173) and unexposed children (N = 447,520).
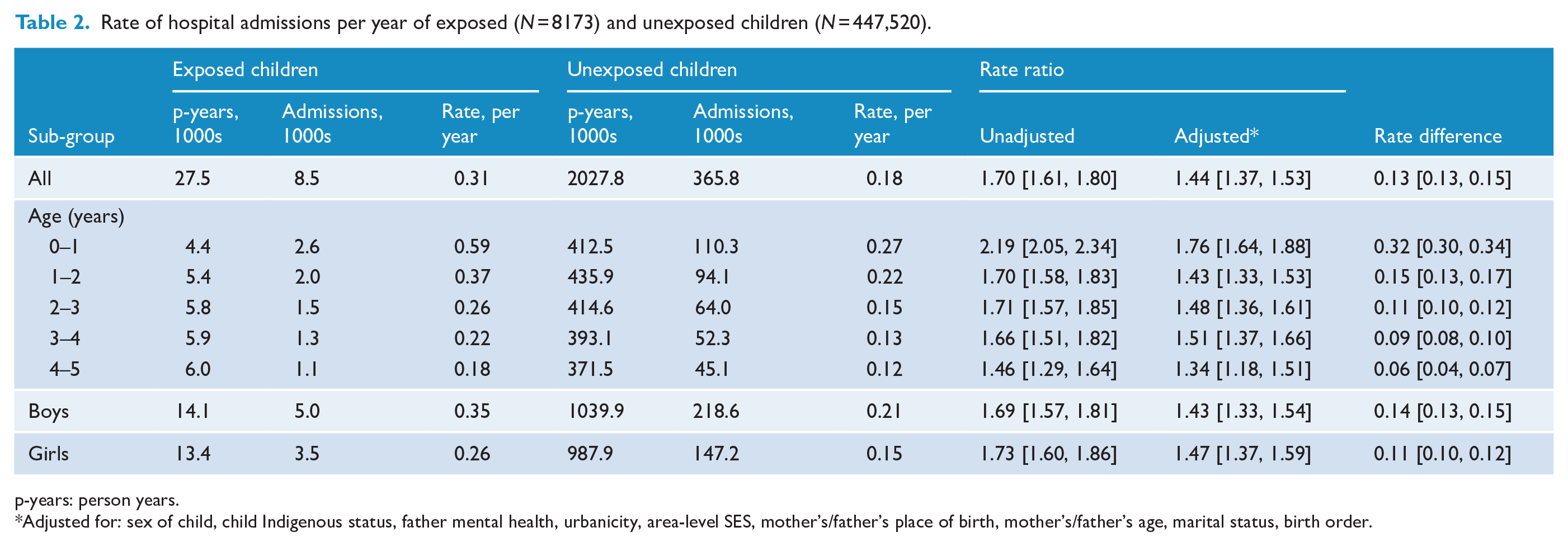
p-years: person years.
Adjusted for: sex of child, child Indigenous status, father mental health, urbanicity, area-level SES, mother’s/father’s place of birth, mother’s/father’s age, marital status, birth order.
The increase in admissions associated with maternal SMI was greatest in the child’s first year of life (aRR = 1.76, 95% CI = [1.64, 1.88]; RD = 0.32, 95% CI = [0.30, 0.34]). The increase reduced with age (e.g. aRR = 1.34, 95% CI = [1.18, 1.51] in Years 4–5). There was a marginally larger absolute increase in admissions for boys than girls (RD for boys = 0.14, 95% CI = [0.13, 0.15]; RD for girls = 0.11, 95% CI = [0.10, 0.12]).
Days in hospital
Children exposed to maternal SMI spent an average of 1.34 days, per year in hospital compared to 0.68 in those unexposed (Table 3). This translated to 0.66 extra days per year for those with maternal SMI (95% CI = [0.64, 0.67]). After adjusting for potential confounders, there were 51% more days spent in hospital, by children exposed to maternal SMI compared to those unexposed. The relative and absolute increase associated with maternal SMI was greatest in the first year of life (aRR = 1.93, 95% CI = [1.73, 2.16]; RD = 2.33, 95% CI = [2.27, 2.38]) and the absolute increase was greater for boys (RD boys = 0.74, 95% CI = [0.72, 0.76]; RD girls = 0.57, 95% CI = [0.55, 0.59]).
Rate of number of days spent in hospital per year of exposed (N = 8173) and unexposed children (N = 447,520).
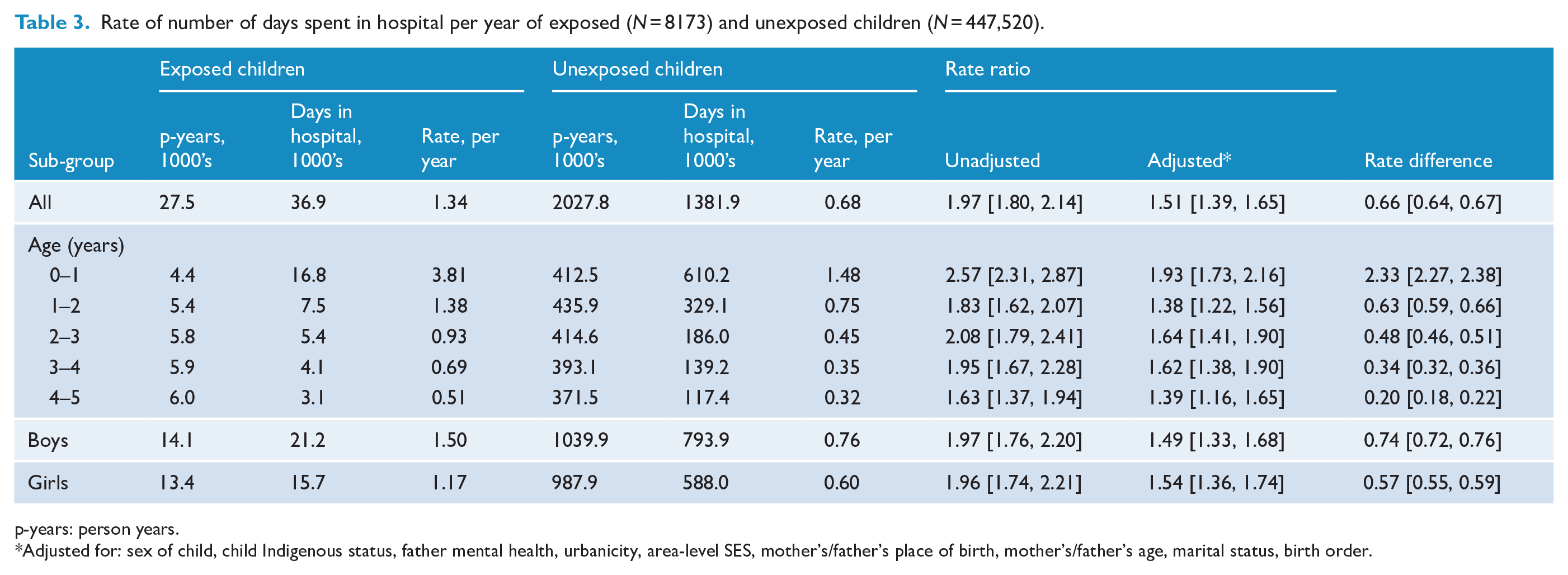
p-years: person years.
Adjusted for: sex of child, child Indigenous status, father mental health, urbanicity, area-level SES, mother’s/father’s place of birth, mother’s/father’s age, marital status, birth order.
Admission for specific diagnoses
After adjusting for confounders, there was a 40% increased rate of admissions for diseases considered potentially preventable (95% CI = [31%, 51%]; Table 4). There was good evidence of a higher rate of admissions associated with maternal SMI for the categories of mental disorders (aRR = 3.95, 95% CI = [2.82, 5.53]); injuries and poisonings (aRR = 1.58, 95% CI = [1.46, 1.70]); infections (aRR = 1.36, 95% CI = [1.28, 1.45]); respiratory system diseases (aRR = 1.35, 95% CI = [1.20, 1.51]); nervous system and sense organs diseases (aRR = 1.30, 95% CI = [1.18, 1.43]) and digestive system diseases (aRR = 1.22, 95% CI = [1.11, 1.33]). There was evidence for a small increase in the rate of admissions for diseases of the genitourinary system (aRR = 1.19, 95% CI = [1.03, 1.38]) and skin and subcutaneous tissue (aRR = 1.18, 95% CI = [1.00, 1.40]). There was an increase observed for cancers (aRR = 1.94, 95% CI = [0.87, 4.36]) and endocrine diseases (aRR = 1.38, 95% CI = [0.86, 2.23]), however neither reached statistical significance. There was no increase observed for diseases of blood or the circulatory system.
Rate of Hospital admissions for specific diagnosis, comparison of children with parental SMI with unexposed children.
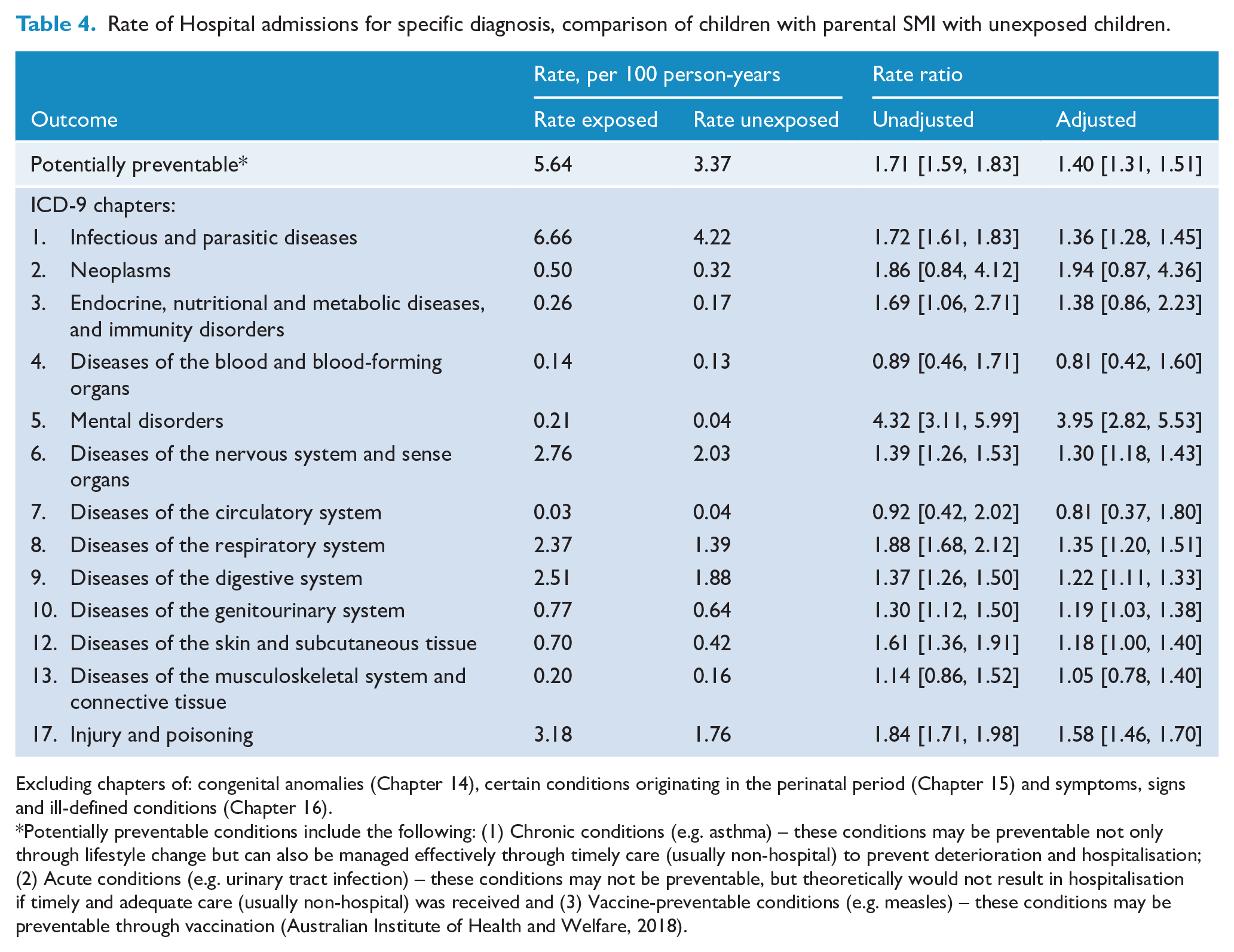
Excluding chapters of: congenital anomalies (Chapter 14), certain conditions originating in the perinatal period (Chapter 15) and symptoms, signs and ill-defined conditions (Chapter 16).
Potentially preventable conditions include the following: (1) Chronic conditions (e.g. asthma) – these conditions may be preventable not only through lifestyle change but can also be managed effectively through timely care (usually non-hospital) to prevent deterioration and hospitalisation; (2) Acute conditions (e.g. urinary tract infection) – these conditions may not be preventable, but theoretically would not result in hospitalisation if timely and adequate care (usually non-hospital) was received and (3) Vaccine-preventable conditions (e.g. measles) – these conditions may be preventable through vaccination (Australian Institute of Health and Welfare, 2018).
Discussion
Main findings
In the first analysis of its kind in Australia, we describe substantial excess inpatient admissions and days in hospital associated with having a mother with an SMI. Children (aged 0–5 years) with maternal SMI had an average increase in 0.13 new hospital admissions and 0.66 days in hospital per year compared to unexposed children. The increase was greatest in the first year of life, where we report a relative increase in 76% more admissions and an absolute increase in 2.33 more days spent in hospital. The association between SMI and hospital inpatient admissions persisted when we adjusted for a range of factors both associated with SMI and considered as risk factors for child morbidity (e.g. being from an Indigenous background, living in lower socio-economic neighbourhoods). This leads us to consider that the association might be a causal effect from SMI to childhood morbidity; however, given the observational nature of this research, this cannot be confirmed.
The association between maternal SMI and healthcare use was non-specific for a particular childhood illness; rather it was observed for a large range of diseases but, notably, was largest for mental disorders (primarily emotional disturbances and developmental delays), injuries, infections and respiratory diseases. After adjusting for potential confounders, there was evidence of a 40% increase in potentially preventable causes of hospital admission. The findings point to an underlying vulnerability in children with maternal SMI. This vulnerability may include genetic, and environmental, effects from having a mother with SMI that influence the risk of childhood physical illness and subsequent hospital admission. High comorbidity between mental and physical disorders is well-described, especially in adults (Nordentoft et al., 2013), and potential genetic pathways have been identified (Zhang et al., 2021). Notwithstanding, clinical teams should consider this additional risk in individual children and consider whether they or their families might benefit from targeted interventions.
Comparison with literature
We confirm a higher rate of child hospital admission associated with maternal SMI, as has been reported for the children of mothers with depression (Guttmann et al., 2004; Lyngsøe et al., 2018; Sills et al., 2007; Ververs et al., 2009). A recent Danish registry study (Ranning et al., 2019) also saw a similar increased risk of offspring hospital admissions associated with parental SMI for a wide range of causes, although the effect estimates reported here are generally larger (e.g. infectious and parasitic diseases RR = 1.36 vs incidence RR = 1.18). This difference might be because our study calculated the estimate based on repeated events, not just the first; and there could be a greater effect of SMI on subsequent events. Also, the Danish study was able to include paternal SMI in their definition and the effects of mothers on health are generally larger than that of fathers (Pierce et al., 2019); not least because of maternal influences on intrauterine growth, an important predictor of subsequent health (Salam et al., 2014). Finally, in Denmark, it could be that the effect of parental SMI is mediated by a strong social welfare system that might act to ameliorate some of the effects that parental mental illness has on SES (Pierce et al., 2020).
This study corroborates our recent systematic review (Pierce et al., 2019) that reported an increased risk of poor physical health in children with parental mental illness. Other studies have demonstrated that children with parental mental illness are at increased risk of poor birth outcomes, including obstetric complications (Jablensky et al., 2005), pre-term birth (Nilsson et al., 2002) and low birthweight (Abel et al., 2010). This could help explain why we reported the greatest relative increase in the children’s first year.
Strengths
This study has a number of strengths. First, we used population-based registers so we were able to draw on a relatively large, prospectively collected dataset that provided sufficient statistical power to investigate the rare exposure of maternal SMI. Second, because the sample is population-based, it has excellent generalisability. Third, the use of registry data means few were lost to follow-up. The notable exception for this is where a family moved from Western Australia because we did not have records of out-migration. We used a limited follow-up of 5 years to mitigate this. However, Western Australia has one of the lowest levels of out-migration of all the Australian states (Morgan et al., 2011), and there is no reason to assume out-migration would have introduced a systematic bias. The fourth strength of this study was the use of multiple linked registers that permitted access to a wide range of covariates, allowing for good covariate adjustment.
Limitations
Notwithstanding, this study has several limitations. First, because our outcome is children’s hospital admissions, we are likely only to capture more severe health events compared with primary care data. This is consistent with evidence suggesting maternal mental illness is associated with increased risk of primary care and outpatient healthcare utilisation; however, there is also evidence that their children access less preventive healthcare (Logan et al., 2008; Minkovitz, 2005). Second, data were not available on important potential confounders; for example, there was no information on maternal smoking, maternal use of medications and neighbourhood pollution. In addition, some of the variables collected may be poor measures of the underlying confounding mechanism (e.g. we only had access to area-level SES rather than individual measures of deprivation). The confounders collected resulted in a slight attenuation of effect, particularly child’s indigenous status and it is likely that further confounders may have attenuated the estimate further.
Third, the proportion of those with maternal SMI (1.8%) was considerably lower than the proportion of those with maternal mental illness in general estimated from other studies (Abel et al., 2019; Pierce et al., 2020). This is because our definition of mental illness included only those admitted to secondary care and excluded those with other types of mental illness, for example, personality disorder and, therefore, this limits the generalisability of the results. Finally, our classification of mothers with SMI was based on a history of psychiatric contact up to the end of 2002. We expect that some comparison children born in the later years of the cohort would have mothers who went on to develop a mental illness after this time. This would result in some misclassification of our exposure, and our results may, therefore, be biased towards a more conservative value.
Meaning of results
This study further demonstrates that there are risks to children with maternal SMI beyond those previously reported for poor birth outcomes and psychiatric morbidity. Poor physical health in childhood is an important component of lifelong health, into adulthood (National Scientific Council on the Developing Child, 2020). There will also be other implications: prolonged time in hospital might affect school attainment or worsen parental mental health.
Children with parental mental illness have been shown to be at a reduced likelihood of receiving vaccinations than unexposed children (Osam et al., 2020; Ozkaya et al., 2010) and, while this is unlikely to explain the current findings, it does show that such children access preventive healthcare less frequently and, therefore, might present only when their symptoms are sufficiently serious. Therefore, the health of these children could be improved if there is more focused targeting of public health messages to this group. Also, because of the clear link between parental mental illness and low SES (Fitzsimons et al., 2017; Pierce et al., 2020), we might expect that much of the effect of parental mental illness is mediated through poverty and deprivation. This would suggest a target for intervention and that lifting these children out of poverty would improve their health. Further research could investigate how the age of the child at maternal mental illness onset and severity of parental mental illness might influence the health of the child.
Conclusion
This study demonstrates that the link between mental and physical health is not restricted to the individual, but that it crosses generations. This adds weight to the argument that we should focus greater attention on common aetiologies between physical and mental disorders, especially in families. Increasingly, cohorts used for epidemiological association studies will include genotypes for complex outcomes. When these data are available, it encourages us to consider epidemiological designs using genetic and environmental measures across generations (Jami et al., 2021). Understanding the determinants of health in children by examining their early life experiences should include the mental health of their parents. This will help us develop our biological understanding of the mechanisms underpinning morbidity and multimorbidity. Timely interventions aimed at the right children and their parents will benefit individuals and lead to efficiencies in healthcare systems as chronic and preventable diseases are averted. Not doing so will lead to widening healthcare inequalities and cohorts of children left behind.
Footnotes
Acknowledgements
The authors thank the Data Linkage Branch of the Western Australia (WA) Department of Health for data linkage and extraction, and client support. They also thank the custodians of the WA Hospital Morbidity and Mental Health Data Collections, the WA Midwives Notification System and the WA Registry of Births, Deaths and Marriages.
Author Contributions
K.M.A. conceived of the study with input from V.A.M. and C.D.; M.P. and P.D.P. planned and conducted the analysis; M.P. wrote the first draft of the manuscript and all authors commented on and approved the final draft.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by grants from the European Research Council (GA682741), the Australian National Health and Medical Research Council (#303235; #458702; APP1002259; APP1080606), March of Dimes (#12-FY04-48; #12-FY07-224), Stanley Foundation and a University of Western Australia Research Collaboration Award.