
Abstract
Current priorities for mental health services include providing treatment and care within a community setting [1]. Various factors complicate treatment and contribute to poor outcomes including lack of adherence to prescribed treatment. One response to non-adherence is the use of legislation based involuntary outpatient commitment (IOC) [2–4]. Involuntary outpatient commitment is a modern development of mental health law introduced as a response to some of the problems arising from deinstitutionalization, specifically that of ‘the revolving door patient’. These patients have been characterized as persistently failing to comply with community treatment and having repeated episodes of illness resulting in involuntary hospitalization [2]. It has been argued that with compulsory treatment such patients spend less time in hospital and experience less intense symptoms and disability [2]. This in turn may enable them to gain more insight into their condition and to make more effective use of community resources [2].
Involuntary outpatient commitment takes the form of community treatment orders (CTOs) within Victoria, Australia. If a patient on a CTO does not adhere to treatment, the order can be revoked and the patient involuntarily hospitalized. Alternately the order may be revoked if the patient is deemed not suitable for community treatment, such as when their mental state has deteriorated to the point where they cannot be safely treated in the community [5]. Community treatment orders have been in use in Victoria for over a decade, with an apparent trend for their increasing use [6]. The authors' experience is that Victorian mental health staff have become accustomed to and experienced in their use and the resistance to the use of CTOs previously reported by Dedman [7] is no longer characteristic. However, IOC has been a subject of considerable controversy outside of Australia [8–12]. From an ethical viewpoint coerced outpatient treatment raises a conflict between meeting the patient's needs and respecting their rights to self-determination [13]. Some have argued that an absolute freedom to refuse treatment is absurd when it is confounded by psychiatric illness resulting in impaired judgement that interferes with the making of reasonable choices about treatment and an inability to care for oneself [4, 12, 14].
Studies of effectiveness of outpatient commitment have yielded limited evidence and many have had methodological problems [2, 15]. It should be noted that there is considerable variation in the types and administration of IOC internationally and this makes generalization of findings difficult. Only two randomized prospective studies have been reported [16, 17]. The decision to randomly discharge to voluntary status patients who were otherwise considered to require IOC has been justified on the basis that it is not really known whether IOC works or not [16]. Such a position is harder to justify in Australia where the majority of clinicians with experience of using CTOs would argue for their effectiveness on the grounds of clinical experience.
Swartz
Steadman
Nearly all other studies have been retrospective and problems such as selection bias, unmeasured variability in treatment and unclear criteria for CTO selection have been evident [2, 16]. Additionally the use of hospital admission rates as the primary outcome measure has been criticized. Other outcomes such as change in symptoms, level of functioning and independence, family attitudes to treatment, degree of burden and risk for the family would also be relevant in assessing the efficacy of involuntary community treatment [15]. With these limitations in mind, findings include reduction in the rates of admission during the period of involuntary outpatient treatment [15,26–33], and in length of stay [15, 26, 28, 29, 32, 34]. Retention in follow-up has been reported to be improved [29,35–37], as has frequency of contact with treating service [15, 31, 37]. Improved compliance with medication [32, 34] and decreased number of emergency service presentations [29] have also been reported. One study found no benefit in terms of rate of readmission or length of stay, but the author qualified his conclusions in light of evidence that the outpatient commitment law was not enforced [38]. Preston
Some clinicians believe that IOC will only have a beneficial impact on medication adherence when depot medication is prescribed [40, 41] and some studies have reported better outcomes when IOC is combined with depot medication [19, 33]. However, depot medications are not suitable for all patients and atypical antipsychotics offer advantages in the treatment of schizophrenia [42–44]. On the basis of their clinical experience the authors are of the opinion that CTOs may enhance adherence with oral medication with some patients. Our first hypothesis was that application of CTOs is associated with reduced relapse rate in patients with schizophrenia and a history of poor treatment adherence. Our second hypothesis was that this effect is not restricted to the use of depot medication but may also be seen for some patients prescribed oral medication.
Method
This is a naturalistic study using a retrospective mirror-image design. The sample was divided into two subgroups to examine the effectiveness of addition of a CTO to treatment. The first subgroup consisted of patients with schizophrenia treated with oral antipsychotic medication while under a CTO (‘oral subgroup’). The second subgroup consisted of patients with schizophrenia treated with depot antipsychotic medication (with or without oral antipsychotic medication in combination) while under a CTO (‘depot subgroup’).
Setting and sample
The study was conducted in three mental health services covering urban and suburban areas in metropolitan Melbourne. Patients suffering from schizophrenia who attended one of the Mental Health Services and who were placed on a CTO at some time between November 1996 and October 1999 were considered eligible for the study. Cases were identified by a manual search of Mental Health Act reports of current and past patients placed on CTOs. The diagnosis of schizophrenia was made by the researchers (D.M., G.I.) using all available information in the clinical files with reference to DSM-IV criteria [45]. Patients with primary diagnoses other than schizophrenia were excluded. In order to provide proportionate duration of comparison conditions within the mirror-image design, patients who were discharged off the CTO before 10 months of such treatment were excluded as were those who had been under the Mental Health Act for more than 6 months during the year prior to a CTO. Patients who had been treated with depot antipsychotic medication for more than 3 months but less than 9 months during the CTO period were excluded as they were considered to have fallen between subgroups. Although the depot subgroup included some patients who were on both oral and depot medication, they were included in the depot group as it was deemed that favourable outcome might be most readily attributed to the depot medication. Those who had been prescribed depot medication for less than 3 months were included within the oral subgroup as it was considered that the fact that they spent the majority of the year on oral medication meant that the outcome for the year would most likely reflect the degree to which they adhered to oral medication. Patients whose files were incomplete and were missing notes from the period under study were excluded. At least six contacts during the year were required but no files had to be excluded on this basis.
Data collection
Data were collected via a retrospective file review for the period of 12 months prior to the date of commencement of the CTO and for the period of 12 months following commencement of that CTO. A questionnaire was used to collect demographic and clinical data, diagnostic data (including inclusion and exclusion criteria), type of prescribed medication, most frequently prescribed dose for the year (in chlorpromazine equivalents) [46], and the total number of contacts with the treating community service including direct and phone contacts. Outcome variables included episodes of relapse indicated by inpatient admissions, episodes of treatment by the crisis team (Crisis Assessment and Treatment Team) and other episodes of relapse documented as defined by need for increase in medication or frequency of contact. No attempt was made to measure treatment adherence directly as it was considered that clinical file notes do not accurately reflect whether patients are taking medication or not when oral medication is prescribed.
A subsample of 10 randomly selected files was reviewed independently by both researchers for the purpose of enabling estimation of interrater reliability.
Data analysis
Data were analysed using SPSS version 9.0 [47]. When comparing subgroups on quantitative variables where data were normally distributed differences between means were tested using Student's
To test the first hypothesis the year prior to commencement of the CTO was used as the control year and the year of the CTO was the experimental year. Data from the two subgroups were combined and analysed using repeated measures tests. As in most instances the distributions of continuous variables were skewed, the Wilcoxon Signed Rank Test was used to determine statistical significance. Where the distribution of data was normally distributed Student's
Results
From the initial sampling frame of 212 patients who were placed on a CTO for at least 10 months during the period of the study, 94 were identified as meeting the inclusion criteria. Sixty-one patients were excluded due to a diagnosis other than schizophrenia, 38 were excluded because the file was unavailable, three were excluded because the file was incomplete, eight were excluded because they had been involuntary patients for at least 6 months of the pre-CTO year and eight were excluded because they were prescribed depot antipsychotic medication for between 3 and 9 months during the CTO year. These 94 patients constituted the total sample. Thirty-one patients (33.0%) met criteria for the oral subgroup while 63 patients (67.0%) met criteria for the depot subgroup.
The main sociodemographic and clinical characteristics of the whole sample and the two subgroups are shown in Table 1. The majority of patients were receiving treatment from community mental health clinics and their oral medication was not routinely supervised.
Demographic and clinical characteristics
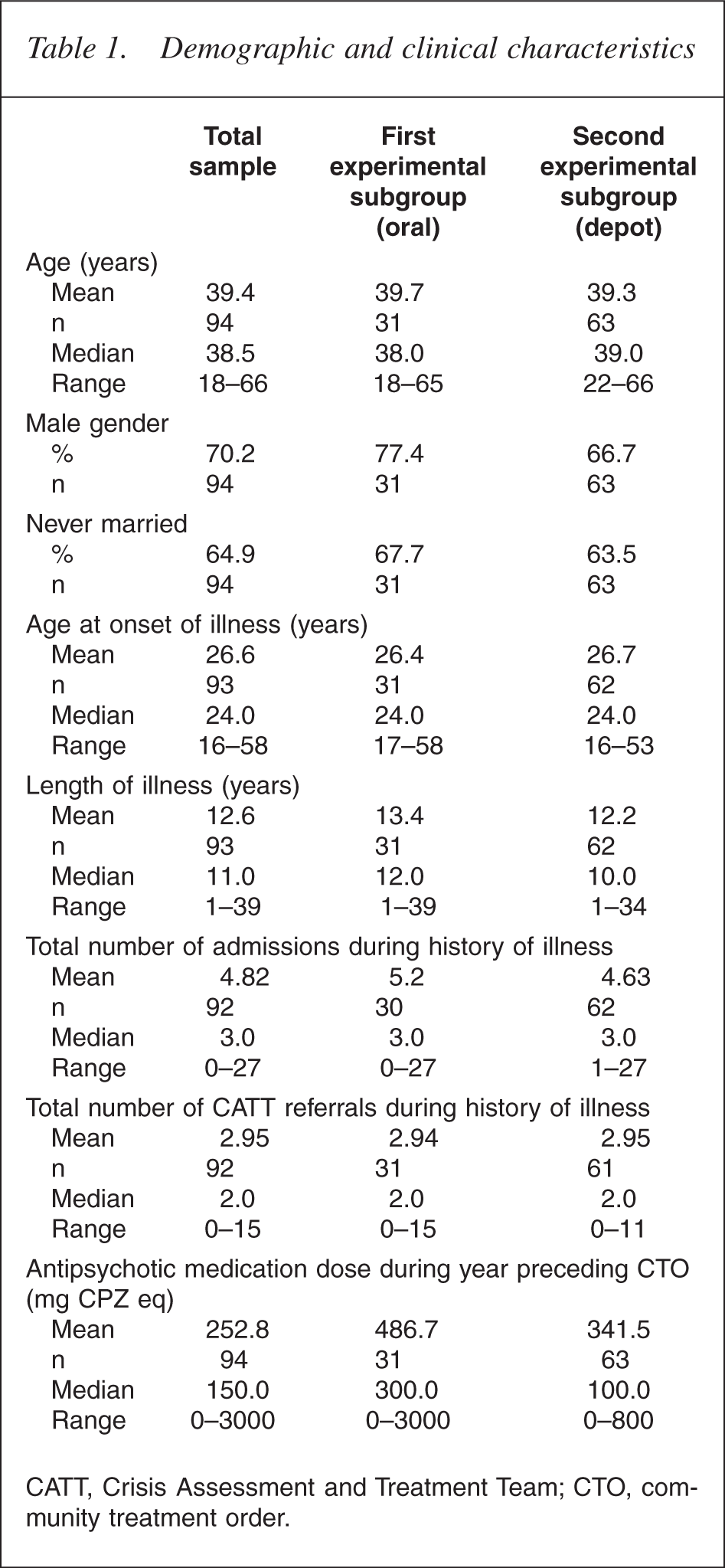
CATT, Crisis Assessment and Treatment Team; CTO, community treatment order.
During the pre-CTO year, 27 patients (28.7%) were receiving no treatment, 15 patients (16.0%) were prescribed oral antipsychotic medication, 25 patients (26.6%) were receiving depot antipsychotic medication and 27 (28.7%) were receiving a combination of depot and oral antipsychotic medication. The mean dose of antipsychotic medication prescribed for the 67 patients who were receiving treatment was 357.7 mg day−1 in chlorpromazine equivalents [46].
Within the total sample 14 patients (14.9%) had a secondary diagnosis of an affective disorder, four (4.3%) had anxiety disorders, five (5.3%) had personality disorder and six (6.4%) had intellectual disability. Sixteen patients (17.0%) had a secondary diagnosis of alcohol misuse and 29 (30.1%) had a diagnosis of other substance use. Two patients (2.1%) had other secondary diagnoses.
Comparison of subgroups
Comparisons between the two subgroups on demographic and clinical variables showed few differences. Within the two subgroups sample populations were normally distributed for age, age at onset and length of illness and there were no significant differences on these variables. There was no significant difference in gender or marital status. The two subgroups did not differ significantly in the total number of admissions they had experienced or the total number of crisis team referrals prior to commencement of the CTO. They were not significantly different when alcohol misuse or other substance misuse was considered. There was a trend towards higher antipsychotic dose in the pre-CTO year for the oral subgroup (Mann–Whitney Z = −1.811, p = 0.07) and a significantly higher dose prescribed to this group in the CTO year (Mann–Whitney Z = −2.608, p = 0.009).
Treatment factors
For the total group the number of contacts the treating community service made with the patients was significantly greater during the year of treatment on CTO (Z = −7.069, p < 0.001). The median dose of antipsychotic medication increased significantly from 250 to 400 mg chlorpromazine equivalents (Z = −4.405, p < 0.001) but the extremes of dose range decreased during the year of the CTO (see Table 2).
Treatment factors and outcome variables in total sample
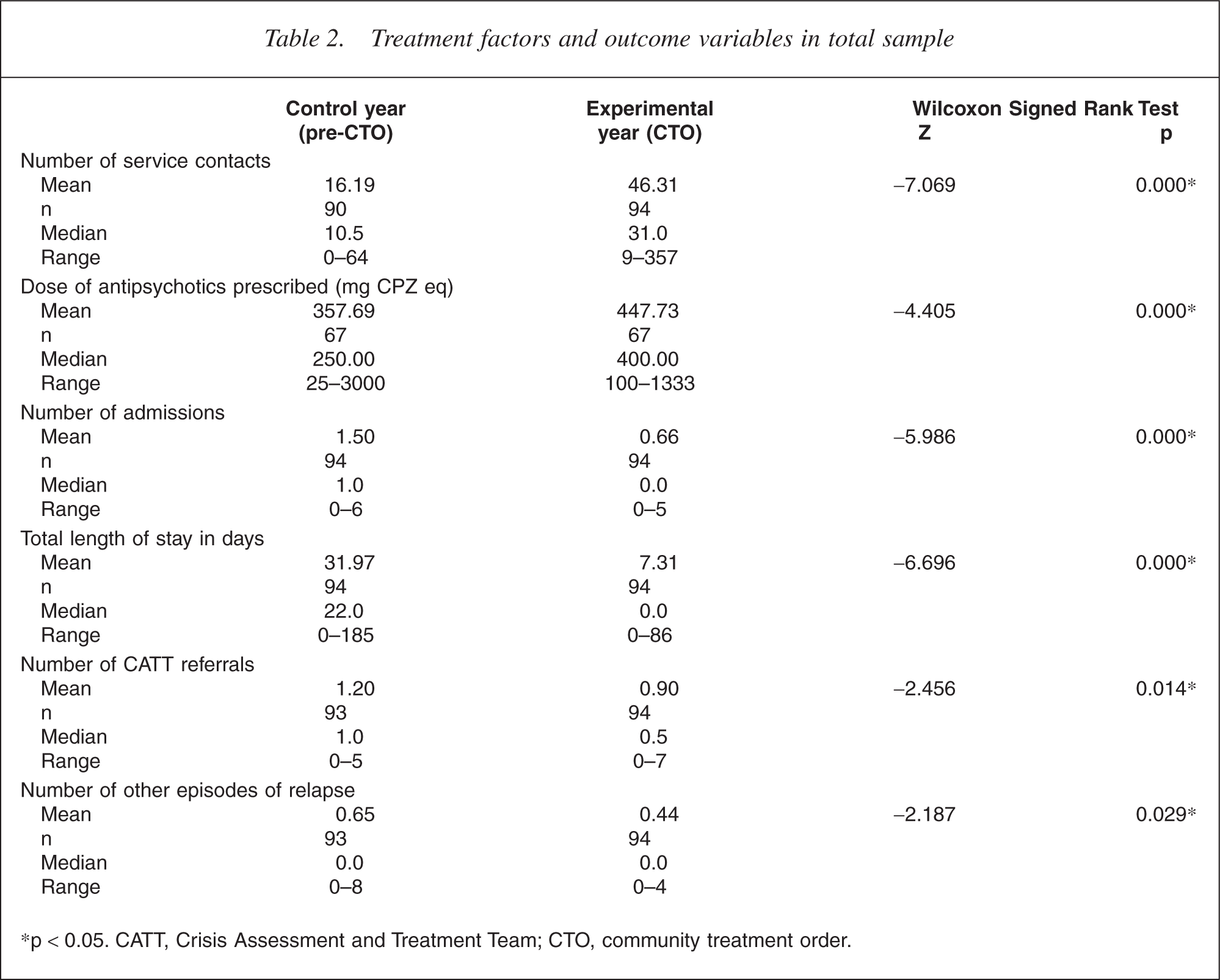
∗p < 0.05. CATT, Crisis Assessment and Treatment Team; CTO, community treatment order.
For the oral subgroup the number of contacts between the treating community service and the patients were significantly increased in the CTO year (Z = −3.682, p < 0.001) (see Table 3 for details). The median dose of antipsychotic medication was significantly increased from the pre-CTO to the CTO year (Z = −2.332, p = 0.020).
Treatment factors and outcome variables in first experimental subgroup (oral antipsychotic medication)
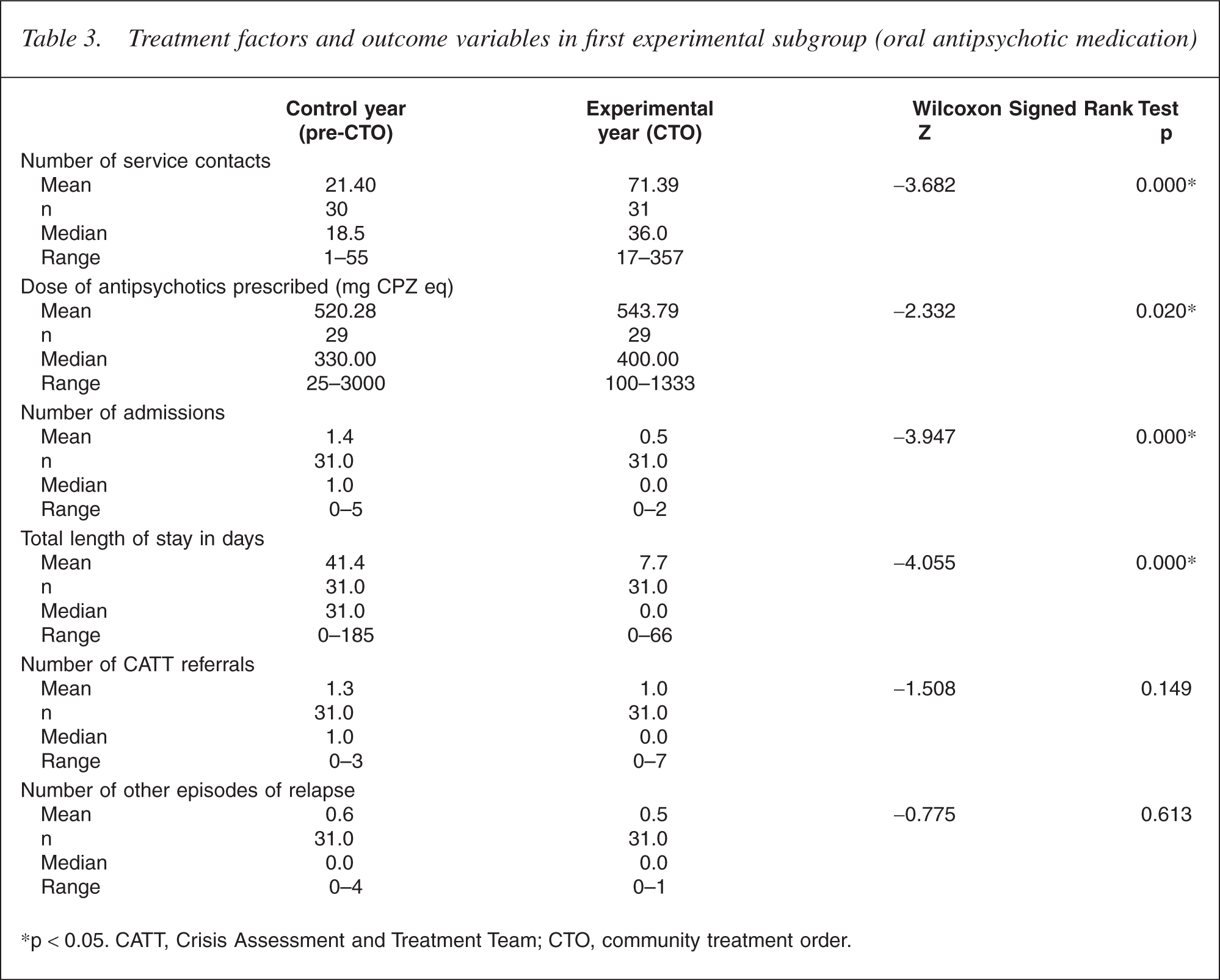
∗p < 0.05. CATT, Crisis Assessment and Treatment Team; CTO, community treatment order.
Similar results were found for the depot subgroup (see Table 4 for details). Contacts with the treating community team were significantly increased in the year of treatment on CTO (Z = −6.040, p < 0.001) and there was also a significant increase in the median dose of antipsychotic medication prescribed (Z = −3.766, p < 0.001). The median dose of antipsychotic medication prescribed during treatment on CTO was significantly higher for the oral compared with the depot subgroup (Z = −2.595, p = 0.009).
Treatment factors and outcome variables in second experimental subgroup (depot or combined antipsychotic medication)
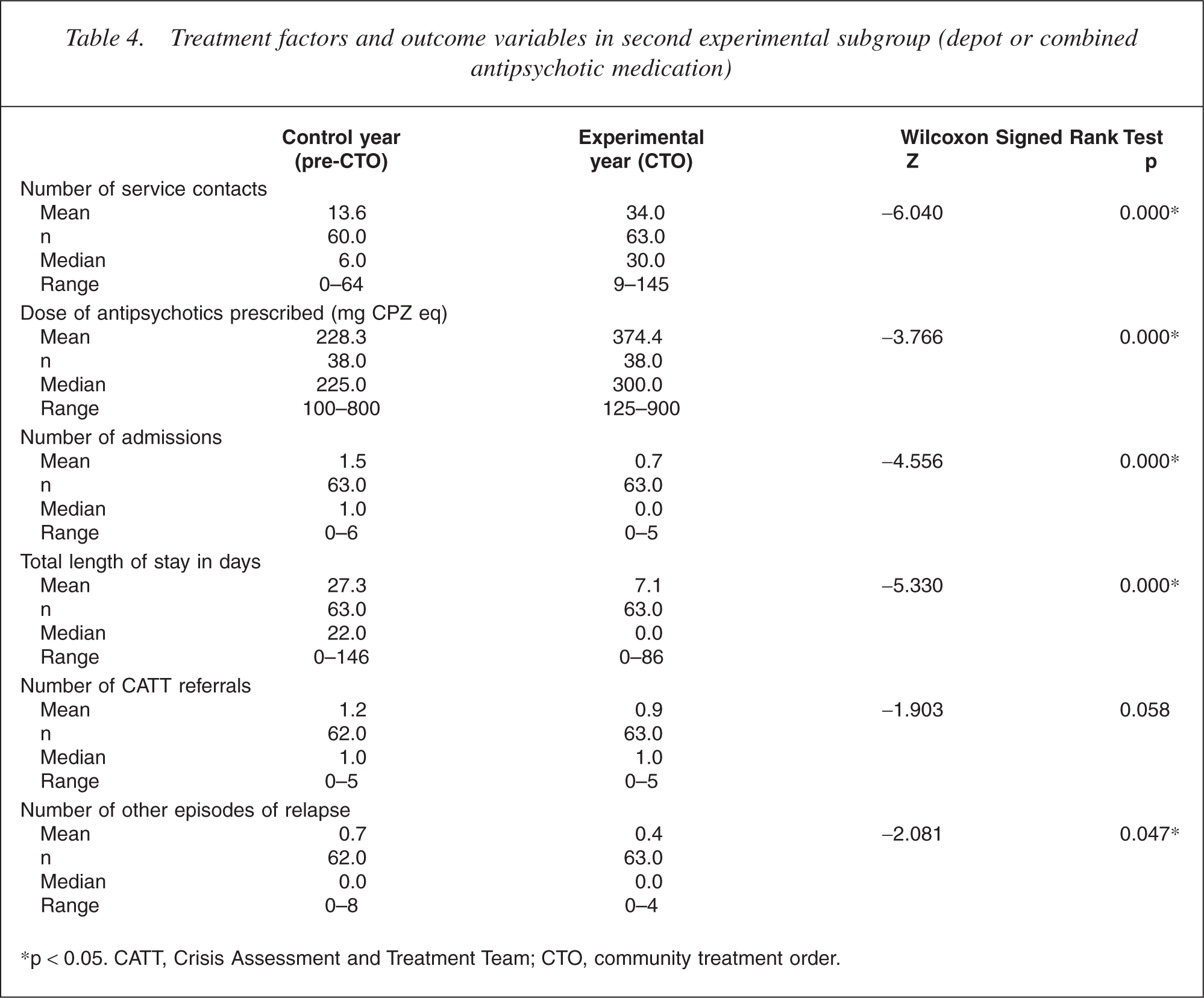
∗p < 0.05. CATT, Crisis Assessment and Treatment Team; CTO, community treatment order.
Outcome
Total group
There were significant differences between the control year and the CTO year for the total sample (see Table 2). The number of admissions was significantly reduced following the introduction of the CTO (Z = −5.986, p < 0.001) as was the total length of stay in hospital for the year (Z = −6.696, p < 0.001). Significant reductions were also seen in the number of crisis team referrals (Z = −2.456, p = 0.014) and the number of other relapses recorded (Z = −2.187, p = 0.029) when comparing the pre-CTO year with the CTO year.
Subgroups
The number of admissions during the CTO year was significantly reduced for both the oral subgroup (Mann–Whitney Z = −3.947, p < 0.001) and the depot subgroup (Mann–Whitney Z = −4.556, p < 0.001) (see Tables 3,4 for details). Similarly total length of stay during hospital admissions was reduced for both subgroups (Mann– Whitney Z = −4.055, p < 0.001 and Mann–Whitney Z = −5.330, p < 0.001, respectively).
The number of crisis team referrals during the year of treatment with the CTO was not significantly different for either subgroup when compared with the pre-CTO year although the depot subgroup showed a non-significant trend (Mann–Whitney Z = −1.903, p = 0.058) towards fewer crisis team referrals. Similarly the comparison of other episodes of relapse recorded in the pre-CTO and CTO years showed significant results for the depot subgroup (Mann–Whitney Z = −2.081, p = 0.047) but no significant difference for the oral subgroup (Mann–Whitney Z = −0.775, p = 0.613).
Interrater reliability
Interrater reliability was assessed on a number of measures. This was good for number of admissions during year prior to CTO (Kappa = 1.0), number of admissions during year of CTO (Kappa = 0.6), length of stay during year of CTO (Kappa = 0.4) and other episodes of relapse during CTO year (Kappa = 0.6). Reliability was poor for some of the measures. These included total number of hospital admissions (Kappa = 0.048), total number of crisis team referrals (Kappa = −0.4), number of crisis team referrals during year prior to CTO (Kappa = 0.0), number of crisis team referrals during year of CTO (Kappa = 0.2), length of stay during year prior to CTO (Kappa = 0.2), average dose of antipsychotic medication during CTO year (Kappa = 0.2) and other episodes of relapse prior to CTO year (Kappa = −0.2).
Discussion
This study addresses an issue that continues to excite interest and controversy within the psychiatric profession: the ongoing debate as to the effectiveness and ethicalness of involuntary treatment [2, 6, 8, 11, 12, 48]. Our results strengthen the case for the effectiveness of IOC in enhancing the outcome of treatment of selected patients with schizophrenia. There were significant decreases in number of admissions and total length of inpatient stay when comparing the year of treatment on CTO with the preceding year for the whole sample and for both subgroups. This is consistent with previous research [15, 18,26–29,31–34]. It indicates that these patients spent more time in their chosen living circumstances in the community suggesting a better quality of life and potentially counterbalancing the infringement of liberty that the CTO represents. This could be seen as consistent with the principle established in the Victorian Mental Health Act [5] of providing the least restrictive alternative treatment. It also represents a substantial reduction in resource consumption by the patients treated with CTOs. Further, our findings extend those of other studies in demonstrating a significant reduction in episodes of relapse-related community treatment (crisis team referrals and other episodes of documented relapse) during treatment on CTO.
A few previous studies have reported an advantage when prescribing depot antipsychotic medication to patients on CTOs [21, 33]. In this study significant reductions in readmissions and length of stay associated with treatment on CTO were found irrespective of whether patients were treated with depot or oral medication. This supports the notion that outcome can be positively influenced for selected patients even when compliance with prescribed medication cannot be directly observed by mental health professionals. Further, it challenges the notion that involuntary outpatient treatment needs to be combined with depot medication [40, 41].
There is insufficient previous research to draw firm conclusions about the types of patients who might benefit from a CTO. This study provides an overview of some of the characteristics of a subgroup of patients who received such treatment from three metropolitan mental health services, remembering that the study only included patients with schizophrenia and the sample was further limited by other exclusion criteria. The majority of patients had a lengthy illness and most had experienced multiple admissions. They were predominantly male; perhaps reflecting the greater degree of psychosocial disability commonly suffered by males with schizophrenia. Most were unmarried and unemployed; factors that suggest substantial psychosocial disability. Similar characteristics of patients in whom CTO use might be appropriate have been identified elsewhere [49], along with a history of repeated violence to others and a history of non-adherence with treatment. Non-adherence was likely to be a feature of our sample as suggested by the observation that a number of the patients were not in treatment prior to the admission that culminated in commencement of the CTO. Some patients had become disengaged from treatment services despite a past history of illness. It can be speculated that this was likely associated with a lack of insight into the need for treatment, a factor commonly considered as contributing to a need for involuntary treatment.
There were significant increases in the number of contacts with the treating community services for all patients on a CTO. This was a measure of the process of treatment and is in line with the findings of other studies [29, 37]. The greater contact that occurred might well have been associated with improvement in those specific outcome measures that demonstrated change following implementation of the CTO. Both subgroups also showed an increase in the number of treatment contacts. Concern has sometimes been expressed that a CTO may be used as a substitute for more assertive follow-up, particularly when depot medication is prescribed. It has been argued that with the CTO enforcing compliance, other aspects of treatment such as psychoeducation and rehabilitation are not seen as necessary. Our finding on the process of treatment suggests that this is not the case within this study and suggests that CTOs are a means of enabling assertive follow-up rather than an alternative to it. In reviewing his experience with outpatient coercion, Geller has stated his opinion that for some patients both coercion and adequate mental health services are necessary but not in themselves sufficient to enable successful living in the community [30]. This is further supported by the findings of Swartz
There are a number of limitations of this study to consider when interpreting the findings. The retrospective design, with reliance on data recorded in clinical files, raises several problems. It is well recognized that data in clinical files may be inaccurate and certain events may be underreported. There was also potential for assessor bias because assessment of the clinical files was not blind to the medication prescribed. To minimize this, objective numerical data were recorded whenever possible and the outcome data were chosen with this in mind. The comparison of ratings on the same files by different researchers shows varying levels of interrater reliability. Low Kappas were found more commonly in the pre-CTO year than in the CTO year suggesting the possibility that documentation is done more clearly when a patient is on a CTO. The Kappas also tended to be lower with measures involving large numbers such as total length of stay and average dose of antipsychotic medication during a year. Another area where interrater reliability was comparatively low was numbers of crisis team referrals. This likely reflects the lack of a consistent method of filing crisis team referrals used by some of the services involved in the study; it was noted by one researcher that these were sometimes indicated only by references within the progress notes rather than by specific referral documentation.
The use of a mirror-image design has limitations, despite its acceptance as a reasonable means of controlling in retrospective studies of IOC [15,26–28,35, 51]. A patient's clinical condition and life circumstances may have varied between the control and the experimental year, regardless of the implementation of the CTO. A further limitation was the relatively low number of cases, particularly in the oral medication subgroup, resulting from relatively few patients being treated with oral medication and CTOs within the study area at the time of the study. A contributing factor to the low number of patients was the relatively high number excluded because the file could not be found in time for assessment. It is possible that these patients might have varied from the patients whose files could be found in terms of clinical characteristics or outcome. Unfortunately it was not possible to address this issue due to the lack of alternate sources of clinical information in the absence of the file. This likely contributed to selection bias.
A further limitation was that there were some patients who had both oral and depot medication during the CTO year in both subgroups. Patients who were on both oral and depot medication in the depot subgroup and those who had been on depot medication for less than 3 months, but on oral medication for the rest of the year, in the oral subgroup. The decision to do this was made to avoid ambiguity about which medication type was most likely related to the observed outcome. It is acknowledged that medication regimes are often complicated and vary over time such that many patients could not readily be fitted into categories of depot or oral medication only. This resulted in some patients being excluded in the attempt to generate discrete subgroups but also possibly contributed to selection bias.
It should be remembered that this was a naturalistic study and was not primarily designed to enable direct comparisons of the outcome of the two subgroups. The purpose was to assess whether the use of IOC could enhance outcome for patients treated with either oral or depot antipsychotic medication. It is difficult to draw conclusions about differences in outcome between the two subgroups because differences in the characteristics of patients may have influenced clinicians in their decision about which medication to prescribe, resulting in unmatched subgroups. Although these two subgroups appeared similar on most demographic and clinical variables considered, it is possible that more patients in the oral subgroup may have had treatment resistant illness as suggested by higher doses of prescribed medication before and during the period of the CTO. In view of this it is not reasonable to draw any conclusions as to whether either treatment is more effective than the other. In order to more directly compare the effectiveness of these two treatment strategies a study would need to use a prospective randomized allocation to treatment type using a sample group that might be considered appropriate for either type of treatment.
Conclusion
This study provides further evidence to support the effectiveness of CTOs as a means of enhancing outcome for certain people with schizophrenia. There was some evidence of improvements in outcome occurring for those patients who were treated with oral medication while on a CTO, as well as for those patients treated with depot medication. This suggests that clinicians might consider the prescription of oral rather than depot antipsychotic medication when planning management for the patient requiring involuntary community treatment. This offers some hope for improved outcomes for patients given the advantages that atypical antipsychotic medications can offer over the use of traditional depot medications. There is also the challenge for clinicians of providing appropriately supportive management to facilitate success of such treatment. It is becoming increasingly evident that for best outcome, involuntary community treatment needs to be combined with assertive and sometimes intensive management. Further research is required to understand better the comparative effectiveness of oral versus depot medication when used for patients on CTOs. It would also be valuable to identify better the characteristics of those patients who are likely to do well when prescribed oral antipsychotics, and what level of support they might need to facilitate this.